Cardiology
Asking for Preferences
Basic to advanced cardiology one by one
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Here is Lesson 1: Cardiology from the Ground Up - covering anatomy, muscle physiology, and the cardiac action potential.
🫀 Cardiology - Lesson 1: Heart Anatomy & Cardiac Muscle Physiology
Source: Guyton & Hall Textbook of Medical Physiology | Goldman-Cecil Medicine
1. Overall Structure of the Heart
The heart has 4 chambers arranged in two pumping circuits:
| Side | Receives | Pumps To | Purpose |
|---|---|---|---|
| Right Atrium | Deoxygenated blood (SVC + IVC) | Right Ventricle | Collects systemic venous return |
| Right Ventricle | From RA | Pulmonary Artery → Lungs | Pulmonary (low-pressure) circuit |
| Left Atrium | Oxygenated blood (4 pulmonary veins) | Left Ventricle | Receives pulmonary return |
| Left Ventricle | From LA | Aorta → Body | Systemic (high-pressure) circuit |
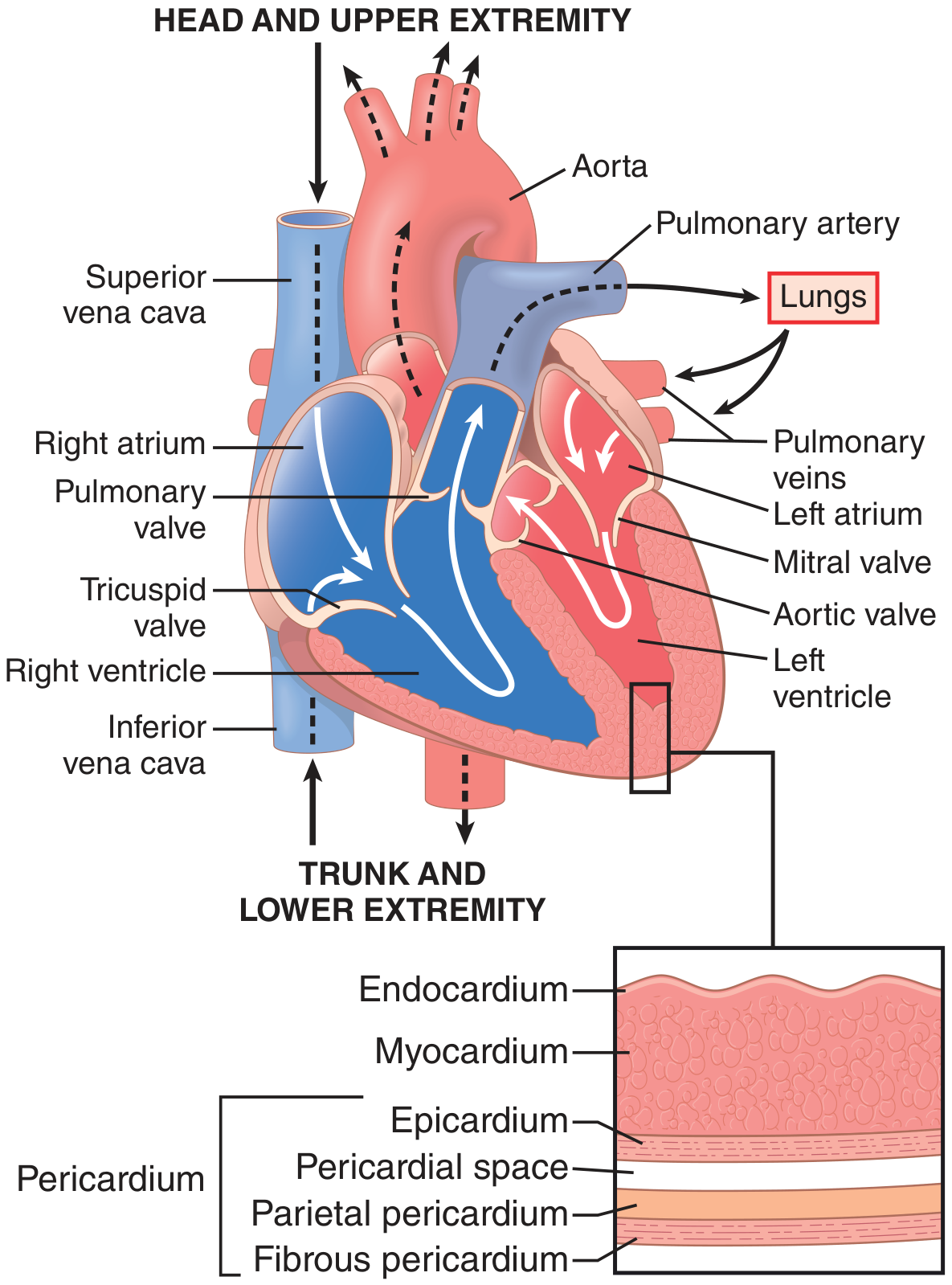
The 4 Valves
- Tricuspid valve - between RA and RV (3 leaflets)
- Pulmonary valve - between RV and pulmonary artery
- Mitral valve - between LA and LV (2 leaflets, bicuspid)
- Aortic valve - between LV and aorta
All valves are passive - they open and close purely based on pressure gradients. The tricuspid and mitral (AV) valves are tethered by chordae tendineae attached to papillary muscles, which prevent leaflet prolapse (regurgitation) during systole.
