Chest x ray read complete guide whith images
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have enough rich content from Grainger & Allison's Diagnostic Radiology to produce a comprehensive, well-illustrated guide. Let me compile the complete guide now.
Complete Guide to Reading a Chest X-Ray
Sourced from Grainger & Allison's Diagnostic Radiology, Tintinalli's Emergency Medicine, and other major clinical textbooks in the medical library.
1. Projections and Technical Quality
Before interpreting anything, assess the film's technical quality. A poor-quality film leads to false conclusions.
Standard Projections
- PA (Posteroanterior): The standard view. Patient stands with chest against the detector, X-ray beam enters from behind. The heart appears its true size because it is close to the detector.
- AP (Anteroposterior): Used for portable/bedside films. The heart appears magnified (~15-20% larger) because it is farther from the detector.
- Lateral: Obtained at 90° to the PA. Helps localize lesions to anterior or posterior segments and assess the retrosternal and retrocardiac spaces.
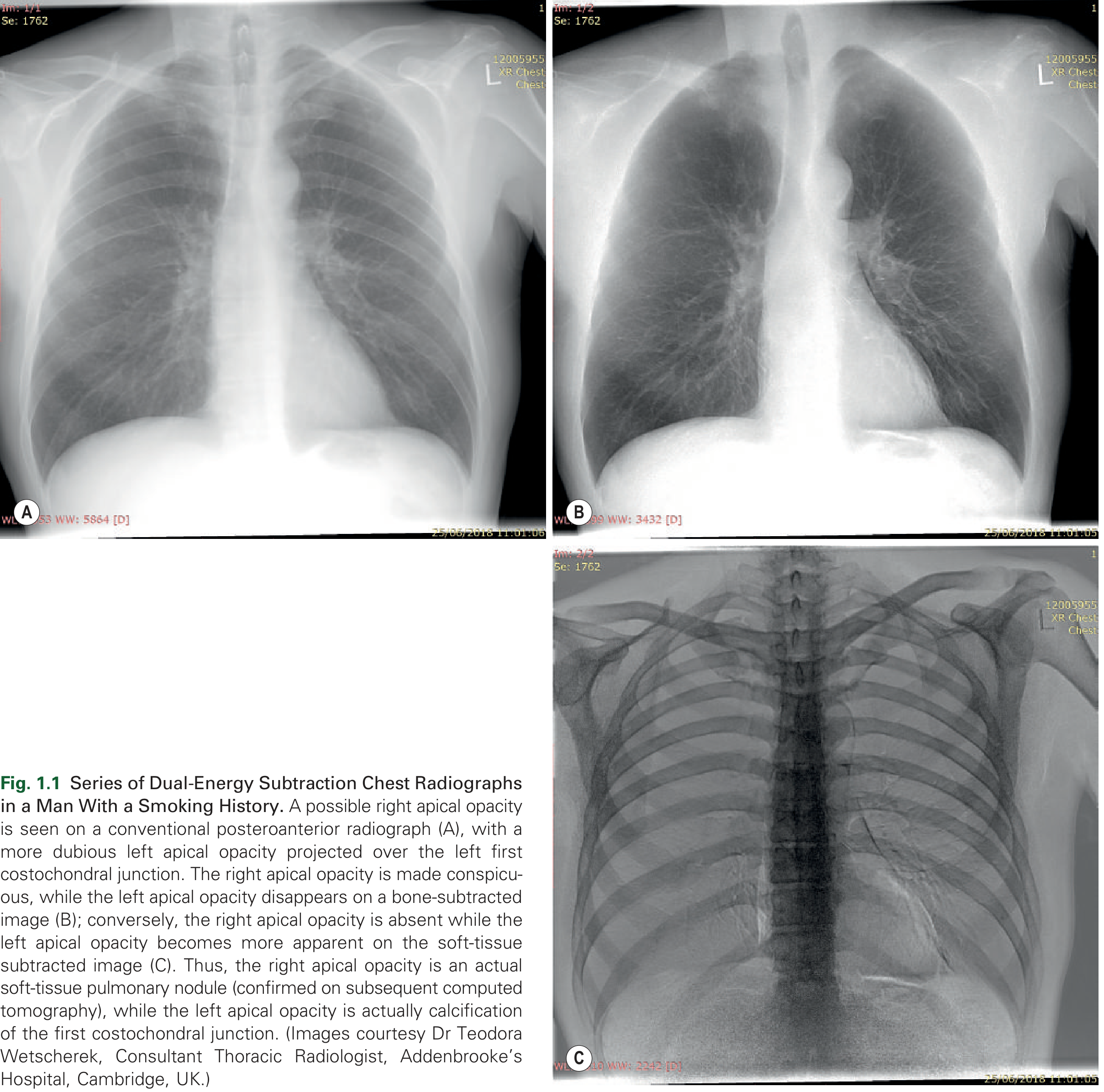
Below is a pair of PA chest radiographs showing dual-energy subtraction technique - image A is the standard PA, while image B (bone-subtracted) and C (soft-tissue subtracted) clarify whether an opacity is a true pulmonary nodule or a calcified rib/costochondral junction:
Assessing Technical Quality (RIPE mnemonic)
| Parameter | What to Check | Normal Finding |
|---|---|---|
| Rotation | Medial ends of clavicles equidistant from spinous process | Equal distance bilaterally |
| Inspiration | Count posterior ribs above diaphragm | 6 posterior ribs minimum; ideally 10 visible |
| Projection | PA vs. AP (noted on film) | PA preferred; AP noted as such |
| Exposure | Vertebral bodies visible through heart? | Yes - but not so dark that lung detail is lost |
2. Systematic Approach - "ABCDE"
Always read a chest X-ray in a consistent order to avoid missing findings. A widely used systematic approach:
A - Airways (trachea, carina, bronchi)
B - Bones and soft tissues
C - Cardiac silhouette and mediastinum
