I now have comprehensive data from all sources. Let me compile the complete 30-mark MD Anaesthesia PG exam answer.
Autonomic Nervous System (ANS) - Anaesthesia-Relevant Anatomy & Physiology, and Changes During Anaesthesia
Sources: Barash's Clinical Anesthesia 9e (Chapter 14) | Braunwald's Heart Disease | Guyton & Hall | Ganong's Physiology | Katzung's Pharmacology
SECTION 1 - FUNCTIONAL ANATOMY OF THE ANS
The ANS is the part of the CNS and peripheral nervous system concerned with the involuntary regulation of cardiac muscle, smooth muscle, and glandular and visceral functions. It maintains homeostasis through two major divisions and a third (enteric) system.
Central Autonomic Organisation
The hypothalamus is the highest integrating centre of the ANS. It coordinates:
- Anterior hypothalamus: parasympathetic functions (heat dissipation, cardiodeceleration)
- Posterior/lateral hypothalamus: sympathetic functions (heat conservation, the "defence reaction")
Other central centres:
- Nucleus tractus solitarius (NTS): primary integration of baroreceptor and chemoreceptor afferents
- Rostral ventrolateral medulla (RVLM): main vasomotor centre; maintains resting sympathetic tone
- Dorsal motor nucleus of vagus: parasympathetic outflow to thoracic and abdominal viscera
- Locus coeruleus: noradrenergic nucleus; modulates arousal and sympathetic tone
- Periaqueductal grey (PAG): descending modulation of pain and ANS activity
Peripheral ANS Organization - The Two-Neuron Arc
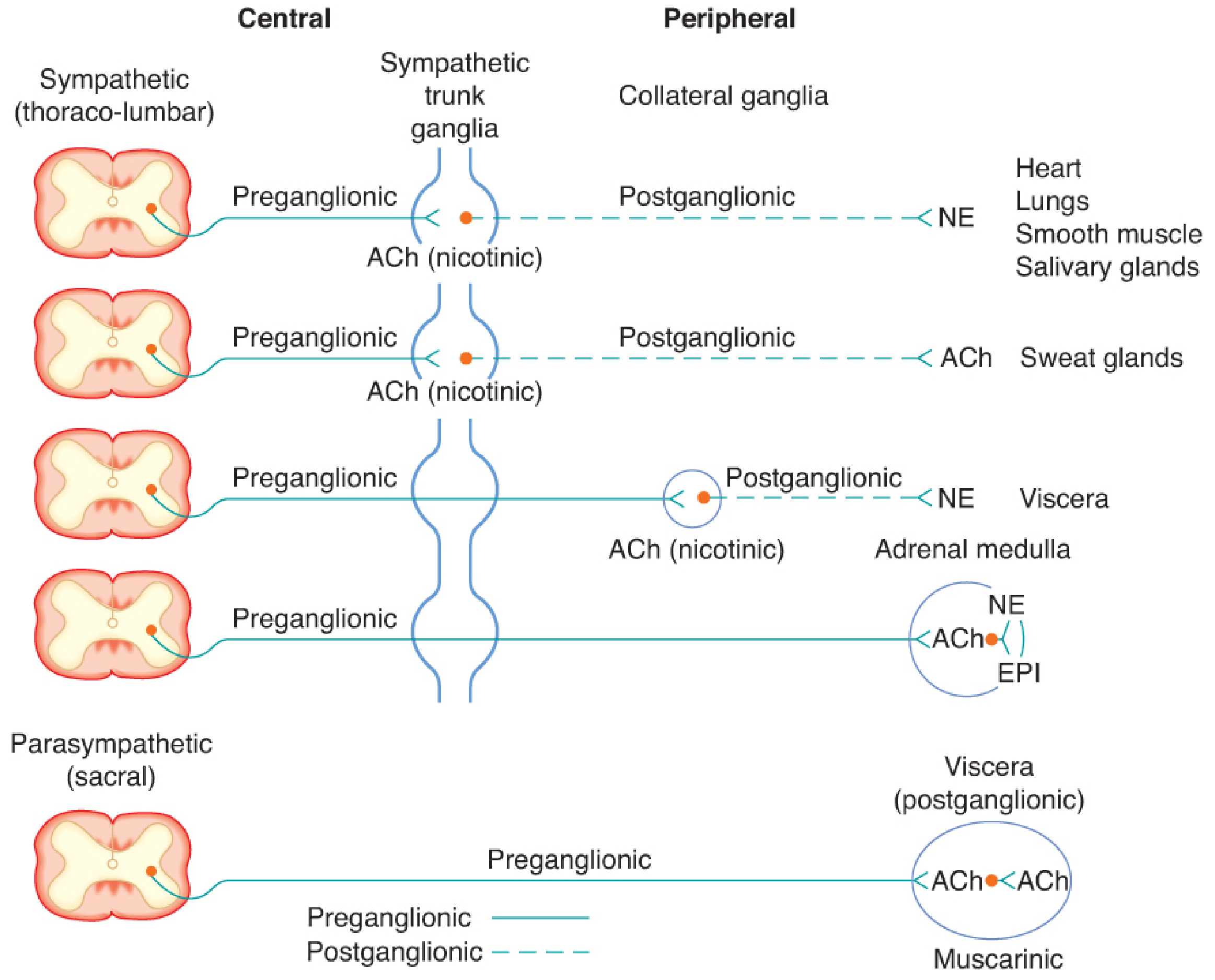
All ANS efferent pathways consist of two neurons in series:
- Preganglionic neuron: cell body in CNS → myelinated (B fibre) → synapse in ganglion
- Postganglionic neuron: cell body in ganglion → unmyelinated (C fibre) → effector organ
SECTION 2 - SYMPATHETIC NERVOUS SYSTEM (SNS)
Anatomy
| Feature | Detail |
|---|
