MYOCARDIAL INFARCTION FOR USMLE STEP 1 EXAM
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have everything I need for a comprehensive USMLE Step 1 guide. Let me compile the full response.
Myocardial Infarction - USMLE Step 1 High-Yield Review
Sources: Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease, Ganong's Review of Medical Physiology, Fuster and Hurst's The Heart, Goldman-Cecil Medicine
Overview - STEMI at a Glance
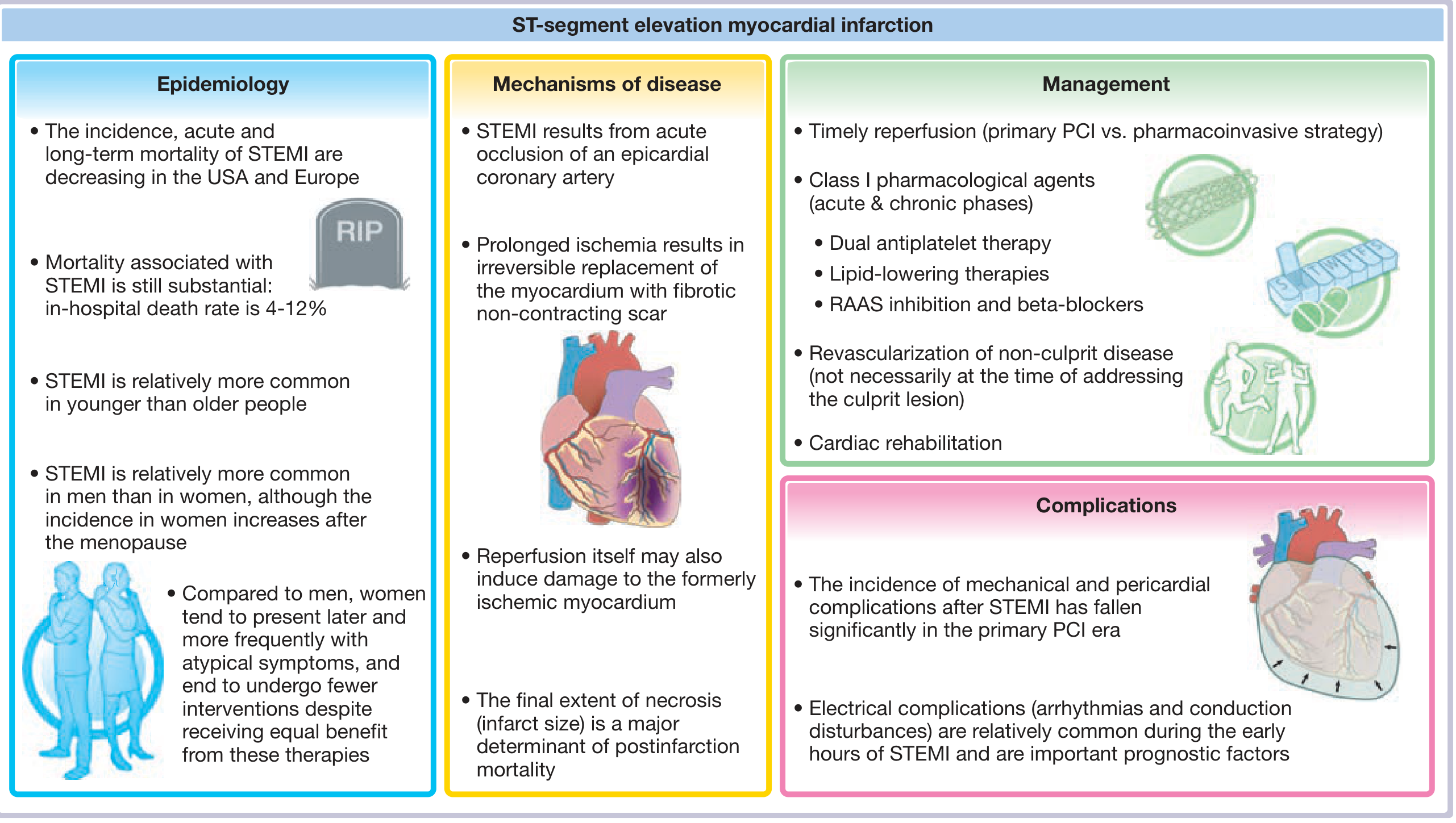
1. Definition & Epidemiology
Myocardial infarction (MI) is necrosis of heart muscle resulting from ischemia. The 2018 joint U.S./European task force defines MI as "acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
- ~10% of MIs occur before age 40; 45% occur before age 65
- Men > Women until menopause; post-menopause the gap narrows
- Women present more frequently with atypical symptoms and tend to receive fewer interventions
- In-hospital STEMI mortality: 4-12%
2. Pathogenesis - The Step-by-Step Sequence
The vast majority of MIs are caused by acute thrombosis on a disrupted atherosclerotic plaque:
- Plaque disruption - erosion or rupture exposes subendothelial collagen and necrotic plaque contents
- Platelet adhesion and activation - release of TXA2, ADP, and serotonin → more aggregation + vasospasm
- Coagulation activation - tissue factor exposure amplifies the thrombus
- Complete luminal occlusion within minutes
90% of MIs show coronary thrombosis on angiography within 4 hours. By 12-24 hours, only ~60% still show it (spontaneous lysis occurs).