D - Diaphragm and pleura
E - Everything else (lung fields, hila, lines/tubes)
3. Airways
Trachea
- Midline or slightly right-deviated at the carina (normal, due to aortic arch).
- The right paratracheal stripe is a thin (≤5 mm) stripe visible in ~two-thirds of normals, formed by the tracheal wall and adjacent mediastinal fat. Widening suggests paratracheal lymphadenopathy or mass.
- The carina angle (subcarinal angle) is normally less than 70°. Widening suggests left atrial enlargement or subcarinal lymphadenopathy.
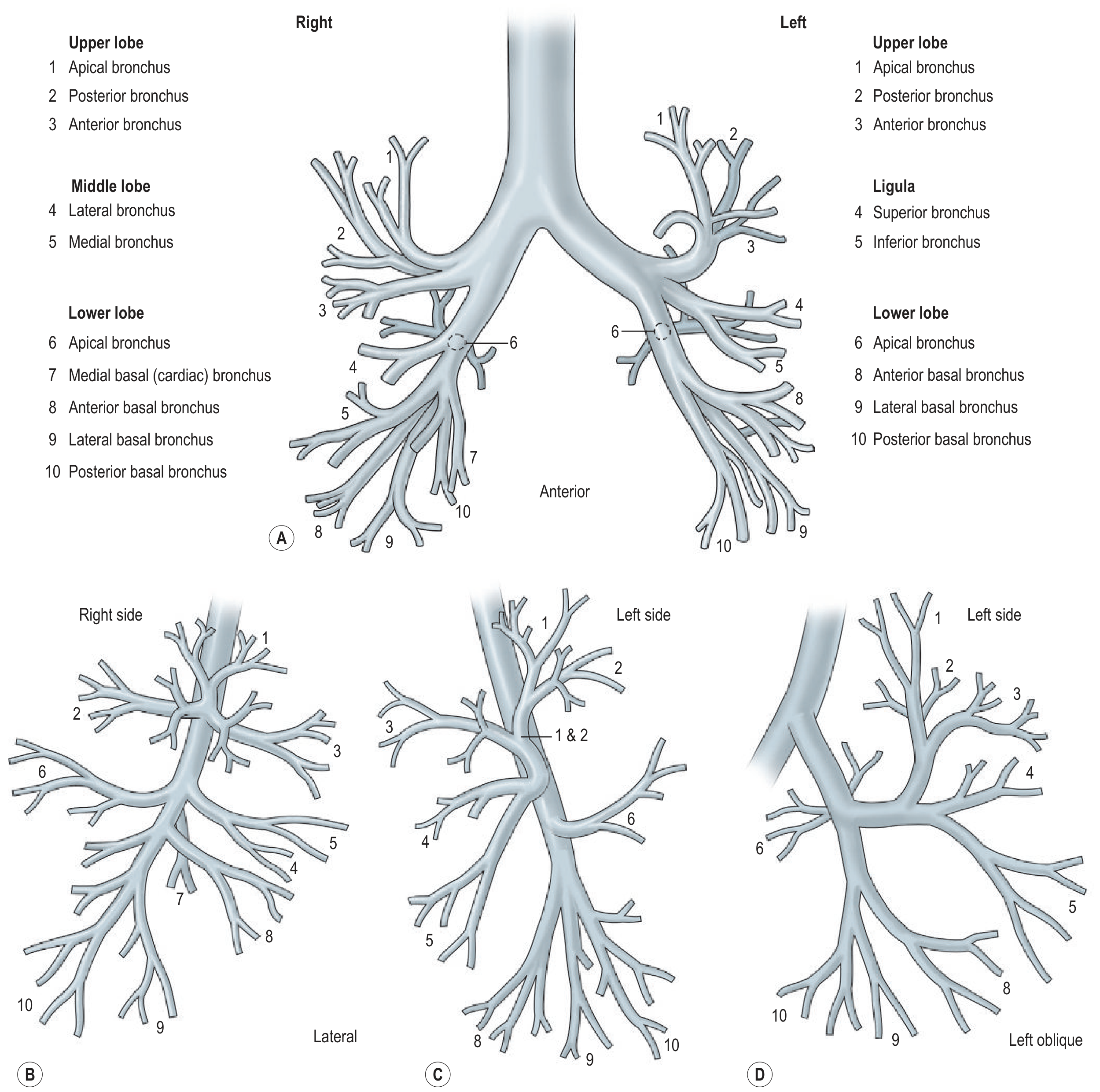
Bronchi
The anatomy of the bronchial tree is shown below. On the right, the main bronchus is shorter (before giving off the upper lobe bronchus). On the left, the main bronchus extends about twice as far before branching.
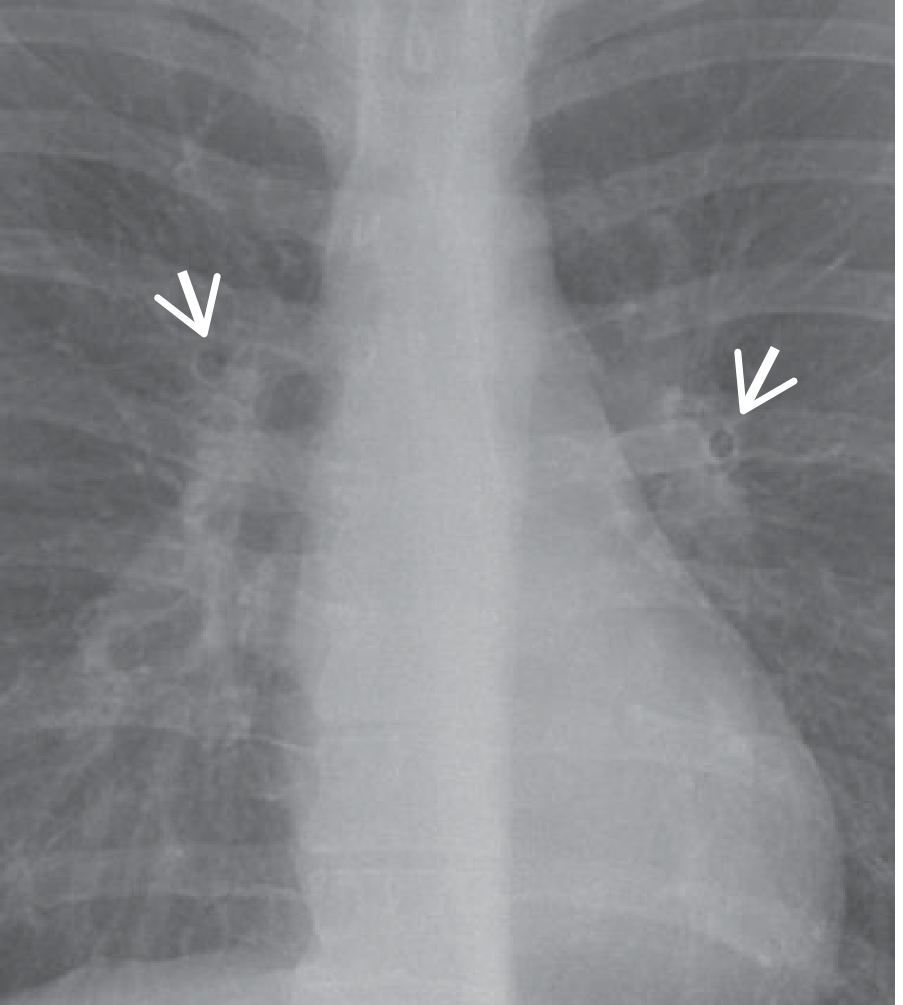
Normal bronchi are not visible in the lung periphery. When seen end-on, they create ring shadows - a normal finding:
4. Bones and Soft Tissues
Ribs
- Count ribs systematically: anterior ribs slope downward; posterior ribs are more horizontal.