| Origin | Intermediolateral grey column of spinal cord, T1-L3 |
| Alternative name | Thoracolumbar division |
| Preganglionic fibre | Short, myelinated (B-fibre), 3mm diameter; speed 3-15 m/s |
| Ganglia location | Paravertebral chain (22 paired ganglia) OR unpaired collateral ganglia (celiac, superior/inferior mesenteric) |
| Postganglionic fibre | Long, unmyelinated (C-fibre); speed <2 m/s |
| Divergence ratio | 1 preganglionic → many postganglionic → diffuse, widespread response |
| Neurotransmitter | Pre: ACh (nicotinic receptor); Post: Norepinephrine (adrenergic receptors) |
| Exception 1 | Sweat glands and sympathetic vasodilator fibres: postganglionic releases ACh |
| Exception 2 | Adrenal medulla - directly innervated by preganglionic fibers; chromaffin cells (modified postganglionic neurons) release 80% EPI + 20% NE directly into blood |
Sympathetic Chain - Three Courses of Preganglionic Fibre
- Synapse in ganglia at level of exit
- Course up/down the chain to synapse at other levels
- Pass through chain without synapsing → prevertebral (collateral) ganglia
Key Sympathetic Ganglia and Clinical Relevance
| Ganglion | Level | Relevant Anaesthesia Point |
|---|
| Cervicothoracic (Stellate) | C7-T1 | Stellate block for CRPS, arrhythmias, Horner's syndrome when blocked |
| Celiac plexus | T12-L1 (prevertebral) | Celiac plexus block for upper abdominal cancer pain |
| Superior hypogastric plexus | L5-S1 | Pelvic pain procedures |
SECTION 3 - PARASYMPATHETIC NERVOUS SYSTEM (PNS)
Anatomy
| Feature | Detail |
|---|
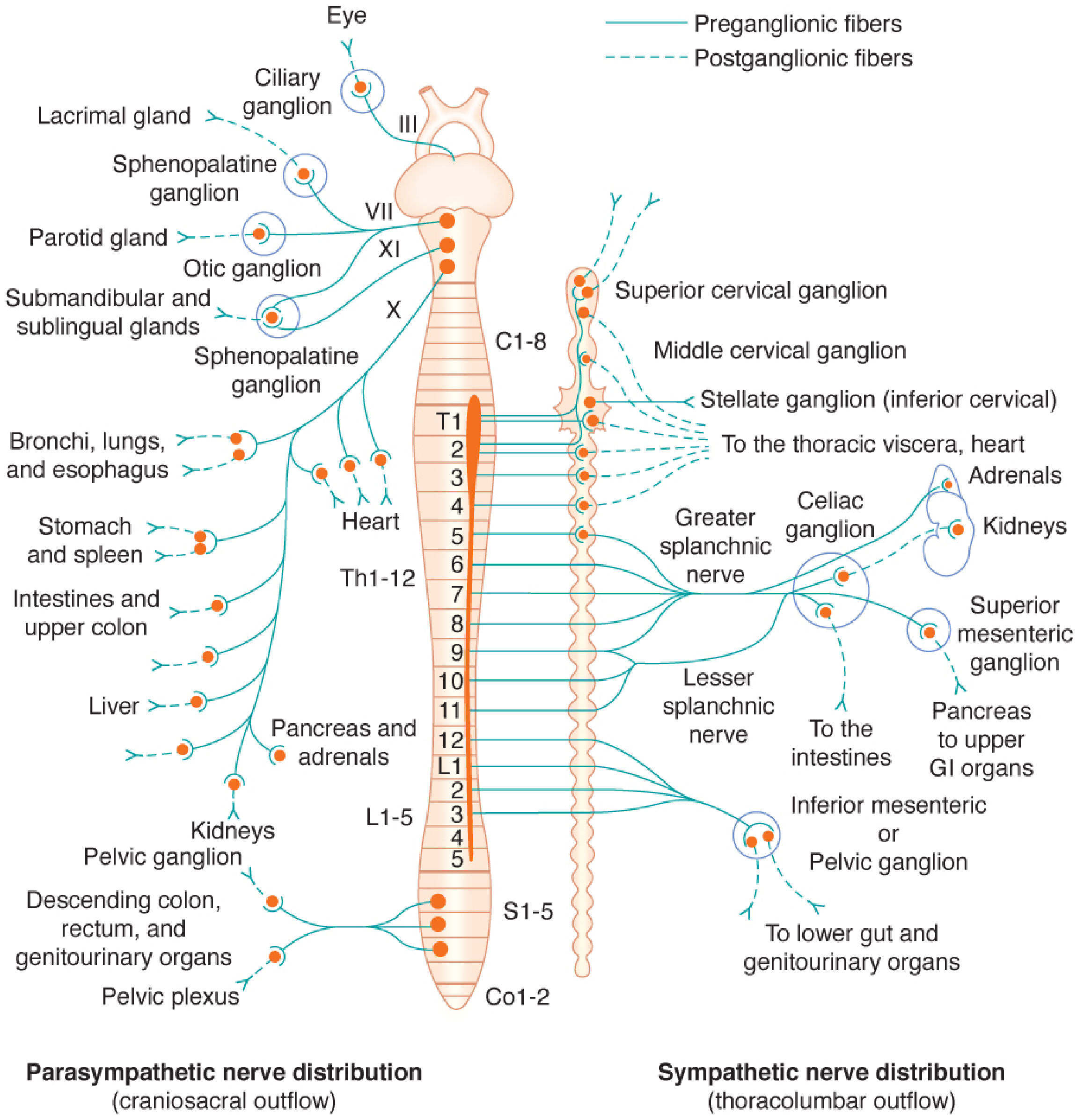
| Origin | Craniosacral outflow: CN III, VII, IX, X + S2-S4 |
| Alternative name | Craniosacral division |
| Preganglionic fibre | Long, myelinated; synapse near or within the target organ |
| Postganglionic fibre | Very short, unmyelinated |
