Teache me as neonatatologist, paeditrcian in depth topic- Spina bifida
"spina bifida" OR "myelomeningocele" AND management
"myelomeningocele" AND "fetal surgery" AND outcomes
Spina Bifida - Complete Teaching Module for the Neonatologist & Pediatrician
1. DEFINITION & OVERVIEW
- Incidence ranges 0.04% to 0.15% in some series; now approximately 1 in 3,000 in folic acid-supplemented populations
- More frequent in girls than boys
- ~80% of spina bifida cases are "open" - covered only by a thin membrane of exposed neural tissue
- 25-40% of MMC pregnancies are now terminated following prenatal diagnosis
The Developing Human: Clinically Oriented Embryology; Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anesthesia 10e
2. EMBRYOLOGY & PATHOGENESIS
Timeline
- Neural tube closure occurs during weeks 3-4 of gestation (days 17-28)
- The caudal neuropore closes around day 28 - hence the lumbar/sacral predominance of lesions
- Spina bifida occulta results from failure of neural arch ossification
- Spina bifida cystica (MMC/meningocele) results from failure of actual neural tube closure
Two-Hit Hypothesis for Myelomeningocele
- First hit: Primary failure of neural tube closure at 3-4 weeks gestation - anatomical malformation
- Second hit: Progressive secondary damage from continued exposure of open neural elements to amniotic fluid - neurotoxic environment and direct trauma
Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anesthesia 10e
3. CLASSIFICATION
| Type | Description | Neural Tissue in Sac? | Neurological Deficit |
|---|---|---|---|
| Spina Bifida Occulta | Bony defect only, skin intact | No | Usually none |
| Meningocele | Meninges + CSF herniate, skin-covered | No (usually) | Minimal to none |
| Myelomeningocele (MMC) | Meninges + spinal cord + nerve roots exposed | YES | Significant - level-dependent |
| Myeloschisis / Rachischisis | Complete failure of closure, no covering membrane | YES (open placode) | Severe |
Spina Bifida Occulta
- Occurs in L5/S1 in ~10% of otherwise normal people
- Usually asymptomatic
- Cutaneous stigmata may be present (see image below)
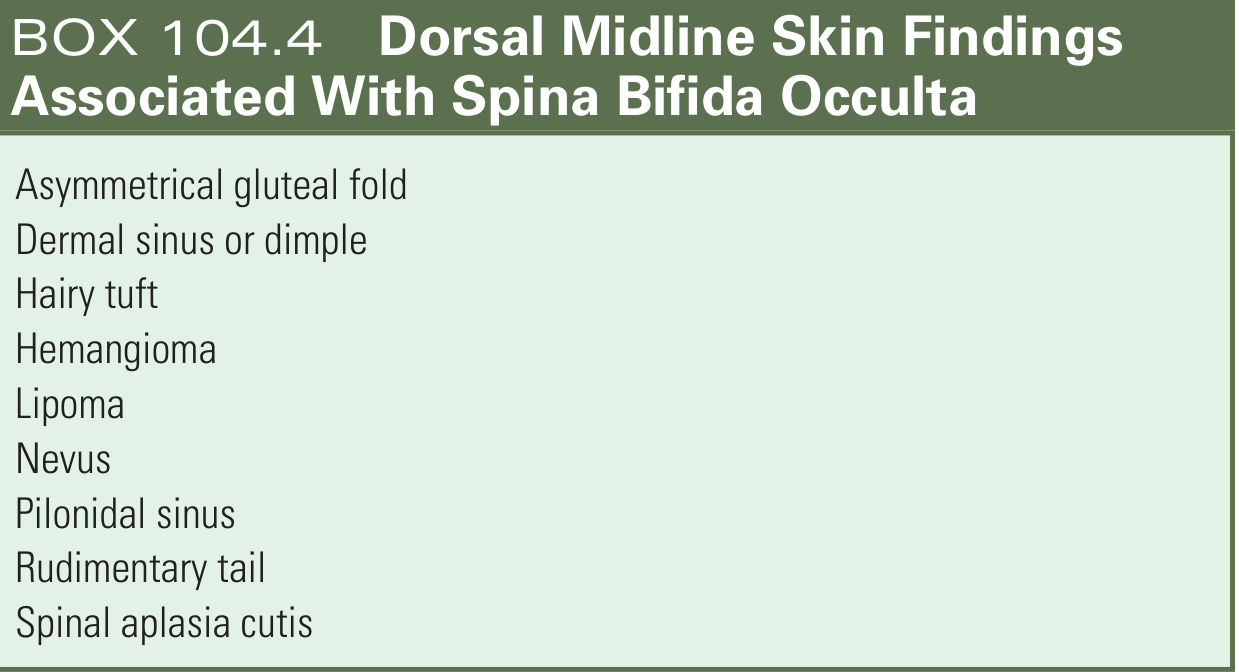
- Hairy tuft (hypertrichosis)
- Dermal sinus or dimple (NOT the sacral dimple, which is normal)
- Hemangioma, lipoma, nevus
- Asymmetrical gluteal fold
- Rudimentary tail
- Spinal aplasia cutis
Spina Bifida Cystica
- Occurs in ~1 in 5,000 births (severe cystic forms)
- Lumbosacral region is most common (>80%)
- Followed by sacral, thoracic, then cervical
Bradley and Daroff's Neurology in Clinical Practice; The Developing Human: Clinically Oriented Embryology
4. PRENATAL DIAGNOSIS
Maternal Serum AFP (MSAFP)
- Tested at 14-16 weeks gestation
- Elevated in ~85% of open NTDs
- False-positive rate ~5%
- Amniotic fluid AFP is more reliable; used for confirmation after elevated serum levels
Ultrasound (Gold Standard in Practice)
- Detects >90% of NTDs at 18-20 weeks
- Combined AFP + ultrasound sensitivity >95%
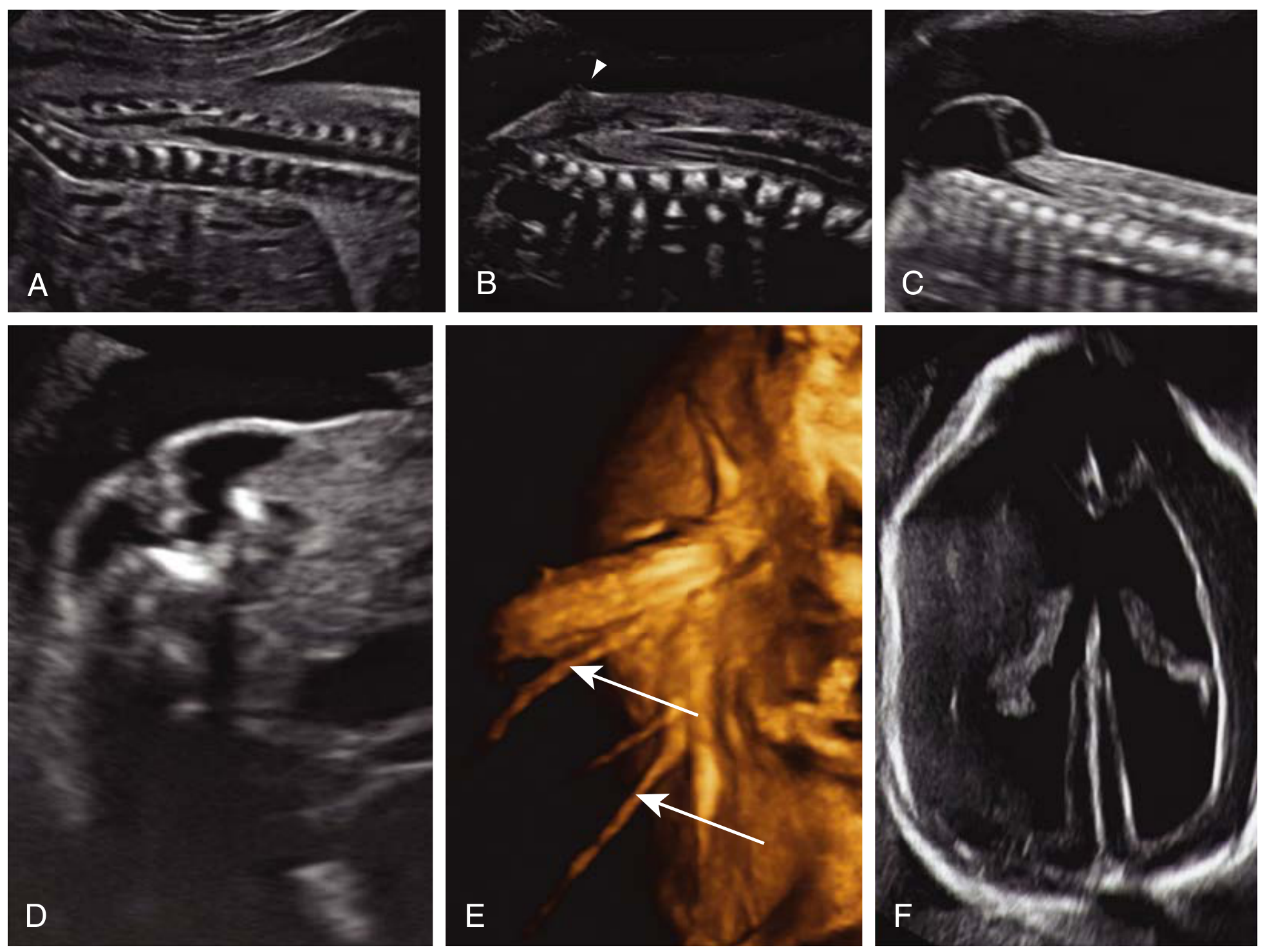
| Sign | Description | Significance |
|---|---|---|
| Lemon sign | Concave (scalloped) shape of frontal calvaria | Present in ~98% of open NTDs before 24 weeks; fades later |
| Banana sign | Anterior curvature/obliteration of cerebellum | Present in ~95% of cases; Chiari II downward displacement |
| Ventriculomegaly | Dilated lateral ventricles | Secondary hydrocephalus |
| Splayed posterior ossification centers | U-shaped vertebrae on transverse view | Pathognomonic of open vertebral defect |
| Cystic dorsal mass | Protruding sac from lumbosacral spine | Direct visualization of defect |
Creasy & Resnik's Maternal-Fetal Medicine; Barash Clinical Anesthesia 9e
5. ASSOCIATED ANOMALIES (Critical for the Neonatologist)
A. Chiari II Malformation (Arnold-Chiari Type II)
- Caudal displacement of cerebellar vermis through the foramen magnum
- Caudal displacement of medulla oblongata + cervical cord
- Kinking of the medulla ("cervicomedullary kink")
- Obliteration of cisterna magna
- Small posterior fossa
- Polymicrogyria, corpus callosum anomalies
- Stridor (vocal cord paralysis)
- Central apnea and bradycardia
- Aspiration pneumonia
- Sleep-disordered breathing
- Lack of coordination, spasticity
- Only ~20% have symptomatic brainstem dysfunction, but mortality in symptomatic patients is very high (35% with brainstem dysfunction die by 5 years)
B. Hydrocephalus
- Develops in 80-90% of infants with MMC
- Caused by Chiari II blocking CSF flow through the 4th ventricle
- Of those with lumbosacral MMC: 64-85% require VP shunting
- ~50% of shunted children have shunt complications in the first year
- Mean IQ in shunted MMC patients ≈ 80 (low normal); lower than non-shunted patients
- Mortality by age 5 years: 14% overall; 35% in those with brainstem dysfunction
C. Tethered Cord Syndrome
- Spinal cord stretched as the spinal column elongates during growth
- Conus medullaris found at abnormally low level
- Progressive neurological deterioration: worsening leg weakness, bowel/bladder dysfunction, scoliosis, back pain
- Requires surgical untethering
- Can occur post-repair of MMC as a late complication
D. Latex Allergy (CRITICALLY Important)
- Children with spina bifida have 28-67% positive skin test rates to latex proteins
- Markedly increased incidence of latex anaphylaxis
- Risk from early, repeated mucosal exposure to latex (urinary catheters, surgical gloves)
- ALL spina bifida patients must be managed in a latex-free environment from birth onward
- This is a patient safety non-negotiable
Barash Clinical Anesthesia 9e; Bradley and Daroff's Neurology; Morgan & Mikhail Clinical Anesthesiology; Cummings Otolaryngology
6. NEUROLOGICAL DEFICITS BY LESION LEVEL
| Lesion Level | Motor Function | Ambulation Prognosis |
|---|---|---|
| Thoracic | Complete paraplegia, hip flexion absent | Wheelchair dependent |
| High Lumbar (L1-L2) | Hip flexors present, no knee extension | Wheelchair, may use braces |
| Mid Lumbar (L3-L4) | Quadriceps present (knee extension) | Community ambulation with AFO |
| Low Lumbar (L5) | Ankle dorsiflexion present | Good community ambulation |
| Sacral | Plantar flexion, intrinsic foot muscles weak | Near-normal gait |
- Bladder sphincter paralysis is universal with lumbosacral lesions
- Bowel sphincter paralysis is common
- "Saddle block" pattern of sensory loss when sphincters involved
7. NEONATAL ASSESSMENT AT BIRTH
Initial Evaluation Checklist
- Level of defect - count vertebral segments, correlate with function
- Sac integrity - intact skin/membrane? Ruptured/leaking CSF? Open placode?
- Neurological examination - spontaneous movement, response to stimulation below level
- Head circumference - already above 98th percentile? Signs of raised ICP?
- Fontanelle - bulging = raised ICP
- Cranial nerve function - suck, swallow, cry, eye movements
- Bladder assessment - palpable bladder, stream, post-void residual
- Orthopedic survey - foot/hip deformities, spine inspection
- Associated anomalies - cardiac, renal screen
Positioning and Wound Care
- Place infant prone to protect the sac
- Cover the open placode/sac with warm, sterile saline-soaked gauze to prevent desiccation
- Apply sterile non-adherent dressing - do NOT let sac dry out
- Avoid diapers and direct pressure on defect
- Use latex-free materials exclusively from the first moment of contact
Infection Prevention
- Start broad-spectrum antibiotics (typically ampicillin + gentamicin) immediately upon admission
- CSF leakage from ruptured sac is a portal for meningitis