10% of MIs occur WITHOUT occlusive atherosclerosis - causes include:
- Coronary vasospasm (e.g., cocaine use, Prinzmetal angina)
- Embolism from mural thrombus (atrial fibrillation) or valve vegetations
- Small-vessel disease (vasculitis, amyloid, sickle cell disease)
- Robbins & Kumar Basic Pathology, p. 354
3. Progression of Myocardial Necrosis
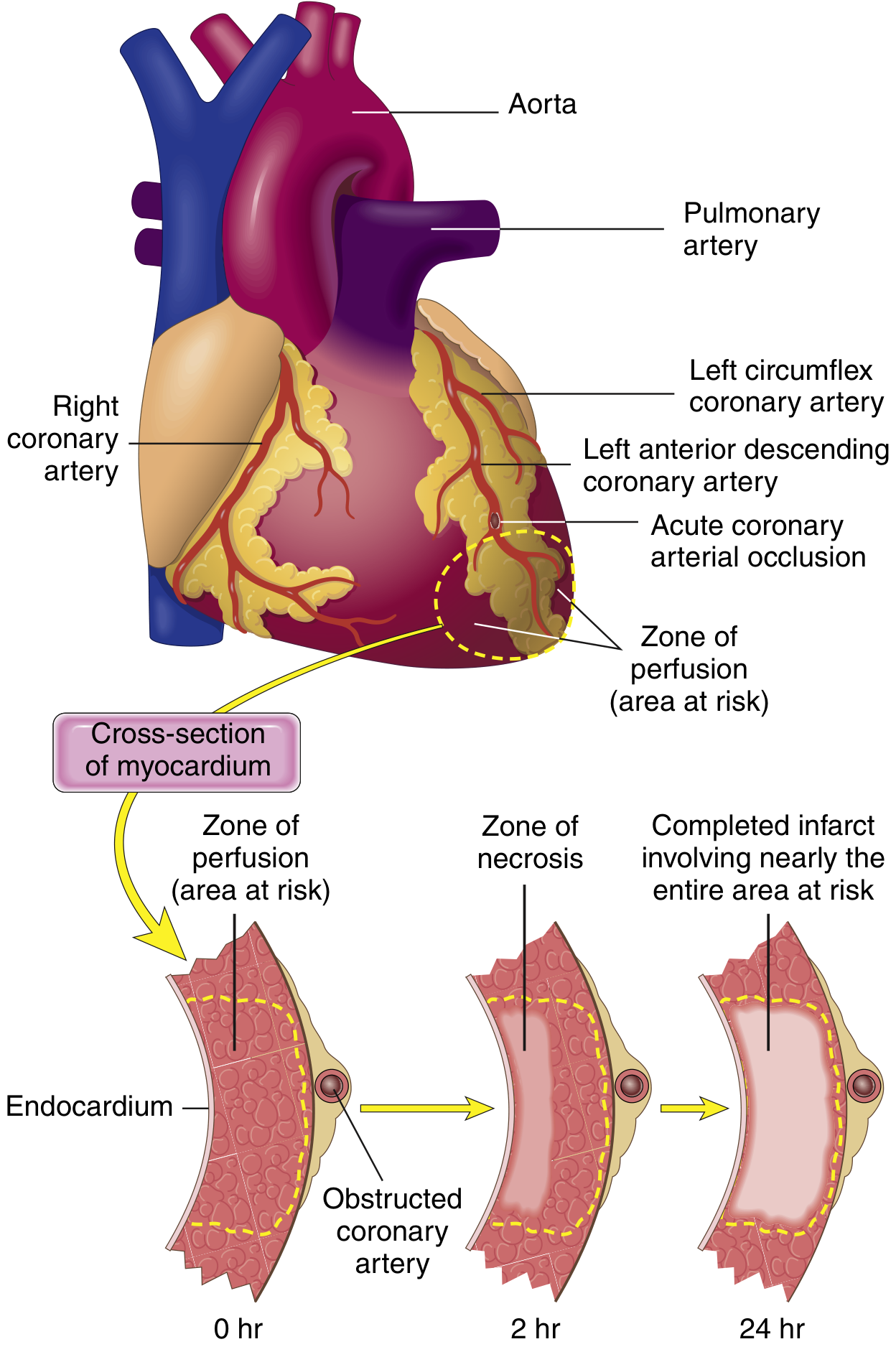
Key concept: Irreversible injury begins in the subendocardium (last to be perfused, highest intramural pressure). With prolonged ischemia, a "wavefront" of necrosis moves toward the epicardium.
- Reversible ischemia if reperfused within ~20-40 minutes
- Transmural infarct develops over 3-6 hours if no intervention
- A thin rim of subendocardium is spared even in transmural MI (oxygenated by diffusion from ventricular cavity)
4. Coronary Artery Territories (HIGH YIELD)
| Artery | Territory | % of MIs |
|---|---|---|
| LAD (Left Anterior Descending) | Anterior LV wall, anterior 2/3 of septum, apex | 40-50% |
| RCA (Right Coronary Artery) | Right ventricle, posterior LV, SA node, AV node | 30-40% |
| LCX (Left Circumflex) | Lateral LV wall | 15-20% |