| Convergence | Limited distribution → discrete, localised responses |
| Neurotransmitter | Pre: ACh (nicotinic); Post: ACh (muscarinic receptors) |
Cranial Parasympathetic Outflow
| Nerve | Ganglion | Target |
|---|
| CN III (Oculomotor) | Ciliary ganglion | Pupil constriction (miosis), accommodation |
| CN VII (Facial) | Pterygopalatine + Submandibular ganglia | Lacrimal, nasal, salivary glands |
| CN IX (Glossopharyngeal) | Otic ganglion | Parotid gland |
| CN X (Vagus) | Ganglia in/near organs | Heart, lungs, GI tract to splenic flexure - 75% of all PNS activity |
Sacral Parasympathetic Outflow (S2-S4)
- Via pelvic splanchnic nerves (nervi erigentes)
- Innervates: descending colon, rectum, bladder, genitalia
- Mediates erection (NO-mediated); bladder detrusor contraction
SECTION 4 - NEUROTRANSMITTERS AND RECEPTORS
Cholinergic Neurotransmission (ACh)
Synthesis: Choline + Acetyl-CoA → ACh (enzyme: Choline acetyltransferase)
Storage: Synaptic vesicles
Release: Ca²+-dependent exocytosis
Degradation: Acetylcholinesterase (AChE) → choline + acetic acid (choline recycled)
Cholinergic Receptors
| Receptor | Type | Location | Effect | Antagonist |
|---|
| Muscarinic M1 | GPCR (Gq) | Brain, gastric glands | CNS excitation, acid secretion | Atropine |
| Muscarinic M2 | GPCR (Gi) | Heart (SA, AV nodes) | ↓HR, ↓conduction velocity | Atropine |
| Muscarinic M3 | GPCR (Gq) | Smooth muscle, glands | Bronchoconstriction, secretion, GI motility | Glycopyrrolate |
| Nicotinic Nn | Ligand-gated ion channel (α3β4) | Autonomic ganglia | Ganglionic transmission | Hexamethonium, trimethaphan |
| Nicotinic Nm | Ligand-gated ion channel (α1β1δε) | Neuromuscular junction | Muscle contraction | Neuromuscular blockers |
Anaesthetic note: Volatile anaesthetics and ketamine potently inhibit both ganglionic (α3β4) and CNS (α4β2) nicotinic receptors.