Wall Layers (inside to outside)
- Endocardium - smooth inner lining
- Myocardium - the muscular wall (thickest in the LV)
- Epicardium - outer visceral layer
- Pericardial space - fluid-filled (prevents friction)
- Pericardium (parietal then fibrous layers)
2. Cardiac Muscle - What Makes It Unique
Cardiac muscle is striated like skeletal muscle, but behaves very differently:
Key Structural Feature - The Syncytium
Cardiac muscle cells (cardiomyocytes) are connected end-to-end by intercalated discs, which contain gap junctions. Gap junctions allow ions to flow freely between cells, meaning an action potential in one cell spreads instantly to ALL neighboring cells.
- The atria form one syncytium
- The ventricles form a separate syncytium
- They are electrically separated by fibrous tissue (the AV node is the only normal bridge)
This "all-or-none" behavior means: either the whole atria contract, or none of them do - same for the ventricles.
Excitation-Contraction Coupling
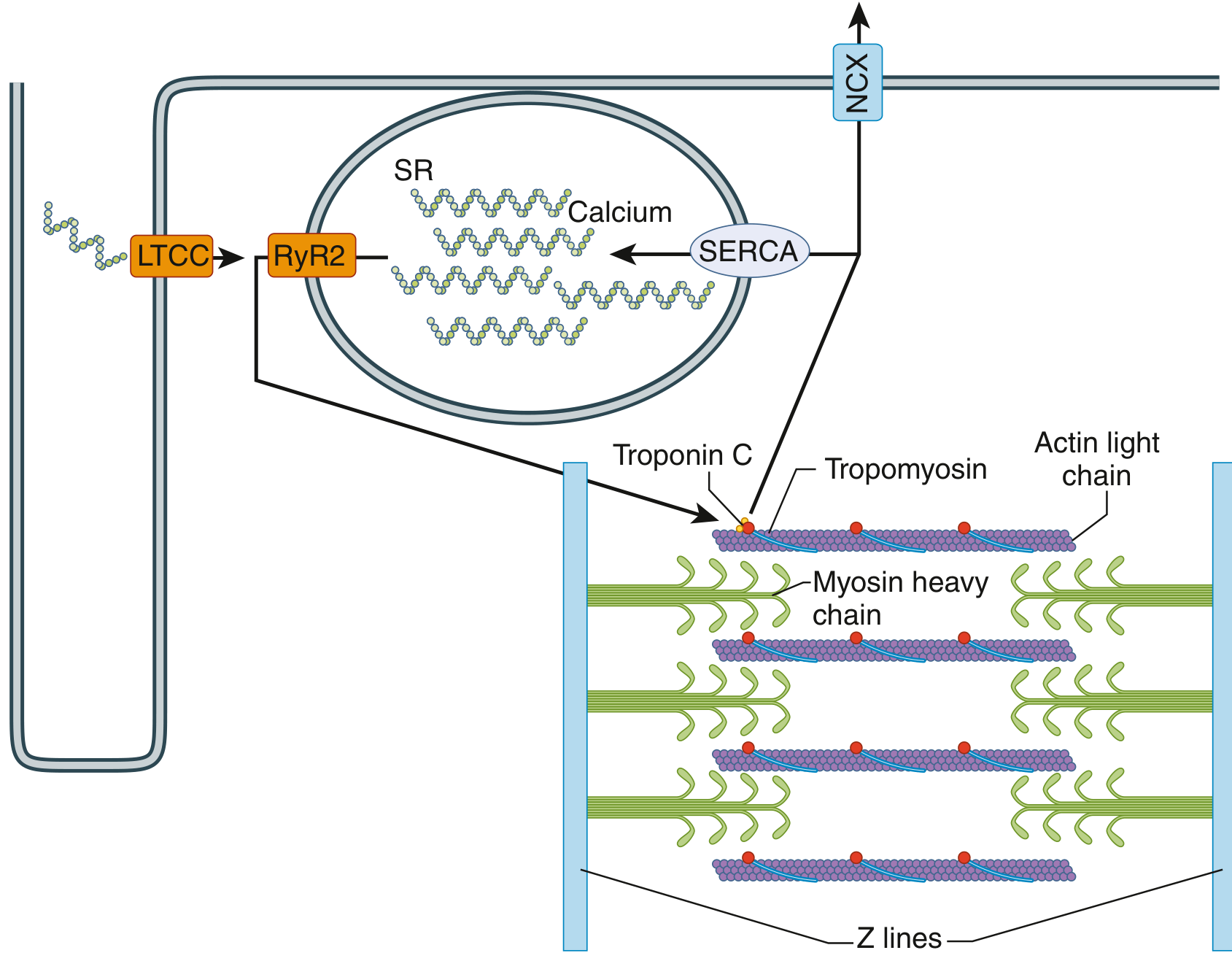
Step by step:
- Action potential depolarizes the cell membrane
- L-type calcium channels (LTCC) open → small Ca²⁺ influx
- This triggers ryanodine receptors (RyR2) on the sarcoplasmic reticulum (SR)
- Massive Ca²⁺ release from SR ("calcium-induced calcium release")
- Ca²⁺ binds Troponin C → conformational change in Tropomyosin
- Myosin heads can now bind Actin → cross-bridge cycling → contraction
