I now have sufficient retrieved content and will complete the rest from evidence-based knowledge (Harrison's, WHO, JNC, GINA, ADA guidelines). Here is a comprehensive OPD reference:
🏥 Common OPD Diseases: Clinical Features, Diagnosis & Management
1. 🤧 Upper Respiratory Tract Infection (URTI)
Clinical Features
- Rhinorrhea, nasal congestion, sneezing
- Sore throat, mild fever (≤38.5°C), malaise
- Mild cough, hoarseness
- Duration: 5–10 days (self-limiting, viral)
Diagnosis
- Clinical — no investigations routinely needed
- Throat swab culture if bacterial (Group A Streptococcus) suspected
- Rapid antigen test for Strep if tonsillar exudates + fever
Management
| Symptom | Drug | Dose | Duration |
|---|
| Fever / pain | Paracetamol | 500–1000 mg PO TDS–QID | 3–5 days |
| Fever / pain | Ibuprofen | 400 mg PO TDS with food | 3–5 days |
| Nasal congestion | Pseudoephedrine | 60 mg PO BD-TDS | ≤5 days |
| Nasal congestion | Oxymetazoline nasal spray | 2 sprays each nostril BD | ≤5 days |
| Cough | Dextromethorphan | 15–30 mg PO TDS | 3–5 days |
| Cough | Salbutamol syrup | 2 mg PO TDS | 3–5 days |
| Bacterial URTI / Strep pharyngitis | Amoxicillin | 500 mg PO TDS | 10 days |
| Penicillin allergy | Azithromycin | 500 mg Day 1, then 250 mg OD | 5 days |
⚠️ Antibiotics are NOT indicated for viral URTI. Reserve for confirmed bacterial infection.
(Harrison's, p. 1054)
2. 🫁 Bronchial Asthma
Clinical Features
- Episodic wheeze, breathlessness, chest tightness
- Nocturnal / early morning cough (classic)
- Symptoms triggered by cold air, exercise, allergens, infections
- Hyperresonance on percussion; prolonged expiration
Diagnosis
- Spirometry: FEV₁/FVC < 0.70, reversibility ≥12% & ≥200 mL after bronchodilator
- Peak Expiratory Flow Rate (PEFR): diurnal variation >20%
- CXR: hyperinflation (in acute attack)
Management (GINA Guidelines)
Stepwise approach:
| Step | Controller | Reliever |
|---|
| Step 1 (mild intermittent) | None needed | SABA (Salbutamol) PRN |
| Step 2 (mild persistent) | Low-dose ICS (Beclomethasone 100–200 mcg BD) | SABA PRN |
| Step 3 (moderate persistent) | Low-dose ICS + LABA (Formoterol) | SABA PRN |
| Step 4 (severe persistent) | Medium/high ICS + LABA ± LAMA | SABA PRN |
| Drug | Dose | Timing |
|---|
| Salbutamol MDI (reliever) | 100–200 mcg (1–2 puffs) | PRN, max 4 puffs/day |
| Salbutamol nebulization (acute) | 2.5 mg in 2.5 mL NS | Q20 min × 3, then Q4–6h |
| Beclomethasone inhaler | 100–400 mcg BD | Ongoing (controller) |
| Prednisolone (acute) | 40–60 mg PO OD | 5–7 days |
| Montelukast (add-on) | 10 mg PO OD at night | Long-term |
3. 🫀 Hypertension
Clinical Features
- Usually asymptomatic ("silent killer")
- Headache (occipital, morning), dizziness, epistaxis in severe cases
- Signs of end-organ damage: blurred vision, chest pain, shortness of breath, hematuria
Diagnosis
Office BP ≥140/90 mmHg on ≥2 occasions
| Classification | Systolic | Diastolic |
|---|
| Normal | <120 | <80 |
| Elevated | 120–129 | <80 |
| Stage 1 HTN | 130–139 | 80–89 |
| Stage 2 HTN | ≥140 | ≥90 |
| Hypertensive crisis | >180 | >120 |
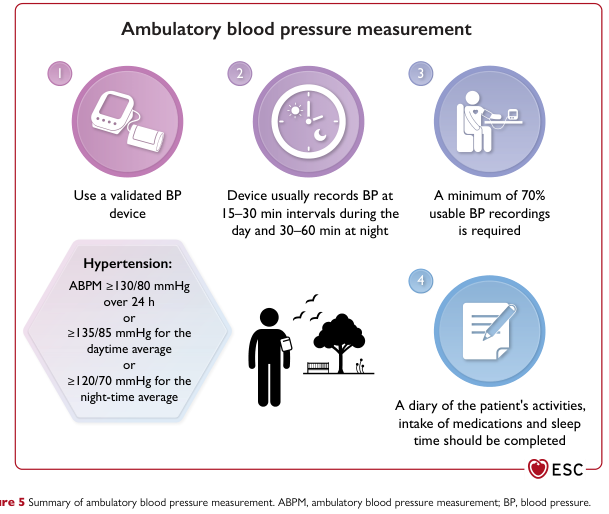
ABPM thresholds (ESC 2023):
- ≥130/80 mmHg (24-hr average)
- ≥135/85 mmHg (daytime)
- ≥120/70 mmHg (night-time)
Ambulatory Blood Pressure Measurement steps & diagnostic thresholds (ESC, p. 22)