SLUDGE (Muscarinic Stimulation Mnemonic)
Salivation, Lacrimation, Urination, Defecation, GI cramps, Emesis
Adrenergic Neurotransmission (NE/EPI)
Catecholamine Synthesis Pathway:
Tyrosine → DOPA → Dopamine → Norepinephrine → Epinephrine
(tyrosine hydroxylase - rate-limiting step)
Termination of action: Primarily by neuronal reuptake (Uptake 1) back into the nerve terminal; metabolised by MAO (intraneuronal) and COMT (extraneuronal).
Adrenergic Receptors - Comprehensive Table
| Receptor | Coupling | Location | Effect | Clinical Use |
|---|
| α1 | Gq → IP3/DAG → ↑Ca²+ | Peripheral vascular smooth muscle, myocardium, urethral sphincter | Vasoconstriction, +inotropy (minor), urinary retention | Phenylephrine (vasopressor) |
| α2 (pre) | Gi → ↓cAMP | Presynaptic terminals | Inhibit NE release (negative feedback) | Clonidine, dexmedetomidine |
| α2 (post) | Gi → ↓cAMP | CNS, coronaries, platelets | Sedation, analgesia, ↓MAC, platelet aggregation | Dexmedetomidine: ICU sedation |
| β1 | Gs → ↑cAMP → PKA | SA node, AV node, myocardium, kidneys (JGA) | ↑HR, ↑Inotropy, ↑Dromotropy, ↑Renin | Dobutamine (cardiac surgery) |
| β2 | Gs → ↑cAMP → PKA | Bronchial, vascular, uterine smooth muscle; liver | Bronchodilation, vasodilation, glycogenolysis, uterine relaxation | Salbutamol, terbutaline |
| β3 | Gs | Adipose tissue, bladder | Lipolysis, bladder relaxation | - |
| DA1 | Gs | Renal, mesenteric, coronary vessels; renal tubule | Vasodilation, natriuresis, diuresis | Dopamine at 2-5 µg/kg/min, Fenoldopam |
| DA2 | Gi | Presynaptic sympathetic terminals | ↓NE release, secondary vasodilation | - |
Receptor Up/Down-Regulation (Clinically Important)
- Downregulation: Prolonged exposure to agonist → internalization of receptors → tachyphylaxis. E.g., chronic heart failure → β1 receptor downregulation (reduced inotropic response to catecholamines)
- Upregulation: Chronic antagonist use → increased receptor numbers. E.g., chronic β-blocker therapy → up to 100% increase in β receptor numbers → β-blocker withdrawal syndrome (acute discontinuation = unopposed α stimulation + increased β receptors)
- Clinical implication: Clonidine withdrawal follows the same mechanism
SECTION 5 - ANS REFLEXES (ANAESTHETIC RELEVANCE)
Baroreceptor Reflex
Pathway:
↑BP → Stretch of carotid sinus (CN IX) / aortic arch (CN X)
→ Nucleus Tractus Solitarius (NTS) in medulla
→ ↑Vagal tone (↓HR) + ↓Sympathetic vasomotor tone
→ BP returns to normal
| Component | Location | Relevance |
|---|
| High-pressure sensors | Carotid sinus (CN IX), Aortic arch (CN X) | Major baroreceptors |
| Low-pressure sensors | Atria, pulmonary vessels, ventricles (Bainbridge reflex) | Volume sensing |
| Integration centre | NTS in medulla → RVLM → dorsal vagal nucleus | Drug targets (dexmedetomidine acts here) |
| Effectors | SA node (HR), peripheral vasculature (SVR) | Main cardiovascular determinants |
Anaesthetic significance: Most anaesthetic agents blunt the baroreceptor reflex, explaining the haemodynamic instability seen during induction. Degree of blunting: Volatile agents > Propofol > Ketamine (maintains baroreflex).