- Keep infant prone, minimize contamination
Barash Clinical Anesthesia 9e; Bailey & Love 28e
8. SURGICAL MANAGEMENT
A. Timing of Postnatal Repair
- Surgery within 24-48 hours of birth is the standard of care
- Reduces risk of ventriculitis, ascending infection, and progressive neurological deterioration
- Does not restore already-lost function but prevents further loss
- Microsurgical dissection to detach neural placode from surrounding skin
- Dural closure
- Fascial, subcutaneous, and skin closure in layers
- Most centers close the defect + place VP shunt simultaneously if hydrocephalus is present
- Some centers delay shunting until symptomatic hydrocephalus develops post-closure
B. Fetal Surgery (Prenatal MMC Repair) - The MOMS Trial
- Open fetal surgery at 19-25 weeks gestation (open maternal laparotomy + hysterotomy)
- Primary composite outcome (fetal/neonatal death OR need for CSF shunt): significantly reduced in prenatal repair group
- Significantly less need for VP shunting
- Better motor function at 2 years (more likely to walk independently)
- Reduction in Chiari II severity
- Singleton pregnancy
- MMC between T1 and S1 level
- Chiari II malformation
- 19-25 weeks gestation
- Normal karyotype
- Maternal criteria met (no contraindications to surgery)
- Preterm delivery (mean gestational age ~34 weeks in fetal surgery group vs ~37 weeks in postnatal group)
- Uterine dehiscence / scar complications
- PPROM
- Maternal morbidity
Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e
9. UROLOGICAL MANAGEMENT (Critical in Pediatrics)
Neuropathic Bladder in MMC
- Universal with lumbosacral lesions
- Detrusor-sphincter dyssynergia - dangerous combination leading to high bladder pressures
- If untreated: vesicoureteral reflux → recurrent UTIs → hydronephrosis → renal scarring → ESRD
Management Protocol
- Baseline renal ultrasound + urodynamics in the neonatal period
- Clean Intermittent Catheterization (CIC) - cornerstone of management, started early
- Anticholinergics (oxybutynin) to reduce bladder overactivity and protect upper tracts
- Regular urodynamic surveillance - every 6-12 months initially
- Watch for vesicoureteral reflux - requires prophylactic antibiotics or surgical correction
- Bowel management program runs in parallel
Bailey & Love 28e; Campbell-Walsh Urology
10. ORTHOPEDIC COMPLICATIONS
| Problem | Mechanism | Management |
|---|---|---|
| Clubfoot / Calcaneal deformity | Muscle imbalance | Ponseti casting ± surgery |
| Hip dislocation/subluxation | Muscle imbalance (L2-L3 level) | Observation or surgical reduction |
| Knee contractures (flexion or extension) | Spasticity + imbalance | Physiotherapy, splinting, surgery |
| Scoliosis/Kyphosis | Vertebral dysplasia + muscle imbalance | Bracing → spinal fusion |
| Ankle valgus | Tibial torsion + muscle imbalance | Supramalleolar osteotomy |
| Pathological fractures | Osteoporosis from immobility, insensate limbs | Prevention, padding |
| Pressure sores | Insensate skin | Pressure relief, turning, seating |
Campbell's Operative Orthopaedics 15e
11. COGNITIVE & NEURODEVELOPMENTAL OUTCOMES
- >70% of long-term survivors have IQ >80
- Only 37% can live independently as adults
- Mean IQ in VP-shunted MMC patients ≈ 80 (low normal); significantly lower with shunt complications or higher lesion levels
- Common cognitive profiles: verbal skills relatively preserved; visuospatial/executive function impaired ("cocktail party speech")
- Attention, memory, processing speed often affected
- Early developmental intervention and educational support are critical
12. MULTIDISCIPLINARY TEAM (MDT)
| Specialty | Role |
|---|---|
| Neurosurgery | Defect closure, VP shunting, tethered cord release, Chiari decompression |
| Neonatology | Immediate stabilization, infection prevention, feeding support |
| Urology/Nephrology | Bladder management, renal surveillance |
| Orthopedics | Deformity prevention and correction |
| Physiotherapy | Mobility, ambulation training, AFOs |
| Occupational therapy | ADL, upper limb function |
| Developmental pediatrics | Neurodevelopmental surveillance |
| Dietitian | Nutrition, obesity (common due to immobility) |
| Psychology | Family support, cognitive development |
| Continence nurse | CIC teaching, bowel program |
13. PREVENTION
Folic Acid Supplementation
- 0.4 mg/day for all women of childbearing age (preconceptionally and first trimester)
- 4 mg/day for women with a prior NTD pregnancy (reduces recurrence risk by ~70%)
- Folic acid fortification of food has reduced NTD prevalence significantly in many countries, but has plateaued without eliminating the condition
- Antiepileptic drugs (valproate, carbamazepine) are major risk factors - they impair folate absorption; these patients need higher supplementation
- Folate supplementation reduces MMC rate by approximately 50%
Bradley and Daroff's Neurology; Harriet Lane Handbook 23e; Goodman & Gilman's Pharmacology
14. PROGNOSIS - SURVIVAL STATISTICS
| Outcome | Data |
|---|---|
| 5-year mortality (all spina bifida) | ~7.9% (79 per 1,000) |
| 5-year mortality (with brainstem dysfunction) | ~35% |
| Need for VP shunting (lumbosacral MMC) | 64-85% |
| Shunt complications in first year | ~50% |
| IQ >80 (long-term survivors) | >70% |
| Independent living as adults | ~37% |
| Hydrocephalus rate (overall MMC) | ~81% |
Creasy & Resnik's Maternal-Fetal Medicine; Barash Clinical Anesthesia 9e
15. MRI FINDINGS TO KNOW
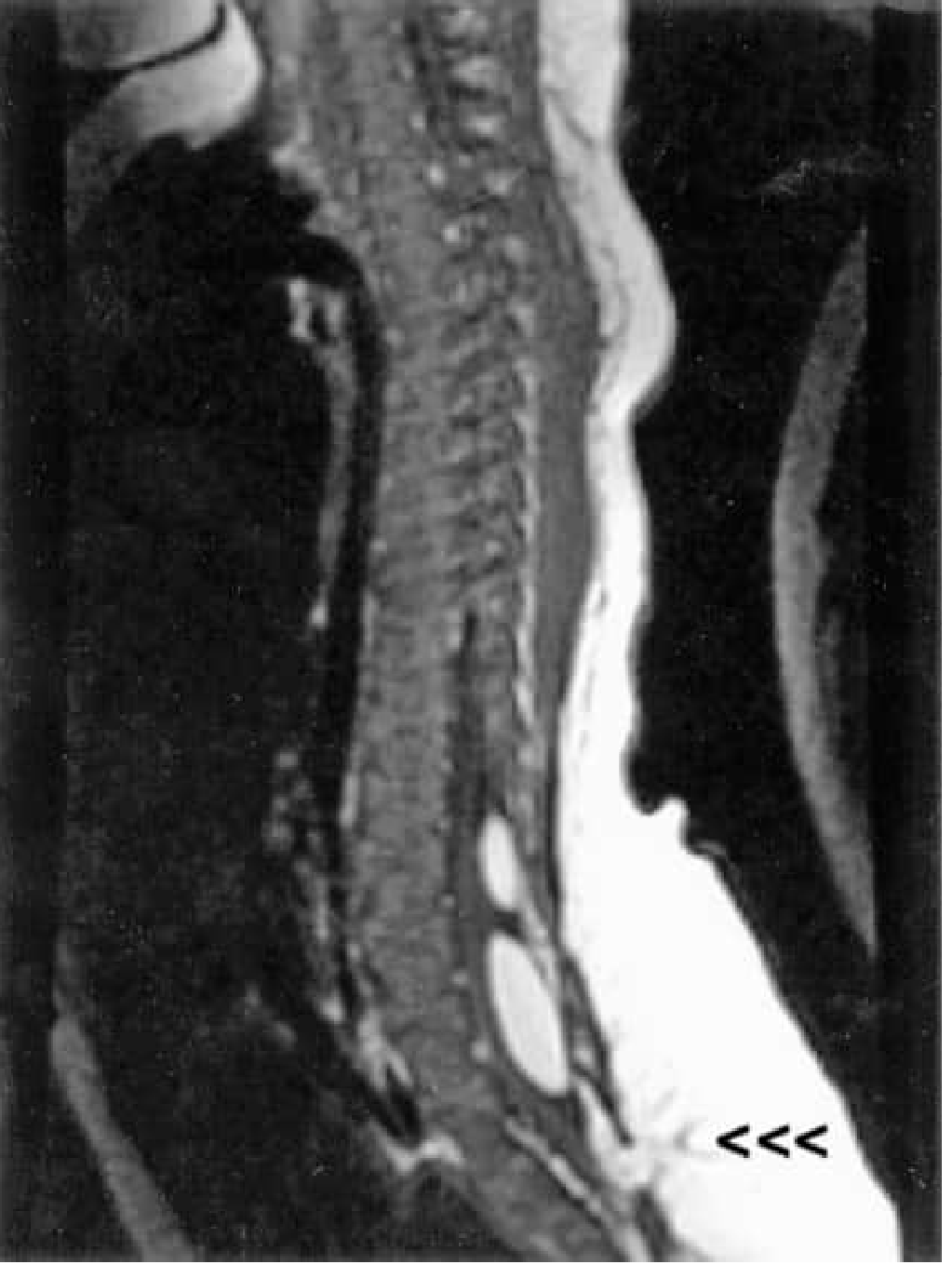
- Low-lying conus medullaris (below L2-3 after 3 months of age = tethered cord until proven otherwise)
- Neural placode - open spinal cord seen in the defect
- Chiari II - downward displacement of cerebellar vermis through foramen magnum
- Ventriculomegaly/hydrocephalus
- Syringomyelia - longitudinal fluid cavity within cord
- Lipomyelomeningocele - lipoma within the sac
- Dermoid inclusion cysts - late complication
16. CLINICAL PEARLS FOR THE NEONATOLOGIST
- Latex-free from birth - never use latex gloves, catheters, or IV equipment. Sensitization starts with first exposure.
- Airway alert - Chiari II can cause vocal cord paralysis; be prepared for intubation difficulties and upper airway obstruction
- Apnea watch - central apnea from brainstem compression can be sudden and fatal; apnea monitor for first weeks
- Prone positioning - protect the sac until surgery; do not let it dry
- CSF leak = emergency - ruptured sac with CSF leakage needs urgent neurosurgical consultation; antibiotics NOW
- Bladder triage - palpate bladder, check voiding; CIC may need to start in the first week
- Do not miss associated cardiac anomalies - screen with echocardiogram
- Feeding challenges - bulbar dysfunction from Chiari II may impair suck/swallow; NGT feeding may be needed initially
- Head circumference - measure daily; crossing centiles upward = developing hydrocephalus
- Family counseling - this is a lifelong condition requiring immense family support; begin early and honestly
17. RECENT EVIDENCE (2023-2025)
- Torres et al. 2025 (PMID 41398113) - Meta-analysis confirms prenatal MMC repair reduces VP shunt rates and improves motor outcomes vs postnatal repair (post-MOMS era evidence)
- de Oliveira Manduca Palmiero et al. 2025 (PMID 41342964) - Systematic review of neurosurgical outcomes after fetal repair; evolving techniques including endoscopic approaches showing promise
- Vencio et al. 2024 (PMID 38536450) - Systematic review of Chiari II surgical management - decompression outcomes
