Tmj joint disorders
Reading File
Finding Sources
Searching PubMed
"temporomandibular joint disorders"[MeSH Terms] AND management
Searching the Web
TMJ temporomandibular joint disorders classification diagnosis treatment 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a thorough overview of TMJ disorders:
Temporomandibular Joint (TMJ) Disorders
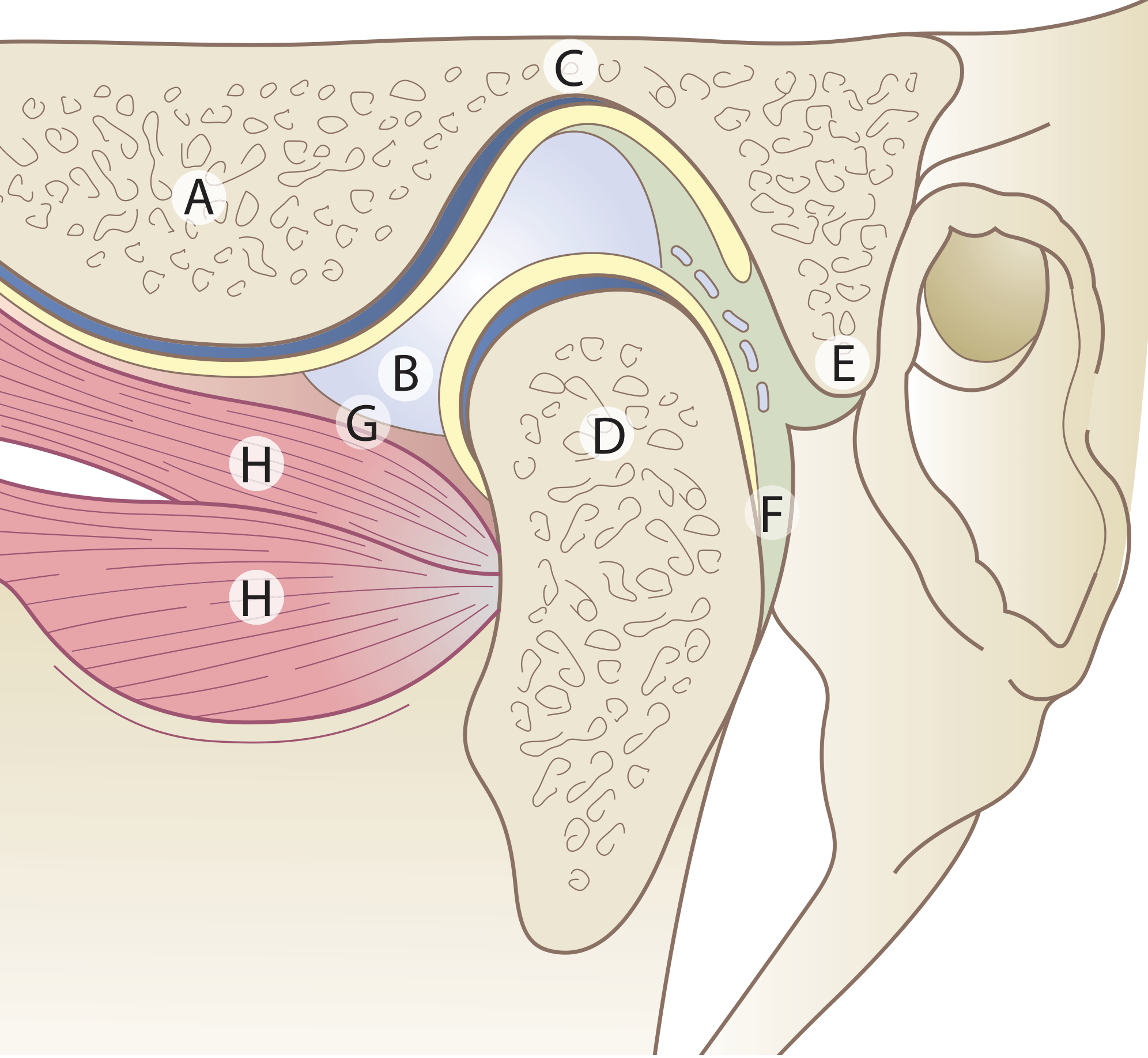
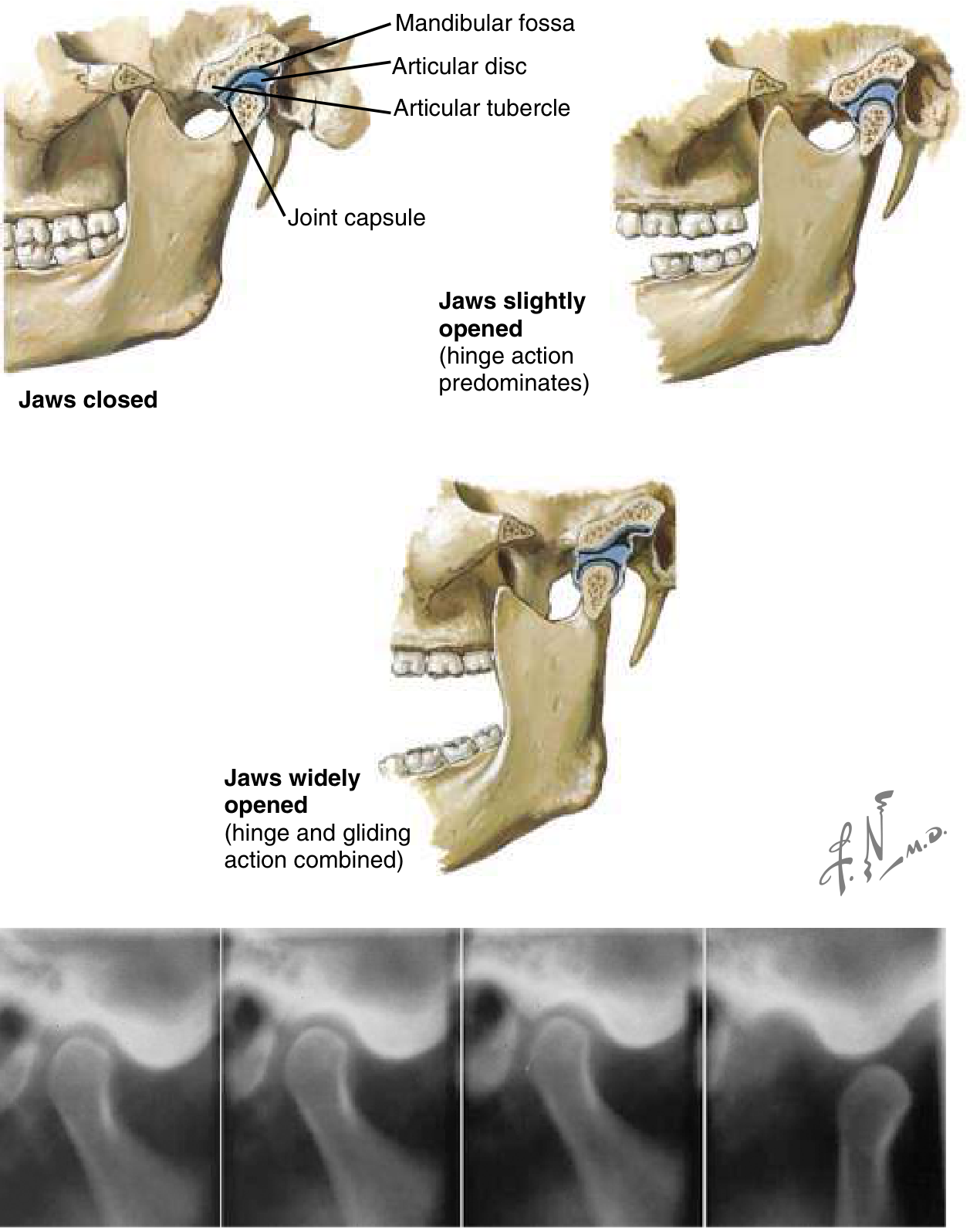
Anatomy of the TMJ
The TMJ is a synovial joint formed by the mandibular (glenoid) fossa of the temporal bone articulating with the mandibular condyle. It has several unique features:
- The joint space is divided into upper and lower cavities by an intra-articular fibrocartilaginous disc
- Articular surfaces are covered by fibrous tissue (not hyaline cartilage), reflecting the joint's intramembranous development
- Permits both gliding (upper compartment) and hinge (lower compartment) movements
- A secondary condylar cartilage is present in the condyle head until adolescence
- Joint movements are directly influenced by the occlusion of teeth
Definition and Terminology
Temporomandibular disorders (TMD) is a collective term for clinical problems involving:
- The masticatory muscles
- The TMJ itself and associated structures
In 1934, James Costen first described the TMJ as a cause of facial and head pain ("Costen syndrome"). TMD is most prevalent between ages 35-45, after which spontaneous resolution is often seen.