Chemoreceptor Reflex
- Peripheral: Carotid and aortic bodies (hypoxia, hypercapnia, acidosis) → ↑Ventilation + ↑Sympathetic tone
- Central: Medullary chemoreceptors (CO2/H+) → ↑Ventilation
- Volatile agents and opioids depress peripheral chemoreceptor response to hypoxia
Bainbridge Reflex
- Atrial stretch receptor activation (volume overload) → reflex tachycardia via vagal afferents
- Competes with baroreceptor reflex; the net HR response depends on the dominant reflex at the time
Bezold-Jarisch Reflex
- Stimulation of ventricular C-fibres (serotonin, capsaicin, ischaemia) → bradycardia + hypotension + vasodilation (triad)
- Mechanism: Vagal efferent activation + sympathetic withdrawal
- Clinical relevance: Paradoxical bradycardia with spinal anesthesia, hypovolaemia in upright position, can cause vasovagal syncope
SECTION 6 - DIFFERENTIAL AUTONOMIC EFFECTS ON ORGANS
| Organ | Sympathetic | Parasympathetic | Dominant Tone |
|---|
| Heart (SA node) | ↑HR (β1) | ↓HR (M2) | Parasympathetic (resting HR <100 due to vagal tone) |
| Heart (contractility) | +Inotropy (β1, β2) | Minimal | Sympathetic |
| Coronary arteries | Constriction (α1) / Dilation (β2, metabolic) | Dilation | Metabolic autoregulation |
| Peripheral vessels | Constriction (α1) | None (except vasodilator fibres in vessels) | Sympathetic |
| Bronchi | Bronchodilation (β2) | Bronchoconstriction (M3) | Parasympathetic |
| GI tract | ↓Motility, ↑sphincter tone (α) | ↑Motility, ↓sphincter tone (M) | Parasympathetic |
| Bladder detrusor | Relaxation (β2) | Contraction (M3) | Parasympathetic |
| Bladder sphincter | Contraction (α1) | Relaxation | Sympathetic |
| Pupil | Dilation - mydriasis (α1, dilator pupillae) | Constriction - miosis (M3, sphincter pupillae) | Equal tone |
| Salivary glands | Thick, viscid saliva (α) | Profuse, watery saliva (M) | Parasympathetic |
| Sweat glands | Diaphoresis (ACh via sympathetic!) | None | Sympathetic (cholinergic) |
| Adrenal medulla | EPI + NE release | None | Sympathetic |
| Liver | Glycogenolysis (α + β) | Glycogen synthesis | Sympathetic |
| Kidney | ↑Renin (β1), vasoconstriction | None | Sympathetic |
| Eye ciliary muscle | Relaxation - far vision (β) | Contraction - near vision/accommodation (M3) | Parasympathetic |
SECTION 7 - CHANGES IN ANS DURING ANAESTHESIA
This is the most important section for an MD Anaesthesia exam.
A. PREOPERATIVE / STRESS RESPONSE
Before induction, surgical anxiety activates the HPA axis and SNS:
- ↑Plasma catecholamines (NE and EPI)
- ↑HR, ↑BP, ↑cardiac output
- Pupil dilation, dry mouth, diaphoresis
- Premedication with midazolam, alpha-2 agonists (dexmedetomidine, clonidine) attenuates this
B. INDUCTION OF ANAESTHESIA
Propofol
- Strong SNS depression: reduces muscle sympathetic nerve activity (MSNA)
- Blunts baroreceptor reflex → ↓SVR and ↓HR → significant hypotension
- Reduces cardiac output
- Mechanism: facilitates GABA-A, inhibits NE release centrally
Thiopentone/Barbiturates
- Inhibits sympathetic outflow from brainstem (reduces MSNA)
- Blunts baroreflex → hypotension
- Despite lower BP, reflex tachycardia may be seen (baroreceptors partly functional)
- Mechanism: GABA-A potentiation + direct myocardial depression
Etomidate
- Cardiovascular stability: minimal effect on SNS
- Does NOT significantly blunt baroreceptor reflex
- Neither heart rate nor blood pressure change significantly
- Drug of choice in haemodynamically unstable patients
Ketamine - Unique Dissociative Profile
- Indirect sympathomimetic: inhibits reuptake of NE into sympathetic nerve terminals → ↑plasma catecholamines
- Net effect: ↑HR, ↑BP, ↑cardiac output, ↑SVR, ↑myocardial O2 demand
- Centrally: direct myocardial depression (masked by SNS stimulation in healthy patients)
- Important: In catecholamine-depleted patients (e.g., prolonged haemorrhagic shock, burns), the direct myocardial depressant effect is unmasked → cardiovascular collapse possible