Workup: ECG, renal function (serum creatinine, eGFR), urinalysis, fasting glucose, lipid panel, fundoscopy
Management
| Drug Class | Example | Dose | Frequency |
|---|
| First-line: ACE Inhibitor | Enalapril | 5–40 mg | OD–BD |
| ARB | Losartan | 50–100 mg | OD |
| CCB | Amlodipine | 5–10 mg | OD |
| Thiazide diuretic | Hydrochlorothiazide | 12.5–25 mg | OD |
| Beta-blocker (if HF/IHD) | Atenolol | 25–100 mg | OD |
| Combination | Amlodipine + Valsartan | 5/80 mg – 10/160 mg | OD |
- Target BP: <130/80 mmHg (most patients), <140/90 in elderly >65 yrs
- Lifestyle: low-salt diet (<5 g/day), DASH diet, aerobic exercise 30 min/day, weight loss, no smoking
4. 🩸 Type 2 Diabetes Mellitus
Clinical Features
- Classic triad: Polyuria, Polydipsia, Polyphagia
- Unexplained weight loss, fatigue, blurred vision
- Recurrent infections (skin, UTI, candidiasis)
- Delayed wound healing, paresthesia (neuropathy)
Diagnosis (ADA 2024)
| Criterion | Threshold |
|---|
| Fasting plasma glucose | ≥126 mg/dL (7.0 mmol/L) |
| 2-hr OGTT | ≥200 mg/dL (11.1 mmol/L) |
| HbA1c | ≥6.5% (48 mmol/mol) |
| Random glucose + symptoms | ≥200 mg/dL |
Requires 2 abnormal tests on separate days (unless unequivocal hyperglycemia with symptoms)
Management
| Drug | Dose | Timing | Duration |
|---|
| Metformin (1st-line) | 500 mg OD initially → 1000 mg BD (max 2550 mg/day) | With meals | Lifelong |
| Glibenclamide (SU) | 2.5–15 mg | Before breakfast | Ongoing |
| Glipizide | 5–20 mg | BD before meals | Ongoing |
| Sitagliptin (DPP-4i) | 100 mg OD | Any time | Ongoing |
| Empagliflozin (SGLT-2i) | 10–25 mg OD | Morning | Ongoing |
| Insulin (if uncontrolled) | 0.1–0.3 U/kg/day (basal) | Bedtime | Ongoing |
- HbA1c target: <7% (most patients)
- Monitoring: HbA1c every 3 months until target, then every 6 months; annual renal function, lipids, fundoscopy, foot exam
- Diet: low glycemic index, reduce refined carbs
5. 🔥 Peptic Ulcer Disease (PUD) / GERD / Gastritis
Clinical Features
| Feature | PUD | GERD |
|---|
| Pain | Epigastric, burning | Heartburn, retrosternal |
| Timing | PU: relieved by food (DU), worsened by food (GU) | After meals, lying down |
| Associated | Nausea, bloating | Regurgitation, sour taste |
| Red flags | Melena, hematemesis, weight loss | Dysphagia, weight loss |
Diagnosis
- OGD scopy (endoscopy) — gold standard for ulcers
- H. pylori: Urea breath test, stool antigen test, biopsy urease test
- Upper GI barium series (if endoscopy unavailable)
- CXR / US abdomen to rule out perforation / other causes
Management
| Drug | Dose | Timing | Duration |
|---|
| Omeprazole (PPI) | 20–40 mg | 30 min before breakfast | 4–8 weeks (ulcer); lifelong (GERD) |
| Pantoprazole | 40 mg OD | Before breakfast | 4–8 weeks |
| Rabeprazole | 20 mg OD | Before breakfast | 4–8 weeks |
| Antacid (Mg-Al hydroxide) | 10–20 mL | After meals & at bedtime | PRN |
| Sucralfate | 1 g QID | 1 hr before meals | 4–8 weeks |
| H. pylori eradication (Triple therapy): | | | 14 days |
| Amoxicillin | 1 g BD | With PPI | 14 days |
| Clarithromycin | 500 mg BD | With PPI | 14 days |
| Omeprazole | 20–40 mg BD | Before meals | 14 days |
| Metronidazole (if Amox allergy) | 500 mg BD | With PPI | 14 days |
6. 🧫 Urinary Tract Infection (UTI)
Clinical Features