- Look for fractures (including posterior rib fractures, which are harder to see than anterior ones).
- Lytic rib lesions (metastases, myeloma), sclerotic lesions, periosteal reaction.
- Key patterns:
- Lytic lesion + anterior chest wall + chondroid calcification = chondrosarcoma
- Expansile rib lesion in young patient = Ewing sarcoma or aneurysmal bone cyst
- Posterior rib "ground-glass matrix" lesion = fibrous dysplasia
- Multiple multifocal lytic lesions = myeloma or metastases
Clavicles and Sternum
- Erosion of the distal clavicle: rheumatoid arthritis, hyperparathyroidism.
- Sternal fractures are often not visible on PA film - lateral view or CT needed.
Soft Tissues
- Check for subcutaneous emphysema (linear lucencies tracking along tissue planes).
- Breast shadows (look for asymmetry suggesting mastectomy or mass).
- Skin folds from positioning can mimic pneumothorax.
- Fat pads at the cardiophrenic angles can simulate cardiomegaly if film is underexposed.
5. Cardiac Silhouette and Mediastinum
Cardiac Size
- On a PA film: measure the cardiothoracic ratio (CTR). Normal is ≤0.5 (heart width < half the widest thoracic diameter at the same level as the widest cardiac point).
- On an AP film the heart always appears larger - CTR is unreliable.
- Cardiomegaly (CTR >0.5) suggests: left ventricular dilation (heart failure, dilated cardiomyopathy, valvular disease), pericardial effusion, or right heart enlargement.
Cardiac Borders
| Border | Structure Forming It |
|---|---|
| Right upper | SVC |
| Right lower | Right atrium |
| Left upper | Aortic knuckle (arch) + pulmonary trunk |
| Left middle | Left atrial appendage |