- Baroreflex maintained with ketamine (unlike most agents)
- S(+)-ketamine: increases MSNA despite ↑BP; racemic ketamine does not significantly increase generalised SNS outflow
Midazolam/Benzodiazepines
- Mild SNS depression
- Minimal baroreceptor blunting
- Cardiovascular stability maintained
C. LARYNGOSCOPY AND TRACHEAL INTUBATION
This represents the most powerful acute sympathetic stimulus in routine anaesthesia:
Mechanism:
- Mechanical stimulation of pharynx/larynx → afferents via CN IX, X
- Activates NTS → massive sympathetic discharge
- Releases EPI and NE from adrenal medulla and sympathetic terminals
- Response: ↑HR (up to 30-50%), ↑MAP (up to 20-30 mmHg), ↑intracranial pressure, ↑intraocular pressure
At-risk patients: Coronary artery disease, cerebrovascular disease, aortic aneurysm, hypertensive patients
Attenuation strategies:
| Drug | Mechanism | Dose |
|---|
| Opioids (fentanyl 2-3 µg/kg) | Central sympatholytic + blunts laryngeal reflexes | Pre-induction |
| Lidocaine IV (1.5 mg/kg) | Blunts laryngeal afferents | 90s before laryngoscopy |
| Esmolol (1-2 mg/kg) | β1 blockade | Pre-induction bolus |
| Labetalol | α+β blockade | |
| Dexmedetomidine (0.5-1 µg/kg) | α2 agonist - central sympatholysis | Pre-induction infusion |
| Clonidine | α2 agonist | Premedication |
| Deep anaesthesia | ↑volatile concentration | Must balance against cardiovascular depression |
D. VOLATILE ANAESTHETIC AGENTS
All volatile agents cause dose-dependent depression of sympathetic nervous activity:
| Agent | Primary ANS Effect | Baroreceptor Effect | HR Effect | BP Effect | Special Feature |
|---|
| Halothane | ↓SNS activity; ↑vagal tone | Markedly blunted | Bradycardia | ↓↓↓BP | Sensitizes myocardium to catecholamines → arrhythmias; do NOT use with epinephrine |
| Enflurane | ↓SNS activity | Blunted | ↑HR (reflex) | ↓↓BP | Less sensitization to catecholamines than halothane |
| Isoflurane | ↓SNS activity (central); ↓SVR | Blunted | ↑HR (reflex tachycardia due to ↓BP) | ↓↓BP | Dilates coronary vasculature |
| Sevoflurane | ↓SNS activity | Moderately blunted | Minimal change | ↓BP (less than isoflurane) | Safest for bronchospasm; cardiac conduction stable |
| Desflurane | ↓SNS activity at steady state | Special: rapid ↑ in concentration → acute SNS stimulation → ↑HR, ↑BP (catecholamine surge) | Tachycardia with rapid ↑ | Transient ↑BP with rapid ↑ | "Sympathetic response to desflurane" on rapid concentration increase |
Mechanism of volatile agent SNS depression:
- Inhibit ganglionic transmission (nicotinic α3β4 receptors)
- Depress RVLM vasomotor centre
- Blunt baroreceptor and chemoreceptor reflexes
- Reduce NE release from sympathetic terminals
- Direct myocardial depression (decrease calcium availability)
Halothane sensitization to catecholamines (HIGH YIELD):
- Mechanism: Halothane + catecholamines → re-entrant cardiac arrhythmias
- Maximum safe dose of epinephrine with halothane: 2 µg/kg (vs 10 µg/kg with isoflurane/sevoflurane)
E. OPIOIDS AND ANS
| Effect | Detail |
|---|
| Central vagomimetic | Opioids stimulate vagal nucleus → bradycardia (especially morphine, fentanyl, remifentanil) |
| ↓SNS activity | Reduce NE release from sympathetic terminals at supraspinal level |
| Histamine release | Morphine (not fentanyl/remifentanil) → histamine release → peripheral vasodilation |
| Blunt stress response | High-dose opioids (cardiac anaesthesia: 50-100 µg/kg fentanyl) significantly attenuate sympathoadrenal response to surgical stimulation |
| Respiratory depression | Blunts peripheral chemoreceptor response to hypoxia |
| Remifentanil | Most potent vagomimetic → severe bradycardia; use with glycopyrrolate |
F. NEURAXIAL ANAESTHESIA (SPINAL/EPIDURAL)
Neuraxial block produces a "chemical sympathectomy" proportional to the level and density of block.