- Moldenhauer et al. 2025 (PMID 40886957) - MOMS trial follow-up: reproductive outcomes after open fetal surgery
Quick Summary Framework: "SPINA BIFIDA at a Glance"
ANATOMY: Failure of neural arch fusion ± neural tube closure
TIMING: Week 3-4 gestation (caudal neuropore = day 28)
TYPES: Occulta → Meningocele → MMC → Myeloschisis
DIAGNOSIS: MSAFP at 14-16 wk; US at 18-20 wk (Lemon + Banana signs)
ASSOCIATED: Chiari II (universal), Hydrocephalus (80-90%), Tethered cord
NEONATAL: Prone, sterile saline cover, antibiotics, LATEX-FREE, urgent surgery
SURGERY: Within 24-48 hours; Fetal surgery (MOMS) if selected prenatally
UROLOGY: CIC + anticholinergics; ESRD is the top cause of death
ORTHO: Clubfoot, hip dislocation, scoliosis
NEURO: IQ >80 in >70%; only 37% live independently
PREVENT: Folic acid 0.4 mg/day all women; 4 mg/day if prior NTD
Above all content in pdf
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && echo "created"
mkdir -p /tmp/workspace/spina-bifida && cat > /tmp/workspace/spina-bifida/generate_pdf.py << 'PYEOF' from reportlab.lib.pagesizes import A4 from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle from reportlab.lib.units import cm, mm from reportlab.lib import colors from reportlab.platypus import ( SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle, HRFlowable, PageBreak, KeepTogether ) from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY from reportlab.platypus import ListFlowable, ListItem import datetime OUTPUT = "/tmp/workspace/spina-bifida/Spina_Bifida_Teaching_Module.pdf" # ── Document setup ────────────────────────────────────────────────────────── doc = SimpleDocTemplate( OUTPUT, pagesize=A4, leftMargin=2*cm, rightMargin=2*cm, topMargin=2.2*cm, bottomMargin=2.2*cm, title="Spina Bifida – Teaching Module for Neonatologists & Paediatricians", author="Orris Medical Education", ) W, H = A4 # ── Colour palette ─────────────────────────────────────────────────────────── DARK_BLUE = colors.HexColor("#1A3A5C") MID_BLUE = colors.HexColor("#2E6DA4") LIGHT_BLUE = colors.HexColor("#D6E8F7") ACCENT = colors.HexColor("#E87722") # orange accent LIGHT_GREY = colors.HexColor("#F4F6F8") MID_GREY = colors.HexColor("#B0B8C1") WHITE = colors.white GREEN = colors.HexColor("#1E7A44") RED = colors.HexColor("#C0392B") AMBER = colors.HexColor("#D68910") # ── Styles ─────────────────────────────────────────────────────────────────── base = getSampleStyleSheet() def S(name, parent="Normal", **kw): s = ParagraphStyle(name, parent=base[parent], **kw) return s # Title page styles sTitle = S("sTitle", fontSize=28, textColor=WHITE, alignment=TA_CENTER, fontName="Helvetica-Bold", leading=34, spaceAfter=6) sSubtitle = S("sSubtitle", fontSize=14, textColor=colors.HexColor("#D6E8F7"), alignment=TA_CENTER, fontName="Helvetica", leading=20, spaceAfter=4) sMeta = S("sMeta", fontSize=11, textColor=colors.HexColor("#AED3EE"), alignment=TA_CENTER, fontName="Helvetica-Oblique", leading=16) # Section heading sSectionH = S("sSectionH", fontSize=14, textColor=WHITE, fontName="Helvetica-Bold", leading=18, spaceBefore=4, spaceAfter=4, leftIndent=0) # Subsection sSubH = S("sSubH", fontSize=12, textColor=DARK_BLUE, fontName="Helvetica-Bold", leading=16, spaceBefore=8, spaceAfter=4) # Body sBody = S("sBody", fontSize=9.5, textColor=colors.HexColor("#1A1A2E"), fontName="Helvetica", leading=14, spaceAfter=4, alignment=TA_JUSTIFY) # Bullet sBullet = S("sBullet", fontSize=9.5, textColor=colors.HexColor("#1A1A2E"), fontName="Helvetica", leading=13, leftIndent=14, spaceAfter=2) # Bold bullet sBulletB = S("sBulletB", fontSize=9.5, textColor=DARK_BLUE, fontName="Helvetica-Bold", leading=13, leftIndent=14, spaceAfter=2) # Pearl (clinical pearl box) sPearl = S("sPearl", fontSize=9.5, textColor=colors.HexColor("#1A3A1A"), fontName="Helvetica", leading=13, leftIndent=6, spaceAfter=2) # Warning / important sWarn = S("sWarn", fontSize=9.5, textColor=RED, fontName="Helvetica-Bold", leading=13, leftIndent=6, spaceAfter=2) # Source / footnote sSrc = S("sSrc", fontSize=7.5, textColor=MID_GREY, fontName="Helvetica-Oblique", leading=11, spaceAfter=2, alignment=TA_CENTER) # Caption sCap = S("sCap", fontSize=8.5, textColor=colors.HexColor("#444466"), fontName="Helvetica-Oblique", leading=12, spaceAfter=4, alignment=TA_CENTER) # ── Helper: section header band ────────────────────────────────────────────── def section_header(num, title, color=DARK_BLUE): data = [[Paragraph(f"<font size=11>{num}</font> {title}", sSectionH)]] t = Table(data, colWidths=[W - 4*cm]) t.setStyle(TableStyle([ ("BACKGROUND", (0,0), (-1,-1), color), ("ROUNDEDCORNERS", [6, 6, 6, 6]), ("TOPPADDING", (0,0), (-1,-1), 7), ("BOTTOMPADDING", (0,0), (-1,-1), 7), ("LEFTPADDING", (0,0), (-1,-1), 12), ("RIGHTPADDING", (0,0), (-1,-1), 12), ])) return t def subsection(title): return Paragraph(title, sSubH) def body(txt): return Paragraph(txt, sBody) def bullet(txt, bold=False): style = sBulletB if bold else sBullet return Paragraph(f"• {txt}", style) def space(h=6): return Spacer(1, h) def hr(color=MID_BLUE, thickness=0.7): return HRFlowable(width="100%", thickness=thickness, color=color, spaceAfter=4, spaceBefore=4) def source(txt): return Paragraph(txt, sSrc) def info_box(title, items, bg=LIGHT_BLUE, title_color=DARK_BLUE, border=MID_BLUE): """Coloured info box with a title row and bullet items.""" rows = [[Paragraph(f"<b>{title}</b>", ParagraphStyle( "bht", fontSize=9.5, textColor=title_color, fontName="Helvetica-Bold", leading=13, leftIndent=0))]] for it in items: rows.append([Paragraph(f"• {it}", ParagraphStyle( "bit", fontSize=9, textColor=colors.HexColor("#1A1A2E"), fontName="Helvetica", leading=13, leftIndent=6))]) t = Table(rows, colWidths=[W - 4*cm]) t.setStyle(TableStyle([ ("BACKGROUND", (0,0), (0,0), title_color), ("TEXTCOLOR", (0,0), (0,0), WHITE), ("BACKGROUND", (0,1), (-1,-1), bg), ("BOX", (0,0), (-1,-1), 1, border), ("TOPPADDING", (0,0), (-1,-1), 5), ("BOTTOMPADDING", (0,0), (-1,-1), 5), ("LEFTPADDING", (0,0), (-1,-1), 10), ("RIGHTPADDING", (0,0), (-1,-1), 10), ])) return t def warning_box(txt, bg=colors.HexColor("#FDECEA"), border=RED): data = [[Paragraph(f"⚠ {txt}", ParagraphStyle( "ww", fontSize=9.5, textColor=RED, fontName="Helvetica-Bold", leading=14))]] t = Table(data, colWidths=[W - 4*cm]) t.setStyle(TableStyle([ ("BACKGROUND", (0,0), (-1,-1), bg), ("BOX", (0,0), (-1,-1), 1.2, border), ("TOPPADDING", (0,0), (-1,-1), 7), ("BOTTOMPADDING", (0,0), (-1,-1), 7), ("LEFTPADDING", (0,0), (-1,-1), 12), ("RIGHTPADDING", (0,0), (-1,-1), 12), ])) return t def std_table(headers, rows, col_widths=None): """Standard data table with styled header.""" all_rows = [headers] + rows if col_widths is None: cw = (W - 4*cm) / len(headers) col_widths = [cw] * len(headers) data = [] for i, row in enumerate(all_rows): data.append([Paragraph(str(c), ParagraphStyle( f"tc{i}", fontSize=9, fontName="Helvetica-Bold" if i == 0 else "Helvetica", textColor=WHITE if i == 0 else colors.HexColor("#1A1A2E"), leading=12)) for c in row]) t = Table(data, colWidths=col_widths, repeatRows=1) t.setStyle(TableStyle([ ("BACKGROUND", (0,0), (-1,0), DARK_BLUE), ("BACKGROUND", (0,1), (-1,-1), colors.white), ("ROWBACKGROUNDS", (0,1), (-1,-1), [colors.white, LIGHT_GREY]), ("BOX", (0,0), (-1,-1), 0.8, MID_BLUE), ("INNERGRID", (0,0), (-1,-1), 0.4, colors.HexColor("#C8D8E8")), ("TOPPADDING", (0,0), (-1,-1), 5), ("BOTTOMPADDING", (0,0), (-1,-1), 5), ("LEFTPADDING", (0,0), (-1,-1), 8), ("RIGHTPADDING", (0,0), (-1,-1), 8), ("VALIGN", (0,0), (-1,-1), "TOP"), ])) return