Dominance: The posterior descending artery (PDA) arises from:
- RCA in 90% of people = right dominant (most common)
- LCX in left dominant
Step 1 pearl: RCA occlusion → inferior MI + SA/AV node involvement → bradycardia, heart block. Also → right ventricular infarction (treat with IV fluids, NOT diuretics or nitrates).
5. Morphologic Timeline (MASTER TABLE - Most Tested on Step 1)
| Time | Gross | Light Microscopy | Key Feature |
|---|---|---|---|
| 0-30 min | None | None | Reversible; mitochondrial swelling only (EM) |
| 30 min - 4 hr | None | Wavy fibers at border | Sarcolemmal disruption |
| 4-12 hr | Dark mottling | Onset coagulative necrosis, edema | Earliest gross change |
| 12-24 hr | Dark mottling | Coagulative necrosis, pyknosis, hypereosinophilic myocytes, neutrophil infiltrate begins, contraction band necrosis | First neutrophils |
| 1-3 days | Mottling with yellow-tan center | Brisk neutrophil infiltrate | Peak neutrophils |
| 3-7 days | Soft, yellow-tan center | Dying neutrophils, early macrophage infiltration, granulation tissue | Highest risk of free wall rupture |
| 7-10 days | Yellow-tan, soft center; red-tan margins | Macrophages phagocytosing dead cells, more granulation tissue, early fibrosis | Still high rupture risk |
| 2-8 wk | Gray-white scar | Collagen deposition | Scar firming |
| >2 months | White glistening scar | Dense collagen scar | Complete healing |
- Robbins & Kumar Basic Pathology, Table 9.2
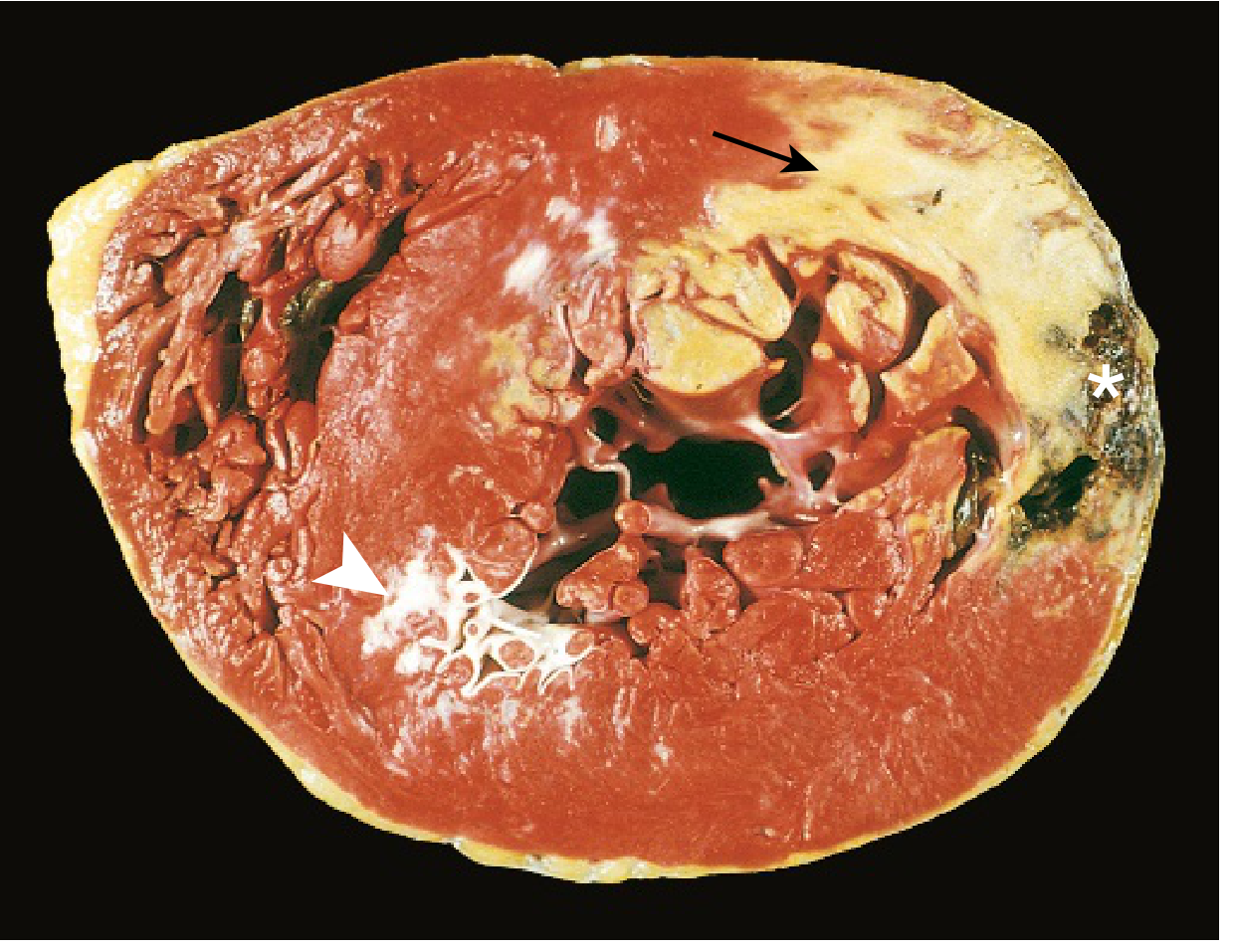
Gross specimen: Acute posterolateral MI (pale area = no TTC staining due to enzyme leakage). Anterior white scar = old healed MI. Hemorrhage at edge = free wall rupture.
6. Cardiac Biomarkers
| Marker | Rises | Peaks | Normalizes | Notes |
|---|---|---|---|---|
| Troponin I/T | 3-6 hr | 24-48 hr | 7-14 days | Most sensitive and specific; gold standard |
| CK-MB | 4-8 hr | 24 hr | 48-72 hr | Useful for detecting reinfarction (re-rises) |
| Myoglobin | 1-4 hr | 6-7 hr | 24 hr | Earliest; NOT cardiac-specific |
| LDH (LDH1 > LDH2) | 24-48 hr | 3-6 days | 8-14 days | Historical; "flipped pattern" |
Step 1 pearl: If a patient presents late (>24-48 hr) and troponin is already coming down, CK-MB is better for identifying reinfarction.