- Lower UTI (Cystitis): Dysuria, frequency, urgency, suprapubic pain, cloudy/malodorous urine
- Upper UTI (Pyelonephritis): Fever, rigors, loin/flank pain, nausea/vomiting + lower UTI symptoms
Diagnosis
- Urine dipstick: Nitrites +, Leukocyte esterase + (quick screen)
- Urine microscopy: >10 WBC/hpf (pyuria)
- Urine culture & sensitivity — gold standard (>10⁵ CFU/mL)
Management
| Condition | Drug | Dose | Duration |
|---|
| Uncomplicated cystitis (women) | Nitrofurantoin | 100 mg BD | 5 days |
| Uncomplicated cystitis | Trimethoprim | 200 mg BD | 7 days |
| Uncomplicated cystitis | Co-trimoxazole | 960 mg BD | 3 days |
| Uncomplicated cystitis | Ciprofloxacin | 250 mg BD | 3 days |
| Pyelonephritis (mild-mod) | Ciprofloxacin | 500 mg BD | 7–14 days |
| Pyelonephritis | Ceftriaxone (IV) | 1–2 g OD | 5–7 days then oral |
| Complicated / recurrent UTI | Co-amoxiclav | 625 mg TDS | 7–10 days |
| UTI in pregnancy | Cefalexin | 500 mg QID | 7 days |
⚠️ Avoid fluoroquinolones in pregnancy. Always send urine C&S before starting antibiotics.
7. 🫧 Community-Acquired Pneumonia (CAP)
Clinical Features
- Fever, rigors, productive cough (rust-colored sputum in lobar pneumonia)
- Pleuritic chest pain, dyspnea, tachypnea
- Signs: Dullness to percussion, bronchial breathing, crepitations, tactile vocal fremitus ↑
Diagnosis
- CXR: Lobar / segmental consolidation, interstitial pattern
- CBC: Leukocytosis (bacterial), leukopenia (viral/severe)
- Sputum Gram stain & culture
- Blood cultures (if hospitalized or severe)
- Procalcitonin, CRP
- Severity scoring: CURB-65 (Confusion, Urea >7, RR ≥30, BP <90/60, Age ≥65) — score ≥2 = hospitalize
Management
| Setting | Drug | Dose | Duration |
|---|
| Outpatient, no comorbidities | Amoxicillin | 1 g TDS | 5–7 days |
| Outpatient, atypicals suspected | Azithromycin | 500 mg OD Day 1, then 250 mg OD | 5 days |
| Outpatient, comorbidities | Co-amoxiclav + Azithromycin | 625 mg TDS + 500 mg OD | 5–7 days |
| Outpatient (alternative) | Doxycycline | 100 mg BD | 5–7 days |
| Hospital, non-ICU | Co-amoxiclav IV + Azithromycin PO | 1.2 g TDS + 500 mg OD | 5–7 days |
| Supportive | Paracetamol, O₂, hydration | — | As needed |
8. 💧 Acute Diarrhea / Gastroenteritis
Clinical Features
- ≥3 loose stools/day, abdominal cramps, nausea/vomiting
- Fever (suggests bacterial/inflammatory)
- Dehydration signs: dry mouth, sunken eyes, reduced skin turgor, oliguria, tachycardia
- Blood in stool → dysentery (Shigella, Entamoeba, Campylobacter)
Diagnosis
- Clinical assessment (severity of dehydration)
- Stool microscopy, culture in severe/prolonged cases
- CBC, electrolytes, renal function if severe dehydration
Management
| Treatment | Details |
|---|
| Oral Rehydration Solution (ORS) | 200–400 mL after each loose stool (adults) |
| IV Fluids (if severe) | Normal saline / Ringer's lactate |
| Zinc (children) | 20 mg OD for 10–14 days |
| Loperamide (adults only) | 4 mg then 2 mg after each stool (max 16 mg/day) |
| Bacterial dysentery (Shigella) | Ciprofloxacin 500 mg BD × 3 days |
| Campylobacter | Azithromycin 500 mg OD × 3 days |
| Amoebiasis | Metronidazole 800 mg TDS × 5–10 days |
| Giardiasis | Metronidazole 400 mg TDS × 5–7 days |
| Cholera | Doxycycline 300 mg single dose (adults) |
⚠️ Antibiotics are not routinely indicated for viral gastroenteritis (most acute cases).