t # ── Header / Footer callbacks ───────────────────────────────────────────────── def on_page(canvas, doc): canvas.saveState() page_num = doc.page # Header bar canvas.setFillColor(DARK_BLUE) canvas.rect(0, H - 1.4*cm, W, 1.4*cm, fill=1, stroke=0) canvas.setFillColor(WHITE) canvas.setFont("Helvetica-Bold", 9) canvas.drawString(2*cm, H - 0.9*cm, "SPINA BIFIDA – Teaching Module for Neonatologists & Paediatricians") canvas.setFont("Helvetica", 8) canvas.drawRightString(W - 2*cm, H - 0.9*cm, "Orris Medical Education | July 2026") # Footer bar canvas.setFillColor(DARK_BLUE) canvas.rect(0, 0, W, 1*cm, fill=1, stroke=0) canvas.setFillColor(WHITE) canvas.setFont("Helvetica", 8) canvas.drawCentredString(W/2, 0.35*cm, f"Page {page_num}") # accent line canvas.setFillColor(ACCENT) canvas.rect(0, H - 1.4*cm - 3, W, 3, fill=1, stroke=0) canvas.restoreState() def on_first_page(canvas, doc): # No header/footer on title page pass # ════════════════════════════════════════════════════════════════════════════ # CONTENT BUILD # ════════════════════════════════════════════════════════════════════════════ story = [] # ── TITLE PAGE ─────────────────────────────────────────────────────────────── # Full-page blue background block title_data = [[ Paragraph("SPINA BIFIDA", sTitle), ]] title_table = Table([[ Spacer(1, 3*cm), Paragraph("SPINA BIFIDA", sTitle), Paragraph("Complete Teaching Module for", sSubtitle), Paragraph("Neonatologists & Paediatricians", sSubtitle), Spacer(1, 0.5*cm), HRFlowable(width="60%", thickness=2, color=ACCENT, spaceAfter=12, spaceBefore=12), Paragraph("Covering Embryology · Classification · Prenatal Diagnosis", sMeta), Paragraph("Neonatal Management · Surgery · Neurology · Urology · Orthopaedics", sMeta), Paragraph("Outcomes · Prevention · Recent Evidence 2023–2025", sMeta), Spacer(1, 1.5*cm), Paragraph(f"Orris Medical Education | July 2026", sMeta), ]], colWidths=[W - 4*cm]) title_table.setStyle(TableStyle([ ("BACKGROUND", (0,0), (-1,-1), DARK_BLUE), ("ALIGN", (0,0), (-1,-1), "CENTER"), ("VALIGN", (0,0), (-1,-1), "MIDDLE"), ("TOPPADDING", (0,0), (-1,-1), 10), ("BOTTOMPADDING", (0,0), (-1,-1), 10), ("LEFTPADDING", (0,0), (-1,-1), 30), ("RIGHTPADDING", (0,0), (-1,-1), 30), ])) from reportlab.platypus import Frame from reportlab.platypus.flowables import Flowable class TitlePage(Flowable): def __init__(self): Flowable.__init__(self) self.width = W - 4*cm self.height = H - 4.4*cm def draw(self): c = self.canv # big background c.setFillColor(DARK_BLUE) c.roundRect(0, 0, self.width, self.height, 12, fill=1, stroke=0) # accent stripe c.setFillColor(ACCENT) c.rect(0, self.height - 8, self.width, 8, fill=1, stroke=0) c.rect(0, 0, self.width, 8, fill=1, stroke=0) # Title c.setFillColor(WHITE) c.setFont("Helvetica-Bold", 34) c.drawCentredString(self.width/2, self.height - 90, "SPINA BIFIDA") # subtitle c.setFont("Helvetica", 15) c.setFillColor(colors.HexColor("#AED3EE")) c.drawCentredString(self.width/2, self.height - 125, "Complete Teaching Module for") c.setFont("Helvetica-Bold", 17) c.setFillColor(colors.HexColor("#D6E8F7")) c.drawCentredString(self.width/2, self.height - 150, "Neonatologists & Paediatricians") # divider c.setStrokeColor(ACCENT) c.setLineWidth(2) c.line(self.width*0.2, self.height - 175, self.width*0.8, self.height - 175) # topics c.setFont("Helvetica", 10) c.setFillColor(colors.HexColor("#7FB3D3")) topics = [ "Embryology · Classification · Prenatal Diagnosis", "Neonatal Stabilisation · Surgical Management", "Neurology · Urology · Orthopaedics · Outcomes", "Prevention · Recent Evidence 2023–2025" ] y = self.height - 210 for t in topics: c.drawCentredString(self.width/2, y, t) y -= 20 # bottom meta c.setFont("Helvetica-Oblique", 10) c.setFillColor(colors.HexColor("#AED3EE")) c.drawCentredString(self.width/2, 40, "Orris Medical Education | July 2026") c.drawCentredString(self.width/2, 22, "Sources: The Developing Human · Bradley & Daroff · Creasy & Resnik · Miller's Anaesthesia · Barash · Bailey & Love · Campbell-Walsh · Harriet Lane") story.append(TitlePage()) story.append(PageBreak()) # ═══════════════════════════════════════════════════════════════════════ # SECTION 1 – DEFINITION & OVERVIEW # ═══════════════════════════════════════════════════════════════════════ story += [ section_header("1", "DEFINITION & OVERVIEW"), space(8), body("Spina bifida is a <b>neural tube defect (NTD)</b> caused by failure of the halves of the embryonic cartilaginous neural arch to fuse, resulting in incomplete closure of the spinal column. It is the most common serious NTD affecting the CNS."), space(6), std_table( ["Parameter", "Data"], [ ["Incidence (general)", "~1 in 1,000–3,000 live births; 0.04%–0.15% in various series"], ["Sex", "More frequent in girls than boys"], ["Open defects", "~80% of cases are open (exposed neural tissue)"], ["After folic acid fortification", "~50% reduction in MMC rate; plateaued without elimination"], ["Pregnancy termination rate", "25–40% of MMC pregnancies following prenatal diagnosis"], ], col_widths=[5.5*cm, 11.5*cm] ), space(6), source("Sources: The Developing Human: Clinically Oriented Embryology; Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anaesthesia 10e"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 2 – EMBRYOLOGY & PATHOGENESIS # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("2", "EMBRYOLOGY & PATHOGENESIS"), space(8), subsection("Timeline of Neural Tube Closure"), bullet("Neural tube closure occurs during <b>weeks 3–4 of gestation</b> (days 17–28)"), bullet("The <b>caudal neuropore closes ~day 28</b> — explains lumbosacral predominance of lesions"), bullet("Spina bifida occulta = failure of neural arch ossification only"), bullet("Spina bifida cystica (MMC/meningocele) = failure of actual neural tube closure"), space(8), subsection("Two-Hit Hypothesis of Myelomeningocele (MMC)"), body("The combined mechanism explains why the defect is progressive and why fetal surgery is beneficial:"), space(4), ] two_hit = std_table( ["Hit", "Timing", "Mechanism", "Result"], [ ["1st Hit", "Weeks 3–4 gestation", "Primary failure of neural tube closure — anatomical malformation", "Open neural placode; vertebral arch defect"], ["2nd Hit", "Throughout pregnancy", "Continuous exposure of open neural elements to amniotic fluid — neurotoxic + direct trauma", "Progressive neurological injury; worsening motor/sensory deficits"], ], col_widths=[1.8*cm, 3.2*cm, 7.5*cm, 4.5*cm] ) story.append(two_hit) story.append(space(6)) story.append(info_box( "Clinical Implication of the Two-Hit Model", ["Prenatal (fetal) surgical repair aims to STOP the second hit by closing the defect and isolating the neural tissue from the amniotic environment", "Animal models (lamb) confirm: prenatal closure → near-normal postnatal neurological function", "Postnatal repair prevents further damage but does NOT restore already-lost function"], bg=colors.HexColor("#E8F5E9"), title_color=GREEN, border=GREEN )) story.append(source("Sources: Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anaesthesia 10e; Barash Clinical Anaesthesia 9e")) # ═══════════════════════════════════════════════════════════════════════ # SECTION 3 – CLASSIFICATION # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("3", "CLASSIFICATION"), space(8), std_table( ["Type", "Description", "Neural Tissue in Sac?", "Neurological Deficit"], [ ["Spina Bifida Occulta", "Bony defect only; skin intact", "No", "Usually none"], ["Meningocele", "Meninges + CSF herniate; skin-covered", "No (usually)", "Minimal to none"], ["Myelomeningocele (MMC)", "Meninges + spinal cord + nerve roots exposed", "YES", "Significant — level-dependent"], ["Myeloschisis / Rachischisis", "Complete failure of closure; no covering membrane", "YES (open placode)", "Severe"], ], col_widths=[4*cm, 5.5*cm, 3.5*cm, 4*cm] ), space(8), subsection("Spina Bifida Occulta — Cutaneous Markers (Box 104.4)"), body("Occurs in L5/S1 in <b>~10% of otherwise normal people</b>. Usually asymptomatic. Look for dorsal midline skin findings:"), space(4), ] occult_items = [ "Asymmetrical gluteal fold", "Dermal sinus or dimple (NOT normal sacral dimple)", "Hairy tuft (hypertrichosis)", "Hemangioma", "Lipoma", "Nevus", "Pilonidal sinus", "Rudimentary tail", "Spinal aplasia cutis" ] cols1 = occult_items[:5] cols2 = occult_items[5:] occult_table = Table( [[Paragraph(f"• {a}", sBullet), Paragraph(f"• {b}", sBullet)] for a, b in zip(cols1, cols2 + [""] * (len(cols1) - len(cols2)))], colWidths=[8.5*cm, 8.5*cm] ) occult_table.setStyle(TableStyle([ ("BACKGROUND", (0,0), (-1,-1), LIGHT_GREY), ("BOX", (0,0), (-1,-1), 0.8, MID_GREY), ("TOPPADDING", (0,0), (-1,-1), 3), ("BOTTOMPADDING", (0,0), (-1,-1), 3), ])) story.append(occult_table) story.append(space(6)) story.append(warning_box( "Any dorsal midline skin marker in a neonate → spinal ultrasound (age <5 months) or MRI spine is mandatory" )) story.append(source("Sources: Bradley and Daroff's Neurology in Clinical Practice; The Developing Human: Clinically Oriented Embryology")) # ═══════════════════════════════════════════════════════════════════════ # SECTION 4 – PRENATAL DIAGNOSIS # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("4", "PRENATAL DIAGNOSIS"), space(8), subsection("Maternal Serum AFP (MSAFP)"), bullet("Tested at <b>14–16 weeks</b> gestation"), bullet("Elevated in ~85% of open NTDs; false-positive rate ~5%"), bullet("<b>Amniotic fluid AFP</b> — more reliable; used for confirmation after elevated serum levels"), space(8), subsection("Ultrasound — Gold Standard"), body("Detects >90% of NTDs at 18–20 weeks. Combined AFP + ultrasound sensitivity >95%."), space(6), std_table( ["Ultrasound Sign", "Description", "Sensitivity / Notes"], [ ["Lemon sign", "Concave (scalloped) shape of frontal calvaria", "~98% of open NTDs before 24 wks; fades after 24 wks; present 1% in normals"], ["Banana sign", "Anterior curvature / obliteration of cerebellum", "~95% of cases; Chiari II downward displacement; does NOT resolve with gestation"], ["Ventriculomegaly", "Dilated lateral ventricles", "Secondary hydrocephalus; correlates with outcome"], ["Splayed vertebral ossification", "U-shaped vertebrae on transverse view", "Pathognomonic of open vertebral defect"], ["Cystic dorsal mass", "Protruding sac from lumbosacral spine", "Direct visualisation of defect"], ["Loss of intracranial translucency", "Absent IT on first-trimester scan", "Early Chiari II sign; parallel to nuchal translucency screening"], ], col_widths=[4.5*cm, 6*cm, 6.5*cm] ), space(6), source("Sources: Creasy & Resnik's Maternal-Fetal Medicine; Barash Clinical Anaesthesia 9e"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 5 – ASSOCIATED ANOMALIES # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("5", "ASSOCIATED ANOMALIES", color=MID_BLUE), space(8), subsection("A. Chiari II Malformation (Arnold-Chiari Type II)"), body("<b>Almost universal in MMC</b> — present in >95% of cases by 19–25 weeks gestation."), space(4), std_table( ["Feature", "Detail"], [ ["Anatomy", "Caudal displacement of cerebellar vermis through foramen magnum"], ["", "Caudal displacement of medulla oblongata + cervical cord"], ["", "Kinking of the medulla ('cervicomedullary kink')"], ["", "Obliteration of cisterna magna; small posterior fossa"], ["", "Polymicrogyria; corpus callosum anomalies"], ["Clinical consequences", "Stridor (vocal cord paralysis)"], ["", "Central apnea and bradycardia"], ["", "Aspiration pneumonia; sleep-disordered breathing"], ["", "Lack of co-ordination; spasticity"], ["Symptomatic rate", "Only ~20% are clinically symptomatic for brainstem dysfunction"], ["Mortality", "35% mortality in those WITH brainstem dysfunction by age 5 years"], ["Treatment", "Shunting first; if symptoms persist → posterior fossa decompression"], ], col_widths=[4*cm, 13*cm] ), space(10), subsection("B. Hydrocephalus"), std_table( ["Parameter", "Data"], [ ["Prevalence in MMC", "80–90% develop hydrocephalus"], ["Mechanism", "Chiari II blocks CSF flow through 4th ventricle → secondary hydrocephalus"], ["VP shunt rate (lumbosacral MMC)", "64–85% require ventriculoperitoneal shunting"], ["Shunt complications (year 1)", "~50% of shunted patients have complications"], ["Mean IQ (shunted)", "~80 (low normal); significantly lower vs non-shunted"], ], col_widths=[6*cm, 11*cm] ), space(10), subsection("C. Tethered Cord Syndrome"), bullet("Stretching of spinal cord as spinal column elongates during childhood growth"), bullet("Conus medullaris at abnormally low level (below L2–3 after age 3 months)"), bullet("Signs: worsening leg weakness, bowel/bladder deterioration, scoliosis, back pain"), bullet("Treatment: <b>surgical untethering</b>; may occur as late complication post-MMC repair"), space(8), subsection("D. Latex Allergy — PATIENT SAFETY CRITICAL"), ] story.append(warning_box( "28–67% of children with spina bifida have positive skin tests to latex proteins. " "ALL spina bifida patients MUST be managed in a completely latex-free environment from birth." )) story.append(space(4)) story.append(bullet("Risk from early, repeated mucosal exposure to latex catheters and surgical gloves")) story.append(bullet("Latex anaphylaxis can be fatal — sensitisation starts with first exposure")) story.append(bullet("Use only latex-free gloves, catheters, IV equipment, and surgical materials")) story.append(source("Sources: Barash Clinical Anaesthesia 9e; Bradley & Daroff's Neurology; Morgan & Mikhail; Cummings Otolaryngology")) # ═══════════════════════════════════════════════════════════════════════ # SECTION 6 – NEUROLOGICAL DEFICITS BY LESION LEVEL # ═══════════════════════════════════════════════════════════════════════ story += [ PageBreak(), section_header("6", "NEUROLOGICAL DEFICITS BY LESION LEVEL"), space(8), body("The level of the lesion determines functional deficit — cornerstone of prognosis and counselling."), space(6), std_table( ["Lesion Level", "Key Motor Function Present", "Ambulation Prognosis"], [ ["Thoracic", "Complete paraplegia; hip flexion absent", "Wheelchair dependent"], ["High Lumbar (L1–L2)", "Hip flexors present; no knee extension", "Wheelchair; may use RGOs/braces"], ["Mid Lumbar (L3–L4)", "Quadriceps present (knee extension)", "Community ambulation with AFO"], ["Low Lumbar (L5)", "Ankle dorsiflexion present", "Good community ambulation"], ["Sacral", "Plantar flexion; intrinsic foot muscles weak", "Near-normal gait; foot deformities"], ], col_widths=[4.5*cm, 7*cm, 5.5*cm] ), space(6), info_box( "Key Principles", [ "Motor deficits AND cognitive dysfunction are BOTH correlated with lesion level — higher lesions = greater morbidity across all domains", "Local damage present at birth remains IRREVERSIBLE despite immediate surgical repair", "Sphincter involvement is universal with lumbosacral lesions (bladder + bowel)", "'Saddle block' pattern of sensory loss when sphincters are involved", ] ), source("Sources: Creasy & Resnik; Barash Clinical Anaesthesia 9e; Bradley & Daroff's