Cardiovascular effects - depend on level:
| Block Level | SNS Blocked | Cardiovascular Effect |
|---|
| Below T10 | Only lumbar/sacral sympathetics | Minimal cardiovascular change |
| T4-T6 | Most splanchnic sympathetics | ↓SVR, ↓preload, ↓BP (major) |
| Above T4 (cardiac accelerator fibres) | T1-T4 cardiac sympathetics blocked | Bradycardia + ↓contractility + ↓BP |
| High spinal (above T1) | All SNS + phrenic nerve | Cardiovascular collapse possible; Bezold-Jarisch reflex precipitated |
Mechanism of hypotension in spinal anaesthesia:
- Sympathetic efferent block → arterial vasodilation (↓SVR)
- Venous dilation → venous pooling → ↓preload → ↓cardiac output
- If T1-T4 blocked: cardiac accelerators blocked → bradycardia
Bezold-Jarisch Reflex in Spinal Anaesthesia:
- Occurs with hypovolaemia + upright position
- Vigorous "empty" ventricle contracts against low volume → stimulates ventricular mechanoreceptors
- Results in: paradoxical bradycardia + hypotension (reflex vagal activation + sympathetic withdrawal)
- Management: Atropine + fluid/vasopressor + Trendelenburg
G. SPECIFIC DRUGS AFFECTING ANS - ANAESTHESIA PHARMACOLOGY
| Drug Class | Drug | ANS Effect | Anaesthesia Use |
|---|
| α2-Agonists | Dexmedetomidine | ↓NE release (presynaptic α2) → sedation, analgesia, ↓MAC (70-90%), ↓sympathetic tone, bradycardia, ↓BP initially | ICU sedation, adjunct to GA, awake fibreoptic intubation |
| α2-Agonists | Clonidine | Same mechanism, longer acting | Premedication, neuraxial adjuvant |
| β-Blockers | Esmolol | β1 blockade → ↓HR, ↓BP | Blunt laryngoscopy response; SVT |
| Anticholinesterases | Neostigmine | ↑ACh → muscarinic effects: bradycardia, bronchospasm, ↑secretions, gut motility | Reversal of NMB; always with anticholinergic |
| Anticholinergics | Atropine | Blocks muscarinic M2 (heart) → ↑HR, ↓secretions | Bradycardia, premedication |
| Anticholinergics | Glycopyrrolate | Quaternary amine - does NOT cross BBB; longer acting; potent antisecretory | Preferred with neostigmine reversal |
| Vasopressors | Phenylephrine | α1 agonist → vasoconstriction, reflex bradycardia | Spinal hypotension (preserves uteroplacental flow) |
| Vasopressors | Ephedrine | Indirect α+β → ↑HR + ↑BP | Spinal hypotension (preferred in obstetrics - older teaching) |
| Sympatholytics | Labetalol | α1+β blocker | Hypertension control perioperatively |
H. REGIONAL AND LOCAL ANAESTHETIC EFFECTS ON ANS
- Epidural adrenaline (epinephrine) with LA: systemic absorption → β2 effects (tachycardia, ↓K+), local vasoconstriction prolongs block, absorption test marker
- Interscalene block: proximity to sympathetic chain → ipsilateral Horner's syndrome (miosis, ptosis, anhidrosis, enophthalmos) in up to 100% - due to stellate ganglion block
- Stellate ganglion block: deliberate therapeutic use for CRPS, hot flushes, arrhythmias
SECTION 8 - AUTONOMIC SYNDROMES RELEVANT TO ANAESTHESIA
| Syndrome | Mechanism | Anaesthetic Implication |
|---|
| Horner's Syndrome | Interruption of oculosympathetic pathway (T1 → superior cervical ganglion → eye) | Expected after interscalene block; concerning if new post-intubation |
| Autonomic Dysreflexia | Spinal cord injury above T6: uncontrolled SNS below lesion with exaggerated responses | Triggered by surgical/bladder stimulation; severe hypertension + bradycardia; requires deep anaesthesia |