Classification / Types
The Diagnostic Criteria for TMD (DC/TMD) organizes disorders into:
1. Muscle Disorders
- Myalgia (most common) - local or regional muscle pain
- Myositis - muscle inflammation
- Tendonitis
- Spasm
- Myofascial pain dysfunction (MPD) syndrome
2. Joint (Intracapsular) Disorders
- Internal derangement - disc displacement (with or without reduction)
- Degenerative joint disease (osteoarthritis)
- Rheumatoid arthritis involving the TMJ
- Infectious arthritis
- Ankylosis (fibrous or bony)
- Mandibular dislocation (condyle locks anterior to articular eminence)
- Condylar hyper- or hypoplasia
- Condylar osteolysis
- Fractures
Etiology and Risk Factors
The exact cause of TMD is debated. Contributing factors include:
- Bruxism (teeth grinding) and clenching - especially stress-related
- Chronic gum chewing
- Emotional stress causing masticatory muscle fatigue and spasm
- Malocclusion and mandibular malalignment (though less commonly causative than once thought; tooth malocclusion is now considered a rare etiology unless resulting from a specific event like dental work)
- Loss of teeth or ill-fitting dentures
- Inflammatory arthritis (RA, psoriatic arthritis)
- Dystonic drug reactions (can cause dislocation)
- Anatomic disharmony between fossa and articular eminence
- Hypermobility of the capsule and TMJ ligaments
Clinical Features
TMD is defined as: "aching in the muscles of mastication, sometimes with occasional brief severe pain on chewing, often associated with restricted jaw movement and clicking or popping sounds."
Cardinal Symptoms
| Feature | Description |
|---|---|
| Pain | Preauricular/facial pain, worse with jaw movement and mastication |
| Joint sounds | Clicking, popping, or crepitus on range of motion |
| Limited mouth opening | Restricted mandibular movement, trismus |
| Referred pain | Ear, eye, head, face, neck muscles |
| Muscle tenderness | Masseter, temporalis, pterygoid muscles on palpation |
| Headache | Often frontal or temporal |
Key Diagnostic Criteria (from Bradley & Daroff's Neurology)
- Pain directly related to jaw movements and mastication
- Tenderness in masticatory muscles or over the TMJ on palpation
- Anesthetic blocking of tender structures confirms the pain source
- Sudden change in occlusal relationship of teeth
- Restriction or interference with mandibular movement (clicking, incoordination, crepitus)
Differential Diagnosis
- Otitis media / externa (mimics TMJ ear pain)
- Sinusitis
- Dental pain (pulpitis, root abscess, cracked tooth syndrome)
- Trigeminal neuralgia
- Cervicogenic headache
- Migraine
- Parotid gland disorders
- Tumors of the jaw or skull base
- Neuromuscular disorders
Investigations
- Clinical examination is the cornerstone (palpation, range of motion, auscultation)
- Radiographs: panoramic X-ray (OPG), TMJ-specific views
- MRI: gold standard for soft tissue - best for disc position and displacement
- CT scan: best for bony pathology (degenerative changes, ankylosis, fractures)
- Laboratory studies: ESR, RF, ANA (if inflammatory arthritis suspected)
Imaging should not be used alone for diagnosis, nor as the primary determinant for surgical intervention. - Cummings Otolaryngology, p. 1637
Management
Step 1 - Conservative (First-Line, should be tried for at least 3-6 months)
| Treatment | Details |
|---|---|
| Soft/mechanically modified diet | Reduces loading on joint |
| Local heat application | Relaxes masticatory muscles |
| NSAIDs | Anti-inflammatory and analgesic |
| Cyclobenzaprine (muscle relaxant) | Given at bedtime |
| Occlusal splints | Night guards/bite plates; proven benefit up to 6 months |
| Isometric jaw exercises | Jaw opening, lateral deviation, thrusting exercises |
| Behavioral modification | Jaw relaxation, stress reduction |
| Physical therapy | Improves range of motion |
Occlusal adjustment and splints have been shown to improve TMJ syndrome and can be used up to 6 months. - Textbook of Family Medicine 9e, p. 914