Neurology"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 7 – NEONATAL ASSESSMENT & IMMEDIATE STABILISATION # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("7", "NEONATAL ASSESSMENT & IMMEDIATE STABILISATION"), space(8), subsection("Initial Evaluation Checklist at Birth"), std_table( ["Step", "Assessment", "Action / Note"], [ ["1", "Level of defect", "Count vertebral segments; correlate with expected function"], ["2", "Sac integrity", "Intact? Ruptured? CSF leaking? Open placode?"], ["3", "Neurological exam", "Spontaneous movements; response to stimulation below level"], ["4", "Head circumference", "Daily measurement; >98th centile or rapid crossing = hydrocephalus"], ["5", "Fontanelle", "Bulging = raised ICP → urgent neurosurgery"], ["6", "Cranial nerve function", "Suck, swallow, cry, eye movements (Chiari II screen)"], ["7", "Bladder assessment", "Palpate; check voiding stream; post-void residual"], ["8", "Orthopedic survey", "Foot/hip deformities; spine inspection"], ["9", "Associated anomalies", "Echocardiogram; renal ultrasound"], ], col_widths=[1.2*cm, 4.5*cm, 11.3*cm] ), space(8), subsection("Wound Care & Positioning"), bullet("Place infant <b>PRONE</b> to protect the sac — never supine before repair"), bullet("Cover open placode/sac with <b>warm, sterile saline-soaked gauze</b> — prevent desiccation"), bullet("Apply sterile non-adherent dressing; change frequently to keep moist"), bullet("Avoid diapers and direct pressure on defect"), bullet("<b>LATEX-FREE materials exclusively</b> from the first moment of contact"), space(8), subsection("Infection Prevention"), bullet("Start <b>broad-spectrum IV antibiotics</b> immediately (e.g. ampicillin + gentamicin)"), bullet("CSF leakage from ruptured sac is a direct portal for meningitis/ventriculitis"), bullet("Minimise contamination; strict aseptic technique for all procedures"), space(6), subsection("Feeding & Airway"), bullet("Bulbar dysfunction (Chiari II) may impair suck and swallow — assess carefully"), bullet("Have NGT feeding ready; observe for aspiration"), bullet("Monitor for stridor (vocal cord paralysis), apnoea, and bradycardia"), bullet("Apnoea monitor mandatory for first weeks"), source("Sources: Barash Clinical Anaesthesia 9e; Creasy & Resnik's Maternal-Fetal Medicine; Bailey & Love 28e"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 8 – SURGICAL MANAGEMENT # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("8", "SURGICAL MANAGEMENT"), space(8), subsection("A. Postnatal Repair"), bullet("<b>Timing:</b> within 24–48 hours of birth — standard of care"), bullet("Reduces risk of ventriculitis, ascending infection, progressive neurological loss"), bullet("Does NOT restore already-lost function; prevents further deterioration"), bullet("Most centres close defect + place VP shunt simultaneously if hydrocephalus present"), bullet("Some centres delay shunting until symptomatic hydrocephalus develops post-closure"), space(6), body("<b>Repair technique:</b> microsurgical dissection → detach neural placode → dural closure → fascial, subcutaneous and skin closure in layers"), space(8), subsection("B. Fetal Surgery — The MOMS Trial"), body("The landmark Management of Myelomeningocele Study (MOMS) established prenatal surgery as superior to postnatal repair in selected cases."), space(6), std_table( ["Parameter", "Prenatal Surgery", "Postnatal Surgery"], [ ["Primary outcome (death or shunt)", "Significantly REDUCED", "Standard reference"], ["VP shunt requirement", "Reduced ~50%", "64–85%"], ["Motor function at 2 years", "Better; more likely to walk", "Baseline"], ["Chiari II severity", "Reduced / reversed", "Unchanged"], ["Mean GA at delivery", "~34 weeks (preterm risk)", "~37 weeks"], ["Maternal risks", "Laparotomy, uterine scar, PPROM", "Minimal (from fetal surgery)"], ], col_widths=[5.5*cm, 6*cm, 5.5*cm] ), space(6), subsection("MOMS Trial — Selection Criteria"), bullet("Singleton pregnancy; MMC between T1 and S1"), bullet("Chiari II malformation present; normal karyotype"), bullet("19–25 weeks gestation"), bullet("Maternal surgical criteria met (no placenta praevia, BMI, uterine anomalies etc.)"), space(6), info_box( "Delivery in MMC — Mode Matters", [ "Planned CAESAREAN SECTION before onset of labour or membrane rupture is recommended", "Improved motor function shown vs vaginal delivery or CS after labour onset", "Reason: minimises additional injury to open neural elements during delivery", ], bg=colors.HexColor("#FFF3E0"), title_color=ACCENT, border=ACCENT ), space(6), info_box( "Evolving Technique — Fetoscopic (Endoscopic) Repair (2025)", [ "Several centres now performing MMC repair via fetoscopy (minimally invasive)", "Avoids full uterine incision — potentially reduces preterm delivery risk", "Torres et al. 2025 meta-analysis (PMID 41398113): confirms prenatal repair superiority; fetoscopic data accumulating", "de Oliveira Manduca Palmiero et al. 2025 (PMID 41342964): evolving neurosurgical techniques post-MOMS", ], bg=colors.HexColor("#E8F5E9"), title_color=GREEN, border=GREEN ), source("Sources: Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anaesthesia 10e; Barash Clinical Anaesthesia 9e"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 9 – UROLOGICAL MANAGEMENT # ═══════════════════════════════════════════════════════════════════════ story += [ PageBreak(), section_header("9", "UROLOGICAL MANAGEMENT", color=MID_BLUE), space(8), warning_box( "End-stage renal disease (ESRD) is the COMMONEST cause of death in children with spina bifida — " "urological surveillance is a TOP PRIORITY from birth" ), space(6), subsection("Neuropathic Bladder in MMC"), bullet("Universal with lumbosacral lesions"), bullet("<b>Detrusor-sphincter dyssynergia</b> — dangerous high bladder pressures"), bullet("If untreated: VUR → recurrent UTIs → hydronephrosis → renal scarring → ESRD"), space(6), subsection("Management Protocol"), std_table( ["Step", "Intervention", "Timing / Details"], [ ["1", "Baseline renal ultrasound + urodynamics", "Neonatal period — establish baseline"], ["2", "Clean Intermittent Catheterisation (CIC)", "Cornerstone; start early; teach family"], ["3", "Anticholinergics (oxybutynin)", "Reduce detrusor overactivity; protect upper tracts"], ["4", "Urodynamic surveillance", "Every 6–12 months initially; adjust management"], ["5", "VUR surveillance", "US + MCUG if indicated; prophylactic antibiotics or surgical correction"], ["6", "Bowel programme", "Parallel bowel management to prevent faecal loading and secondary UTIs"], ], col_widths=[1*cm, 5.5*cm, 10.5*cm] ), space(6), bullet("Note: prenatal repair associated with <b>higher rates of complete sphincter denervation</b> — urological surveillance equally important regardless of repair type"), source("Sources: Bailey & Love 28e; Campbell-Walsh Urology"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 10 – ORTHOPAEDIC COMPLICATIONS # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("10", "ORTHOPAEDIC COMPLICATIONS"), space(8), body("Progressive musculoskeletal deformities are <b>expected</b> — anticipate and refer early to orthopaedics and physiotherapy."), space(6), std_table( ["Complication", "Mechanism", "Management"], [ ["Clubfoot / calcaneal deformity", "Muscle imbalance (tibialis anterior overpowers absent plantar flexors)", "Ponseti casting ± minor posterior release; early intervention"], ["Hip dislocation / subluxation", "Muscle imbalance: hip flexors/adductors unopposed (L2–L3 level)", "Observation or surgical reduction; controversial — depends on level"], ["Knee contractures (flexion or extension)", "Spasticity + muscle imbalance", "Physiotherapy, splinting, serial casting, surgery"], ["Scoliosis / kyphosis", "Vertebral dysplasia + muscle imbalance", "Bracing early; spinal fusion for progressive curves"], ["Ankle valgus", "Tibial torsion + muscle imbalance", "Supramalleolar osteotomy"], ["Pathological fractures", "Osteoporosis from immobility; insensate limbs", "Prevention via padding; prompt recognition; DEXA surveillance"], ["Pressure sores / decubitus ulcers", "Insensate skin below lesion level", "Pressure relief, regular turning, appropriate seating and footwear"], ], col_widths=[4*cm, 6*cm, 7*cm] ), source("Sources: Campbell's Operative Orthopaedics 15e; Bailey & Love 28e"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 11 – COGNITIVE & NEURODEVELOPMENTAL OUTCOMES # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("11", "COGNITIVE & NEURODEVELOPMENTAL OUTCOMES"), space(8), std_table( ["Outcome Measure", "Data"], [ ["IQ >80 in long-term survivors", ">70%"], ["Independent living as adults", "~37%"], ["Mean IQ in VP-shunted patients", "~80 (low normal)"], ["IQ impact of shunt complications", "Significantly lower"], ["Higher lesion level effect", "Worse cognitive outcomes as well as motor"], ["Typical cognitive profile", "Verbal skills relatively preserved; visuospatial and executive function impaired ('cocktail party speech')"], ["Other cognitive domains", "Attention, memory, processing speed commonly affected"], ], col_widths=[6*cm, 11*cm] ), space(6), info_box( "Neurodevelopmental Surveillance Plan", [ "Enrol in early intervention programme from birth", "Formal developmental assessment at 6, 12, 18, 24 months then annually", "Educational psychologist input before school entry", "Monitor for hydrocephalus-related cognitive decline (shunt malfunction signs)", "Occupational therapy for fine motor and ADL development", ] ), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 12 – MULTIDISCIPLINARY TEAM # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("12", "MULTIDISCIPLINARY TEAM (MDT)"), space(8), std_table( ["Specialty", "Role"], [ ["Neurosurgery", "Defect closure, VP shunting, tethered cord release, Chiari decompression"], ["Neonatology", "Immediate stabilisation, infection prevention, feeding support, apnoea monitoring"], ["Urology / Nephrology", "Bladder management (CIC, urodynamics), renal surveillance, VUR management"], ["Orthopaedics", "Deformity prevention and correction (foot, hip, spine)"], ["Physiotherapy", "Mobility, ambulation training, AFO fitting, strengthening"], ["Occupational Therapy", "ADL, upper limb function, assistive devices"], ["Developmental Paediatrics", "Neurodevelopmental surveillance, school readiness"], ["Dietitian", "Nutrition, obesity prevention (common due to immobility)"], ["Clinical Psychology", "Family support, child cognitive development, adjustment"], ["Continence Nurse Specialist", "CIC teaching and troubleshooting, bowel programme"], ["Social Work", "Family support, benefits, housing, respite care"], ], col_widths=[5*cm, 12*cm] ), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 13 – PREVENTION # ═══════════════════════════════════════════════════════════════════════ story += [ PageBreak(), section_header("13", "PREVENTION"), space(8), subsection("Folic Acid Supplementation"), std_table( ["Group", "Dose", "Timing"], [ ["All women of childbearing age (general population)", "0.4 mg/day", "Preconceptionally and throughout first trimester"], ["Prior NTD pregnancy", "4 mg/day (prescription required)", "Starting 1 month before conception through first trimester"], ["Women on antiepileptic drugs (valproate, carbamazepine)", "Higher dose — discuss with specialist", "AEDs impair folate absorption; increased supplementation essential"], ], col_widths=[5.5*cm, 3.5*cm, 8*cm] ), space(6), bullet("Folic acid fortification of food has reduced NTD prevalence significantly worldwide"), bullet("Rate of MMC reduced by approximately <b>50%</b> with folate supplementation"), bullet("Reduction has <b>plateaued</b> without eliminating the condition — ongoing research into non-folate-responsive NTDs"), space(6), info_box( "Other Risk Factors to Screen / Counsel", [ "Family history of neural tube defects — increased recurrence risk", "Maternal antiepileptic drug use (valproate, carbamazepine, phenytoin)", "Maternal diabetes mellitus — increased NTD risk", "Maternal obesity — independent risk factor", "Hyperthermia in first trimester (fever, hot tub use)", ], bg=colors.HexColor("#FFF3E0"), title_color=AMBER, border=AMBER ), source("Sources: Bradley & Daroff's Neurology; Harriet Lane Handbook 23e; Goodman & Gilman's Pharmacology"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 14 – PROGNOSIS # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("14", "PROGNOSIS — SURVIVAL & OUTCOME STATISTICS"), space(8), std_table( ["Outcome", "Data"], [ ["5-year mortality (all spina bifida with neonatal repair)", "~7.9% (79 per 1,000)"], ["5-year mortality (WITH brainstem dysfunction)", "~35%"], ["VP shunt requirement (lumbosacral MMC)", "64–85%"], ["Shunt complications in first year of life", "~50%"], ["IQ >80 in long-term survivors", ">70%"], ["Independent living as adults", "~37%"], ["Hydrocephalus requiring treatment", "~81%"], ["5-year mortality rate (neural tube defect births overall)", "79 per 1,000 births"], ], col_widths=[8*cm, 9*cm] ), source("Sources: Creasy & Resnik's Maternal-Fetal Medicine; Barash Clinical Anaesthesia 9e"), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 15 – CLINICAL PEARLS FOR THE NEONATOLOGIST # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("15", "10 CLINICAL PEARLS FOR THE NEONATOLOGIST", color=ACCENT), space(8), ] pearls = [ ("1. LATEX-FREE from birth", "Never use latex gloves, catheters, or IV equipment. Sensitisation starts with first exposure. Fatal anaphylaxis is preventable."), ("2. Airway alert", "Chiari II can cause vocal cord paralysis and airway obstruction. Be prepared for intubation difficulties and have a difficult airway plan."), ("3. Apnoea watch", "Central apnoea from brainstem compression can be sudden and fatal. Mandatory cardiorespiratory monitoring for first weeks."), ("4. Prone positioning", "Protect the sac at all times until surgery. Do not let it dry. Change saline-soaked dressing regularly."), ("5. CSF leak = EMERGENCY", "Ruptured sac with CSF leakage demands urgent neurosurgical consultation and immediate antibiotics. Do not delay."), ("6. Bladder triage early", "Palpate bladder; check voiding. CIC and anticholinergics may need to begin in the first week — kidneys need protection from day 1."), ("7. Cardiac screen", "Do not miss associated cardiac anomalies. Echocardiogram before surgical repair."), ("8. Feeding assessment", "Bulbar dysfunction from Chiari II impairs suck/swallow. Assess formally; have NGT ready; watch for aspiration."), ("9. Daily head circumference", "Measure every day. Rapidly crossing centiles upward = developing hydrocephalus. Alert neurosurgery early."), ("10. Family counselling", "Spina bifida is a lifelong condition. Begin honest, compassionate counselling early. Engage MDT and social support from day 1."), ] pearl_data = [[ Paragraph(f"<b>{p[0]}</b>", ParagraphStyle("ph", fontSize=9.5, textColor=DARK_BLUE, fontName="Helvetica-Bold", leading=13)), Paragraph(p[1], ParagraphStyle("pb", fontSize=9, textColor=colors.HexColor("#1A1A2E"), fontName="Helvetica", leading=13)), ] for