- Relaxation: Ca²⁺ pumped back into SR by SERCA and out of cell by NCX
3. The Cardiac Action Potential
The ventricular action potential has 5 phases, and lasts ~200-300 ms (vs. skeletal muscle at ~2 ms):
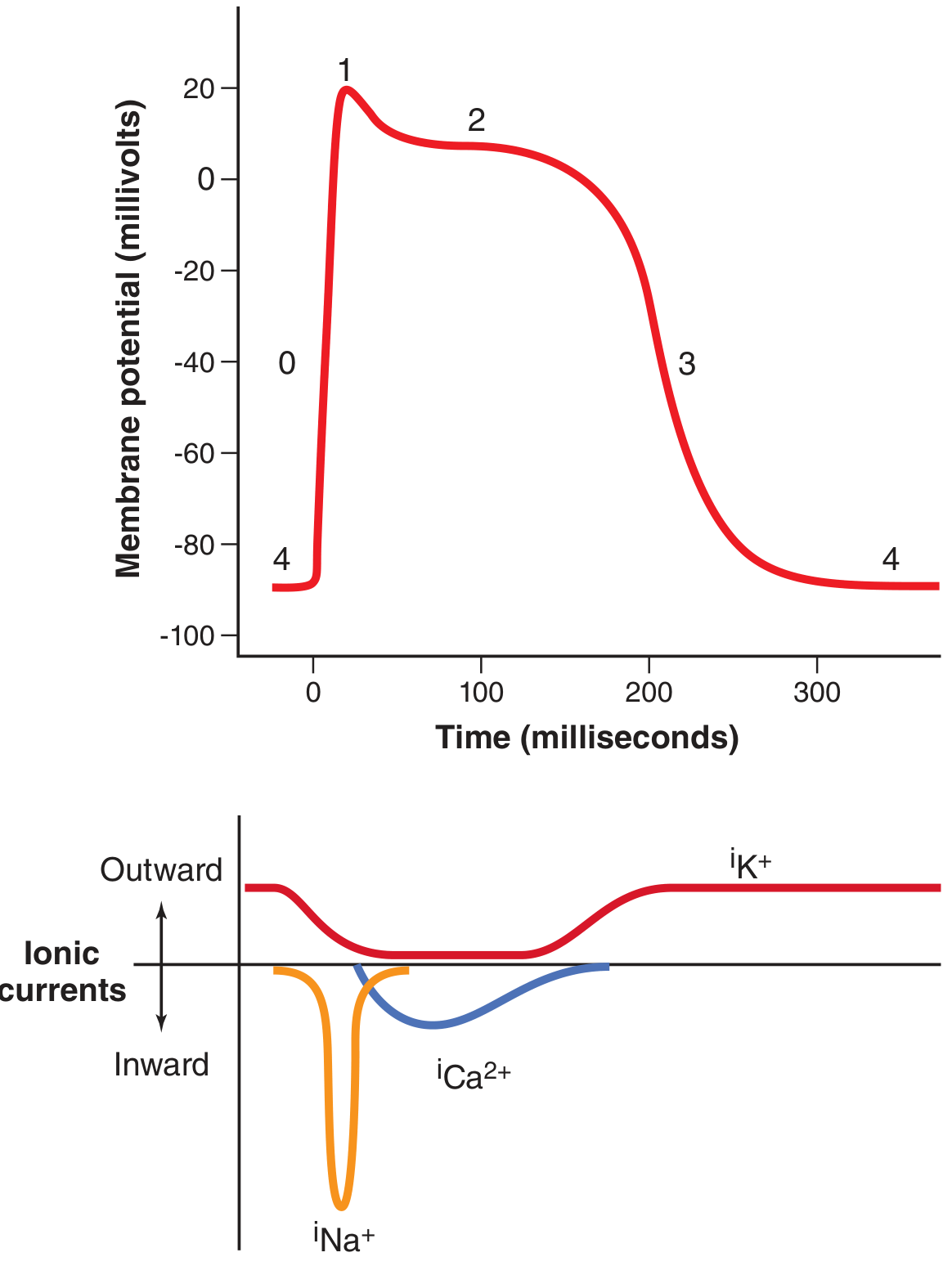
| Phase | Name | What Happens | Ion Movement |
|---|---|---|---|
| Phase 4 | Resting membrane potential | Cell at rest | -85 mV; K⁺ channels open |
| Phase 0 | Rapid depolarization | Fast Na⁺ channels open | Na⁺ rushes IN → -85 to +20 mV |
| Phase 1 | Early repolarization | Fast Na⁺ channels close; transient K⁺ out | Brief dip |
| Phase 2 | Plateau | L-type Ca²⁺ channels open | Ca²⁺ (+ some Na⁺) IN; K⁺ outflow reduced |
| Phase 3 | Rapid repolarization | Ca²⁺ channels close; K⁺ channels open fully | K⁺ OUT → returns to -85 mV |
Why does the plateau exist?
Two reasons unique to cardiac muscle:
- Slow L-type Ca²⁺ channels open and stay open for ~200 ms, prolonging depolarization
- K⁺ permeability drops sharply at the start of the action potential, reducing the repolarizing force
The plateau has a critical protective function - it creates a long refractory period (~250 ms), which prevents the heart from going into tetanic (sustained) contraction the way skeletal muscle can. This is essential - a tetanic heart would not fill with blood and would stop pumping.
4. Coronary Blood Supply (Introduction)