| Orthostatic Hypotension | Failure of sympathetic vasoconstriction on standing | Treat with position, fluids, phenylephrine; common post-spinal |
| Diabetic Autonomic Neuropathy | Loss of sympathetic regulation + vagal tone | "Silent MI", gastroparesis (aspiration risk), labile BP, resting tachycardia, orthostatic hypotension |
| MAO Inhibitors | ↑Synaptic catecholamines (block MAO) | Avoid indirect sympathomimetics (ephedrine, tyramine foods → "hypertensive crisis"); avoid pethidine (serotonin syndrome); use direct-acting vasopressors only |
| Tricyclic Antidepressants | Block NE reuptake + anticholinergic | Exaggerated response to indirect vasopressors; anticholinergic effects |
| Carcinoid Syndrome | Tumour secretes serotonin, bradykinin, histamine, tachykinins | Perioperative carcinoid crisis (flushing, bronchospasm, hypotension); treat with Octreotide |
| Phaeochromocytoma | Catecholamine-secreting tumour | Pre-operative α-blockade (phenoxybenzamine 10-14 days) → then β-blockade; intraoperative hypertensive crisis on tumour handling |
SECTION 9 - SUMMARY TABLE: ANS EFFECTS OF COMMON ANAESTHETIC AGENTS
| Agent | HR | BP | SVR | Cardiac Output | Baroreflex | Special ANS Note |
|---|
| Propofol | ↓ | ↓↓ | ↓↓ | ↓ | Blunted | Vagomimetic; hypotension via SNS depression |
| Thiopentone | ↑ (reflex) | ↓ | ↓ | ↓ | Blunted | Reflex tachycardia common |
| Etomidate | NC | NC | NC | NC | Maintained | Cardiovascular stability; choice in shock |
| Ketamine | ↑↑ | ↑↑ | ↑ | ↑ | Maintained | Indirect sympathomimetic; catecholamine release |
| Halothane | ↓↓ | ↓↓ | ↓ | ↓↓ | Blunted | Sensitizes myocardium to catecholamines |
| Isoflurane | ↑ (reflex) | ↓↓ | ↓↓ | NC/↑ | Blunted | Reflex tachycardia from vasodilation |
| Sevoflurane | NC | ↓ | ↓ | NC/↓ | Moderate blunting | Safest for cardiac; minimal HR change |
| Desflurane | ↑↑ (rapid ↑) | ↑ (rapid ↑) | ↑ (rapid ↑) | NC | Blunted | Sympathetic surge with rapid concentration ↑ |
| Morphine | ↓ | ↓ | ↓ | ↓ | Blunted | Histamine release; vagomimetic |
| Fentanyl | ↓↓ | NC | NC | NC | Blunted | Potent vagomimetic; no histamine |
| Remifentanil | ↓↓↓ | ↓ | ↓ | ↓ | Blunted | Most potent bradycardia of all opioids |
| Dexmedetomidine | ↓↓ | ↓ | ↑ (initial) then ↓ | ↓ | Maintained | Biphasic BP; profound α2 agonism; ↓MAC 70-90% |
| Spinal (T4-T6) | ↓ (if above T4) | ↓↓ | ↓↓ | ↓ | Bypassed | Chemical sympathectomy |
QUICK EXAM MNEMONICS
Cranial nerve parasympathetic outflow: "3, 7, 9, 10" (OIII, OVII, OIX, OX)
Sympathetic thoracolumbar levels: T1-L3 (or T1-L2/L3)
All preganglionic fibers release: ACh (both SNS and PNS preganglionic = nicotinic)
Adrenal medulla exception: Preganglionic SNS fiber → ACh (nicotinic on chromaffin cells) → EPI + NE release
Sweat glands exception: Sympathetic innervation but ACh (muscarinic) is the neurotransmitter
Ketamine vs all others: Only anaesthetic that ↑HR + ↑BP (indirect sympathomimetic)
Desflurane: Only volatile that causes acute SNS surge with rapid concentration increase
Halothane sensitisation: Avoid epinephrine-containing LA solutions during halothane; maximum 2 µg/kg adrenaline
Sources: Barash, Cullen & Stoelting's Clinical Anesthesia 9e (Chapter 14 - Anesthesia and the Autonomic Nervous System) | Braunwald's Heart Disease 12e | Guyton & Hall Medical Physiology | Katzung's Basic & Clinical Pharmacology 16e | ANS Sympathetic Review - Anesthesiology 2008