p in pearls] pearl_table = Table(pearl_data, colWidths=[5*cm, 12*cm]) pearl_table.setStyle(TableStyle([ ("ROWBACKGROUNDS", (0,0), (-1,-1), [LIGHT_BLUE, colors.white]), ("BOX", (0,0), (-1,-1), 0.8, MID_BLUE), ("INNERGRID", (0,0), (-1,-1), 0.4, colors.HexColor("#C8D8E8")), ("TOPPADDING", (0,0), (-1,-1), 5), ("BOTTOMPADDING", (0,0), (-1,-1), 5), ("LEFTPADDING", (0,0), (-1,-1), 8), ("RIGHTPADDING", (0,0), (-1,-1), 8), ("VALIGN", (0,0), (-1,-1), "TOP"), ])) story.append(pearl_table) # ═══════════════════════════════════════════════════════════════════════ # SECTION 16 – RECENT EVIDENCE # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("16", "RECENT EVIDENCE 2023–2025"), space(8), std_table( ["PMID", "Authors / Year", "Journal", "Key Finding"], [ ["41398113", "Torres et al. 2025", "Childs Nerv Syst", "Meta-analysis: prenatal MMC repair reduces VP shunt rates and improves motor outcomes vs postnatal repair"], ["41342964", "de Oliveira Manduca Palmiero et al. 2025", "Childs Nerv Syst", "Systematic review: neurosurgical outcomes after fetal repair; fetoscopic techniques accumulating evidence"], ["38536450", "Vencio et al. 2024", "Childs Nerv Syst", "Systematic review of Chiari II surgical management — decompression outcomes"], ["40886957", "Moldenhauer et al. 2025", "Am J Obstet Gynecol MFM", "MOMS trial follow-up: reproductive outcomes after open fetal surgery for MMC"], ["41387653", "Etts et al. 2025", "Childs Nerv Syst", "Systematic review: strengths/limitations of healthcare transition programmes for spina bifida patients"], ], col_widths=[2.5*cm, 4*cm, 4*cm, 6.5*cm] ), ] # ═══════════════════════════════════════════════════════════════════════ # SECTION 17 – QUICK SUMMARY FRAMEWORK # ═══════════════════════════════════════════════════════════════════════ story += [ space(10), section_header("17", "QUICK SUMMARY FRAMEWORK", color=GREEN), space(8), ] summary_data = [ ["ANATOMY", "Failure of neural arch fusion ± neural tube closure; defect in vertebral arch"], ["TIMING", "Week 3–4 gestation; caudal neuropore = day 28 (lumbosacral predominance)"], ["TYPES", "Occulta → Meningocele → Myelomeningocele → Myeloschisis"], ["DIAGNOSIS", "MSAFP at 14–16 wks; US at 18–20 wks (Lemon + Banana signs; >95% sensitivity combined)"], ["ASSOCIATED", "Chiari II (universal), Hydrocephalus (80–90%), Tethered cord, Latex allergy"], ["NEONATAL", "Prone + sterile saline cover + antibiotics + LATEX-FREE + urgent surgery <48 hrs"], ["SURGERY", "Postnatal <48 hrs; Fetal surgery (MOMS trial) if eligible prenatally at 19–25 wks"], ["UROLOGY", "CIC + anticholinergics from birth; ESRD is leading cause of death"], ["ORTHO", "Clubfoot, hip dislocation, scoliosis — anticipate and refer early"], ["NEURO", "IQ >80 in >70% survivors; only 37% live independently as adults"], ["PREVENT", "Folic acid 0.4 mg/day all women; 4 mg/day if prior NTD pregnancy"], ] for row in summary_data: data = [[ Paragraph(row[0], ParagraphStyle("sk", fontSize=9.5, textColor=WHITE, fontName="Helvetica-Bold", leading=13)), Paragraph(row[1], ParagraphStyle("sv", fontSize=9.5, textColor=DARK_BLUE, fontName="Helvetica", leading=13)), ]] t = Table(data, colWidths=[4*cm, 13*cm]) t.setStyle(TableStyle([ ("BACKGROUND", (0,0), (0,0), GREEN), ("BACKGROUND", (1,0), (1,0), LIGHT_GREY), ("BOX", (0,0), (-1,-1), 0.5, MID_GREY), ("TOPPADDING", (0,0), (-1,-1), 5), ("BOTTOMPADDING", (0,0), (-1,-1), 5), ("LEFTPADDING", (0,0), (-1,-1), 8), ("RIGHTPADDING", (0,0), (-1,-1), 8), ("VALIGN", (0,0), (-1,-1), "MIDDLE"), ])) story.append(t) story.append(Spacer(1, 2)) # ═══════════════════════════════════════════════════════════════════════ # REFERENCES # ═══════════════════════════════════════════════════════════════════════ story += [ space(14), hr(), Paragraph("<b>References & Sources</b>", ParagraphStyle("refh", fontSize=10, textColor=DARK_BLUE, fontName="Helvetica-Bold", leading=14, spaceAfter=6)), Paragraph("1. Moore KL, Persaud TVN, Torchia MG. The Developing Human: Clinically Oriented Embryology. 11th ed.", sSrc), Paragraph("2. Daroff RB et al. Bradley and Daroff's Neurology in Clinical Practice. 8th ed.", sSrc), Paragraph("3. Creasy RK et al. Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice. 9th ed.", sSrc), Paragraph("4. Gropper MA et al. Miller's Anaesthesia. 10th ed.", sSrc), Paragraph("5. Barash PG et al. Barash, Cullen, and Stoelting's Clinical Anaesthesia. 9th ed.", sSrc), Paragraph("6. Williams NS et al. Bailey & Love's Short Practice of Surgery. 28th ed.", sSrc), Paragraph("7. Wein AJ et al. Campbell-Walsh Urology. 12th ed.", sSrc), Paragraph("8. Azar FM et al. Campbell's Operative Orthopaedics. 15th ed., 2026.", sSrc), Paragraph("9. The Johns Hopkins Hospital. The Harriet Lane Handbook. 23rd ed.", sSrc), Paragraph("10. Torres JPV et al. Outcomes in prenatal vs. postnatal surgery for myelomeningocele: a systematic review and meta-analysis. Childs Nerv Syst. 2025. PMID 41398113", sSrc), Paragraph("11. de Oliveira Manduca Palmiero H et al. Fetal myelomeningocele repair after the MOMS trial. Childs Nerv Syst. 2025. PMID 41342964", sSrc), Paragraph("12. Vencio RCC et al. Surgical management of Chiari II malformation: a systematic review. Childs Nerv Syst. 2024. PMID 38536450", sSrc), Paragraph("13. Moldenhauer JS et al. Reproductive outcomes following open maternal-fetal surgery for MMC closure: analysis of MOMS trial participants. Am J Obstet Gynecol MFM. 2025. PMID 40886957", sSrc), ] # ── BUILD ──────────────────────────────────────────────────────────────────── doc.build(story, onFirstPage=on_first_page, onLaterPages=on_page) print(f"PDF created: {OUTPUT}") PYEOF echo "Script written."
cd /tmp/workspace/spina-bifida && python generate_pdf.py 2>&1
~/spina-bifida/generate_pdf.py
Successfully replaced 1 instance(s) of the string in '/tmp/workspace/spina-bifida/generate_pdf.py'
~/spina-bifida/generate_pdf.py
Successfully replaced 1 instance(s) of the string in '/tmp/workspace/spina-bifida/generate_pdf.py'
~/spina-bifida/generate_pdf.py
Successfully replaced 1 instance(s) of the string in '/tmp/workspace/spina-bifida/generate_pdf.py'
cd /tmp/workspace/spina-bifida && python generate_pdf.py 2>&1
ls -lh /tmp/workspace/spina-bifida/Spina_Bifida_Teaching_Module.pdf
Spina Bifida Teaching Module
PDF Document · PDF
| Section | Content |
|---|---|
| 1 | Definition & Overview — incidence, epidemiology table |
| 2 | Embryology & Pathogenesis — Two-Hit Model with clinical implications box |
| 3 | Classification — 4-type table + cutaneous markers of occulta + warning box |
| 4 | Prenatal Diagnosis — MSAFP + 6 ultrasound signs table (Lemon, Banana, etc.) |
| 5 | Associated Anomalies — Chiari II, Hydrocephalus, Tethered Cord, Latex Allergy |
| 6 | Neurological Deficits by Lesion Level — ambulation prognosis table |
| 7 | Neonatal Assessment & Stabilisation — step-by-step checklist table |
| 8 | Surgical Management — Postnatal repair + MOMS Trial comparison table + fetoscopy update |
| 9 | Urological Management — 6-step protocol table; ESRD warning |
| 10 | Orthopaedic Complications — 7 conditions with management |
| 11 | Cognitive & Neurodevelopmental Outcomes + surveillance plan |
| 12 | Multidisciplinary Team — 11 specialties + roles |
| 13 | Prevention — folic acid doses table + risk factors |
| 14 | Prognosis — survival statistics table |
| 15 | 10 Clinical Pearls for the Neonatologist — highlighted table |
| 16 | Recent Evidence 2023–2025 — 5 latest papers with findings |
| 17 | Quick Summary Framework — at-a-glance reference |