7. ECG Changes (Ganong's Physiology)
Three mechanisms drive ECG changes in acute MI:
| Defect in Infarcted Cells | Current Flow | ECG Change (leads over infarct) |
|---|---|---|
| Rapid repolarization (K+ leak) | Out of infarct | ST elevation |
| Decreased resting membrane potential | Into infarct | TQ depression → recorded as ST elevation |
| Delayed depolarization | Out of infarct | ST elevation |
Temporal ECG evolution:
- Hyperacute T waves (very early - minutes)
- ST elevation (acute phase - hours to days)
- Q wave formation (dead tissue electrically silent; within hours to days; persistent)
- T-wave inversion (days to weeks)
- Persistent Q waves = marker of old transmural MI
Reciprocal ST depression appears in leads opposite the infarct.
Localization by ECG leads:
| Leads with ST elevation | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCX |
| II, III, aVF | Inferior | RCA (or LCX in left dominant) |
| V1 (tall R wave), V7-V9 | Posterior | RCA or LCX |
| V3R, V4R | Right ventricle | RCA |
- Ganong's Review of Medical Physiology, p. 534
8. Consequences and Complications of MI
Timing of Complications (USMLE LOVES THIS)
| Time Post-MI | Complication | Mechanism |
|---|---|---|
| Within 24 hr | Arrhythmias (VF, VT) | Electrical instability; #1 cause of early death |
| 1-3 days | Fibrinous pericarditis | Transmural inflammation reaching the pericardium |
| 3-5 days | Free wall rupture | Neutrophil-mediated softening of myocardium |
| 3-5 days | Ventricular septal defect (VSD) | Septal rupture; new harsh holosystolic murmur |
| 3-5 days | Papillary muscle rupture → acute mitral regurgitation | Posterior papillary muscle (single blood supply from RCA) most vulnerable; new soft systolic murmur |
| Days to weeks | Mural thrombus | Akinetic wall + endocardial inflammation; risk of stroke |
| Weeks to months | Ventricular aneurysm | Thinning and outward bulging of infarcted wall (usually anterior/apical, from LAD occlusion); persistent ST elevation on ECG |
| 1-8 weeks | Dressler syndrome | Autoimmune pericarditis; fever, pleuritic chest pain, elevated ESR; treat with NSAIDs |
Key distinctions:
- Free wall rupture → pericardial tamponade → pulseless electrical activity (PEA)
- VSD vs papillary rupture: both cause new murmurs post-MI, but VSD is a systolic thrill, papillary rupture causes acute pulmonary edema
- True aneurysm vs pseudoaneurysm: true = thinned fibrotic wall; pseudo = contained free wall rupture (higher risk of re-rupture)
- Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease
9. Reperfusion Injury
When blood is restored to ischemic myocardium, reperfusion itself can cause damage:
- Reperfusion arrhythmias (most common - usually benign)
- Stunned myocardium - viable but temporarily non-contractile; recovers over days
- Hibernating myocardium - chronically reduced contractility due to chronic ischemia; can recover with revascularization
- Contraction band necrosis - hypercontracted sarcomeres due to Ca²+ overload; hallmark on histology of reperfused myocardium
10. Management Overview (STEMI)
Acute:
- Primary PCI is preferred if available within 90 min (door-to-balloon)
- Fibrinolysis (tPA, streptokinase) if PCI not available within 120 min
- Antiplatelet therapy: Aspirin + P2Y12 inhibitor (clopidogrel, ticagrelor)
- Anticoagulation (heparin)
- Beta-blockers, ACE inhibitors/ARBs (reduce remodeling)
- High-intensity statins
Contraindications to thrombolytics: Prior hemorrhagic stroke, recent surgery/trauma, active bleeding, severe hypertension
11. High-Yield USMLE Step 1 Mnemonics
"STEMI vs NSTEMI"
- STEMI = complete occlusion, transmural → ST elevation + Q waves
- NSTEMI = partial occlusion, subendocardial → ST depression or T-wave inversions, NO Q waves; troponin elevated
"Most common cause of death"
- Within 1 hour: VF (ventricular fibrillation)
- In hospital: Cardiogenic shock (pump failure)
- Late death: CHF / arrhythmias
"Which papillary muscle ruptures?"