The heart feeds itself first. Coronary arteries arise from the aorta just above the aortic valve:
- Right coronary artery (RCA) - supplies RV, inferior LV, SA and AV nodes
- Left anterior descending (LAD) - supplies anterior LV, apex, anterior septum ("widow maker")
- Left circumflex (LCx) - supplies lateral LV wall
Key physiology: Coronary flow to the subendocardium occurs predominantly during diastole - because during systole, the contracting myocardium compresses intramural vessels. This is why tachycardia (shortened diastole) can cause subendocardial ischemia even with normal coronary arteries.
Factors that increase coronary flow (up to 6x): nitric oxide, adenosine, bradykinins, prostaglandins, CO₂.
Summary - What to Remember from Lesson 1
- Right heart = pulmonary circuit (low pressure); Left heart = systemic circuit (high pressure)
- Cardiac muscle is a syncytium - gap junctions make it "all-or-nothing"
- Ca²⁺ is the trigger for contraction: LTCC → RyR2 → SR release → Troponin C
- The action potential plateau (Phase 2) prevents tetany and enables Ca²⁺ entry
- Coronary subendocardial flow happens mainly in diastole
Ready for Lesson 2? We'll cover the cardiac conduction system - SA node, AV node, Bundle of His, Purkinje fibers, automaticity, and how the ECG is generated. Just say "next" or "continue."
This is a shared conversation. Sign in to Orris to start your own chat.