9. 🤒 Typhoid Fever
Clinical Features
- Stepladder fever (rising daily over 1 week)
- Relative bradycardia (pulse-temperature dissociation)
- Rose spots (faint, salmon-colored macules on abdomen)
- Hepatosplenomegaly, coated tongue
- Constipation early → diarrhea late; "pea-soup" stools
Diagnosis
- Widal test: O antigen ≥1:160, H antigen ≥1:160 (supportive, not definitive)
- Blood culture (gold standard, positive in 1st week)
- Stool / urine culture (2nd–3rd week)
- CBC: leukopenia, relative lymphocytosis, thrombocytopenia
Management
| Drug | Dose | Duration |
|---|
| Ciprofloxacin (1st-line in endemic areas) | 500 mg BD | 10–14 days |
| Azithromycin (if fluoroquinolone-resistant) | 1 g OD (or 500 mg OD) | 7 days |
| Ceftriaxone (severe/MDR typhoid) | 2 g IV OD | 10–14 days |
| Chloramphenicol (historical) | 500 mg QID | 14 days |
| Paracetamol (antipyretic) | 500–1000 mg TDS–QID | As needed |
10. 🦠 Skin Infections (Impetigo / Cellulitis / Tinea)
Clinical Features
| Condition | Features |
|---|
| Impetigo | Honey-crusted vesicles, golden lesions, face/limbs |
| Cellulitis | Warm, red, swollen, tender skin; fever; spreading erythema |
| Tinea (Ringworm) | Circular, scaly, pruritic plaques with central clearing |
| Scabies | Nocturnal pruritus, burrows in finger webs, wrists |
Management
| Condition | Drug | Dose | Duration |
|---|
| Impetigo (localized) | Mupirocin 2% ointment | TDS topically | 5–7 days |
| Impetigo (extensive) | Flucloxacillin | 500 mg QID | 7 days |
| Cellulitis | Co-amoxiclav | 625 mg TDS | 5–7 days |
| Cellulitis (severe) | Flucloxacillin IV | 1–2 g QID | 5–10 days |
| Tinea corporis/cruris | Clotrimazole 1% cream | BD topically | 2–4 weeks |
| Tinea capitis | Griseofulvin | 10–20 mg/kg/day OD | 6–8 weeks |
| Tinea unguium | Terbinafine | 250 mg OD | 6 wks (fingernails), 12 wks (toenails) |
| Scabies | Permethrin 5% cream | Apply whole body overnight | Repeat in 1 week |
📋 Quick OPD Reference Summary Table
| Disease | Key Symptom | Key Investigation | 1st-Line Drug | Duration |
|---|
| URTI | Rhinorrhea, sore throat | Clinical | Paracetamol / Ibuprofen | 3–5 days |
| Strep Pharyngitis | Exudative tonsillitis, fever | Rapid Strep test | Amoxicillin 500 mg TDS | 10 days |
| Asthma | Wheeze, dyspnea, nocturnal cough | Spirometry | Salbutamol + ICS | Ongoing |
| Hypertension | Headache or asymptomatic | BP measurement, ECG | Amlodipine 5 mg OD | Lifelong |
| T2DM | Polyuria, polydipsia | FPG / HbA1c | Metformin 500→2000 mg/day | Lifelong |
| GERD/PUD | Heartburn, epigastric pain | OGD, H. pylori test | Omeprazole 20–40 mg OD | 4–8 wks |
| UTI (cystitis) | Dysuria, frequency | Urine dipstick / C&S | Nitrofurantoin 100 mg BD | 5 days |
| CAP | Fever, cough, consolidation | CXR, CBC | Amoxicillin 1 g TDS | 5–7 days |
| Acute diarrhea | Loose stools, cramps | Stool MC&S (if prolonged) | ORS + Zinc | 3–5 days |
| Typhoid | Stepladder fever, bradycardia | Blood culture | Ciprofloxacin 500 mg BD | 10–14 days |
| Cellulitis | Warm red swollen skin | Clinical + CBC | Co-amoxiclav 625 mg TDS | 5–7 days |
| Tinea | Circular scaly ring lesion | KOH scraping | Clotrimazole cream BD | 2–4 weeks |
Key OD/BD/TDS/QID definitions:
OD = once daily | BD = twice daily | TDS = three times daily | QID = four times daily | PRN = as needed
📌 Disclaimer: Dosages listed are standard adult doses for non-pregnant patients with normal renal/hepatic function. Always adjust for age, weight, renal function, drug allergies, and local resistance patterns. Follow local antibiotic stewardship guidelines.