Step 2 - Intermediate Treatments (if conservative fails)
- Botulinum toxin injections: Recent 2024 meta-analysis (PMID 38483856) supports effectiveness for pain reduction in TMD
- Low-level laser therapy (LLLT): Systematic reviews (2024-2025) show benefit over TENS and therapeutic ultrasound for pain and function
- Hyaluronate intra-articular injections: Insufficient evidence per older data; recent reviews ongoing
- Cognitive behavioral therapy and biofeedback
Step 3 - Surgical (only after failure of nonsurgical therapy + imaging evidence of pathology)
Absolute indications for surgery:
- Neoplasms
- Growth abnormalities
- Ankylosis
Relative indications:
- Pain and dysfunction refractory to conservative management
- Confirmed pathology on imaging
- Significant compromise in quality of life
Surgical options (in order of invasiveness):
-
Arthrocentesis (least invasive)
- Office-based, under IV sedation + local anesthesia
- Two 18-gauge needles inserted into superior joint space
- Performs lysis, lavage with Ringer lactate, and can inject anti-inflammatory agents
- Success rate: 70-90% for pain reduction and improved range of motion
- A 2024 network meta-analysis (PMID 39294620) confirms arthrocentesis as effective
-
Arthroscopy
- Surgical suite, general anesthesia
- Allows direct visualization of the superior joint space
- Lysis, lavage, and limited operative procedures
- Success rate: 80-90%
-
Open joint surgery (arthroplasty)
- Disc repositioning and repair, condylotomy, or total joint replacement
- Reserved for severe structural pathology refractory to lesser interventions
Surgery is indicated when pain or dysfunction is refractory to nonsurgical therapy and quality of life is significantly compromised. It is rarely performed in isolation and must be supported by pre- and post-surgical therapy. - Cummings Otolaryngology, p. 1637
Special Situation: TMJ Dislocation
When the condyle travels anterior to the articular eminence and locks there:
- Masseter, internal pterygoid, and temporalis muscles go into spasm (trismus)
- Condyle cannot return to the temporal fossa
- Bilateral dislocation is more common (jaw opens but cannot close)
- Unilateral dislocation: jaw deviates to the opposite side
- Risk factors: ligament weakness, capsule laxity, drug-induced dystonic reactions, prior dislocation episodes
Management of dislocation:
- Manual reduction (intraoral technique with downward and posterior pressure on posterior teeth)
- Pre-treatment with benzodiazepine or muscle relaxant helps
- Consider prolotherapy or eminectomy for recurrent cases
Recent Evidence (2024-2025)
| Evidence | Finding | PMID |
|---|---|---|
| Systematic review + meta-analysis | Botulinum toxin is effective for TMD pain | 38483856 |
| Cochrane review | Limited evidence for occlusal interventions alone | 39282765 |
| Network meta-analysis | Arthrocentesis effective for pain and function | 39294620 |
| Systematic review | LLLT superior to TENS and ultrasound in TMD | 35315745 |
| Systematic review (2025) | Low-level laser therapy reduces pain in RCTs | 40096874 |
Key Takeaways
- TMD is a broad group of conditions involving the joint, muscles, and related structures - not a single diagnosis
- Most cases (>80%) resolve with conservative management; avoid rushing to surgery
- Always exclude serious causes (tumors, inflammatory arthritis, neurological disorders) before diagnosing TMD
- The neurological evaluation should confirm pain is directly related to jaw use, with confirmatory anesthetic block when needed
- Imaging (preferably MRI) is required before any surgical decision, but should not drive treatment alone
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 693 | Rosen's Emergency Medicine (9e), p. 873 | Cummings Otolaryngology Head & Neck Surgery, p. 1637 | Bradley and Daroff's Neurology in Clinical Practice, p. 2473 | Textbook of Family Medicine 9e, p. 914
This is a shared conversation. Sign in to Orris to start your own chat.