- Posterior papillary muscle = single blood supply (PDA from RCA)
- Anterior papillary muscle = dual supply (LAD + LCX) → less vulnerable
Rupture timing: "3-5-7"
- Free wall rupture: most common 3-5 days
- VSD: 3-5 days
- Full healing: ~6-8 weeks
"Zones of ischemia" (from center outward):
- Zone of necrosis → center; irreversible
- Zone of injury → ST elevation
- Zone of ischemia → T-wave inversion; reversible
12. Quick Summary Table
| Feature | Detail |
|---|---|
| Most common cause | Atherosclerotic plaque rupture + thrombosis |
| Most common artery | LAD (40-50%) |
| First biomarker to rise | Myoglobin (1-4 hr) |
| Gold-standard biomarker | Troponin I or T |
| Earliest histologic change | Wavy fibers (30 min - 4 hr) |
| First cells seen | Neutrophils (12-24 hr) |
| Peak neutrophils | 1-3 days |
| Peak macrophages | 3-7 days |
| Earliest complication | Arrhythmias/VF (within 24 hr) |
| Highest rupture risk | 3-7 days (softened by neutrophils) |
| Scar complete | >2 months |
| Dressler syndrome | 1-8 weeks post-MI; autoimmune pericarditis |
ASK ME ONE NBME STYLE QUESTION
A 67-year-old man is brought to the emergency department 30 minutes after the sudden onset of severe substernal chest pain radiating to his left arm. He is diaphoretic and pale. ECG shows ST elevation in leads II, III, and aVF. He is taken for emergent cardiac catheterization and reperfusion is achieved. Three days later, the patient develops sudden hypotension, a new holosystolic murmur heard best at the left lower sternal border, and an oxygen step-up is noted on right heart catheterization.
Which of the following best explains this patient's current condition?
- (A) Rupture of the posterior papillary muscle causing acute mitral regurgitation
- (B) Rupture of the interventricular septum causing left-to-right shunt
- (C) Free wall rupture causing pericardial tamponade
- (D) Development of a left ventricular aneurysm
- (E) Dressler syndrome causing fibrinous pericarditis
Take your time. When you're ready, reply with your answer and your reasoning.
E
❌ Incorrect — The answer is (B)
Why B is correct: Ventricular Septal Rupture
Let's break down the three key clues in the stem:
| Clue | Interpretation |
|---|---|
| Inferior MI (ST elevation in II, III, aVF) → RCA territory | Affects the posterior septum |
| Holosystolic murmur at the left lower sternal border | Blood shunting through a septal defect |
| Oxygen step-up on right heart catheterization | O₂-rich blood from LV entering the RV through the VSD → pathognomonic |
The oxygen step-up is the definitive clue. It means blood oxygenation is higher in the RV than the RA, which only happens when oxygenated left-sided blood crosses into the right side - i.e., a left-to-right shunt through a VSD.
Why you chose E - and why it's wrong
Dressler syndrome does cause chest pain and fever post-MI, but:
- It presents 1-8 weeks after MI, not day 3
- It causes pericarditic chest pain (pleuritic, positional), NOT hypotension or a new murmur
- It does NOT produce an oxygen step-up
- It has NO holosystolic murmur
Why the other choices fail
| Choice | Why Wrong |
|---|---|
| (A) Posterior papillary rupture | Also gives a holosystolic murmur and hypotension, but the murmur is heard best at the apex (mitral regurgitation), and right heart cath would show tall V waves in the wedge tracing, NOT an O₂ step-up |
| (C) Free wall rupture | Causes PEA / tamponade - no murmur, Beck's triad (hypotension, muffled heart sounds, JVD) |
| (D) LV aneurysm | Develops over weeks to months; causes persistent ST elevation but no acute decompensation with a new murmur |
The High-Yield Distinction to Lock In
New holosystolic murmur + O₂ step-up = VSD New holosystolic murmur + tall V waves on wedge = Papillary muscle rupture (MR)
Both occur at 3-5 days post-MI when neutrophil infiltration is at its peak, softening the myocardium. Both present with hypotension and pulmonary edema. The right heart cath is what separates them on the exam.
Ready for another question?
This is a shared conversation. Sign in to Orris to start your own chat.