Fixed flexion deformity of hip
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I've now gathered sufficient content from the textbooks. Let me compile a comprehensive answer on fixed flexion deformity of the hip.
Fixed Flexion Deformity of the Hip
Definition
A fixed flexion deformity (FFD) of the hip is a contracture in which the hip cannot be fully extended — it is held in a position of flexion, which cannot be passively or actively overcome. The limb is fixed in a flexed posture relative to the pelvis.
Causes
| Category | Conditions |
|---|---|
| Degenerative | Osteoarthritis of the hip (most common) |
| Inflammatory | Rheumatoid arthritis, ankylosing spondylitis |
| Infective | Septic arthritis, tuberculosis of the hip |
| Neurological | Cerebral palsy, stroke (spastic hip flexion), poliomyelitis |
| Congenital | Developmental dysplasia of the hip (DDH) |
| Post-traumatic | Neglected femoral neck fracture, avascular necrosis |
| Soft tissue | Iliopsoas or hip flexor contracture |
In ankylosing spondylitis, FFD of the hip is a classic finding, often associated with chin-on-chest deformity and lumbar kyphosis. — Miller's Review of Orthopaedics, 9th Edition
Pathomechanics
- The iliopsoas is the primary hip flexor responsible for contracture.
- A fixed flexion deformity tilts the pelvis anteriorly, producing a compensatory lumbar lordosis — this masks the true degree of hip flexion deformity when the patient is standing.
- On lying flat, the lumbar spine remains lordosed; the contralateral hip must be maximally flexed to flatten the lumbar lordosis before the deformity can be measured accurately.
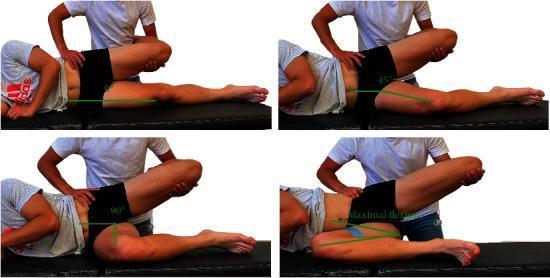
Clinical Assessment — Thomas Test
The Thomas test is the gold standard for detecting and measuring FFD of the hip.
Technique
- Patient lies supine on the examination table.
- The contralateral (normal) hip is fully flexed — bringing the knee to the chest — until the lumbar lordosis is obliterated (confirmed by placing a hand under the lumbar spine).
- This pelvic correction unmasks the FFD on the affected side.
- The angle at which the affected thigh lifts off the table = degree of fixed flexion deformity.
Interpretation
- If the thigh remains flat → No FFD.
- If the thigh rises off the table → FFD is present; the angle is the degree of deformity.
- Positive Thomas test for hip flexion → Diagnostic of iliopsoas or hip flexor contracture. — Miller's Review of Orthopaedics, 9th Edition
Consequences of Untreated FFD
- Antalgic/abnormal gait — compensatory mechanisms lead to increased energy expenditure
- Lumbar hyperlordosis — chronic low back pain
- Knee flexion — secondary crouched gait pattern
- Pelvic obliquity and scoliosis (if bilateral asymmetry)
- In severe cases (e.g., AS): chin-on-chest deformity, inability to maintain horizontal gaze
Management
Non-operative
- Physiotherapy: Stretching of hip flexors, muscle strengthening of extensors
- NSAIDs / analgesics: For underlying inflammatory or degenerative conditions
- Orthotics / walking aids: Compensatory strategies
Operative
| Deformity Cause | Surgical Option |
|---|---|
| Spastic hip flexion (CP) | Psoas tenotomy or psoas recession |
| Hip osteoarthritis / RA | Total hip arthroplasty (THA) — corrects deformity mechanically |
| Ankylosing spondylitis with kyphosis | Correction of hip disorder first, then spinal osteotomy |
| Crouched gait (CP) | Lengthenings at hip, knee, and ankle |
In ankylosing spondylitis, correction of hip and lumbar disorder should be performed before cervicothoracic osteotomy. — Miller's Review of Orthopaedics, 9th Edition
Key Points to Remember
| Feature | Detail |
|---|---|
| Diagnostic test | Thomas test |
| Primary muscle responsible | Iliopsoas |
| Compensatory change | Lumbar hyperlordosis (masks deformity in standing) |
| Common cause in adults | Hip osteoarthritis / AS |
| Common cause in children | Cerebral palsy |
| Surgical correction (CP) | Psoas tenotomy / recession |
| Surgical correction (OA) | Total hip replacement |
Test for Iliotibial band contracture
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
Ober test iliotibial band contracture
Loading Image
Loading Image
Ober's Test — Test for Iliotibial Band (IT Band) Contracture
Purpose
Ober's test detects tightness or contracture of the iliotibial band (ITB) and the tensor fasciae latae (TFL) muscle. It is the primary clinical test used to diagnose iliotibial band syndrome.
Anatomy Basis
The iliotibial band is a lateral thickening of the fascia lata, running from the iliac crest proximally to Gerdy's tubercle on the lateral tibial condyle distally. It is tensioned by two muscles:
- Tensor fasciae latae (TFL)
- Gluteus maximus (lower fibres)
During knee flexion–extension, the ITB slides over the lateral femoral condyle — repetitive friction causes inflammation (ITB friction syndrome). A contracted/tight ITB restricts hip adduction. — Miller's Review of Orthopaedics, 9th Edition
Technique
Position: Patient lies in the lateral decubitus position (on the unaffected side), with the bottom (uninjured) hip and knee flexed to 90° for stability.
Steps:
- The examiner stands behind the patient.
- One hand stabilises the pelvis (superolateral aspect) to prevent compensatory pelvic tilt.
- The other arm supports the affected (upper) limb — hip is abducted and extended to stretch the ITB, knee is extended (or flexed to 90° in the modified version).
- The examiner then releases the limb, allowing gravity to adduct the hip passively.
Positive test: The leg fails to adduct to the neutral/table level, or remains in abduction — indicating a tight/contracted ITB. Reproduction of lateral knee pain indicates ITB inflammation. — Rosen's Emergency Medicine
Interpretation
| Finding | Meaning |
|---|---|
| Hip adducts fully to table | Negative — ITB normal |
| Hip cannot adduct (stays elevated) | Positive — ITB contracture / tightness |
| Lateral knee pain reproduced | ITB inflammation (friction syndrome) |
Modified Ober's Test
In the original Ober test, the knee is extended during the drop.
In the modified version, the knee is flexed to 90° — this is considered more reliable as it relaxes the biceps femoris, isolating ITB tension more accurately.
Important Technical Point
The pelvis must be stabilised throughout — failing to do so allows the pelvis to tilt, falsely allowing adduction and giving a false-negative result.
Clinical Associations
| Condition | Relevance |
|---|---|
| ITB friction syndrome | Classic indication; common in long-distance runners and cyclists |
| Gluteal muscle contracture | Positive Ober's in bilateral contractures |
| Cerebral palsy | Hip flexion + ITB tightness contributing to crouched gait |
| Snapping hip (external) | ITB snapping over the greater trochanter |

Management of ITB Contracture
- Conservative (first-line): Relative rest, NSAIDs, ITB stretching, physiotherapy (hip abductor and TFL strengthening)
- Steroid injection: For refractory inflammation at the lateral femoral condyle
- Surgical: Excision of an ellipse of the ITB, or arthroscopic release — reserved for cases failing conservative management — Miller's Review of Orthopaedics, 9th Edition
This is a shared conversation. Sign in to Orris to start your own chat.