| Left lower | Left ventricle |
Mediastinal Contours and Stripes
The diagram below shows the key mediastinal boundaries and junction lines visible on a PA CXR, with corresponding CT correlation:
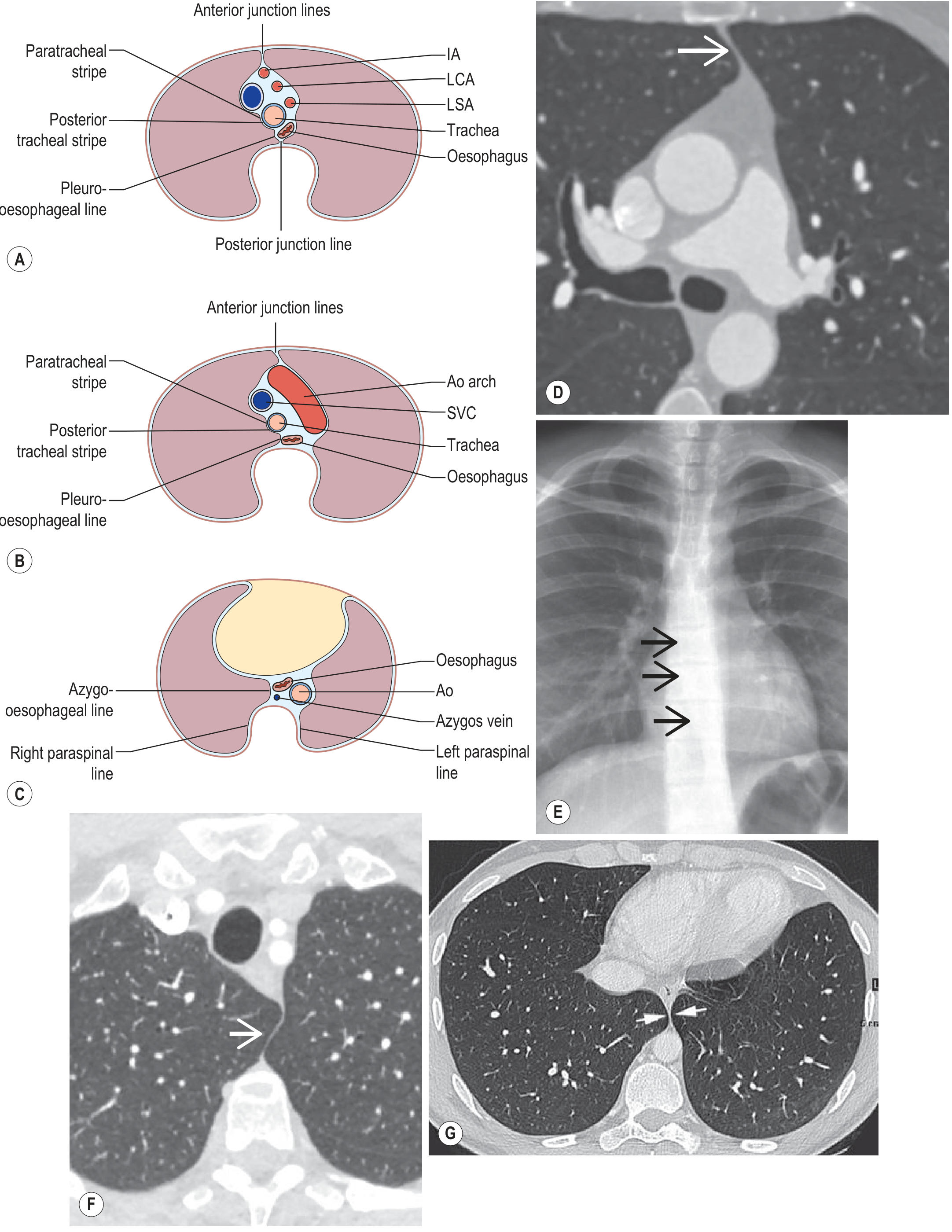
Key mediastinal landmarks:
- Right paratracheal stripe: ≤5 mm. Widening = lymphadenopathy, goiter, vascular anomaly.
- Azygos vein: Visible in the right tracheobronchial angle; ≤10 mm diameter is normal. Enlarges with raised central venous pressure (heart failure, IVC obstruction).
- Aortic knuckle: The aortic arch knob is normally visible left of the trachea. Unfolding/widening = hypertension, aneurysm. Absent/indistinct = acute aortic dissection (emergency).
- Left paraspinal line: Follows the thoracic spine. Widening or displacement = paraspinal abscess, hematoma (aortic pathology), mass.
Mediastinal Widening
Normal mediastinal width at the level of the aortic arch is less than 8 cm (PA film). Widening raises concern for:
- Aortic aneurysm/dissection
- Superior mediastinal mass (thyroid, thymoma, lymphoma, teratoma)
- Mediastinal hematoma after trauma
- Lymphadenopathy (TB, sarcoidosis, lymphoma, metastases)
The "4 T's" of anterior mediastinal masses: Thymoma, Teratoma (germ cell tumor), Thyroid mass, Terrible lymphoma.
6. Diaphragm
- The right hemidiaphragm is normally higher than the left by ~15 mm (up to 30 mm is normal).
- Both hemidiaphragms are normally smooth convex domes, with their midpoint at the level of the 5th-6th anterior rib interspace.
- The lateral costophrenic angle is a sharp acute angle - blunting indicates pleural fluid (at least 200-500 mL needed to blunt the lateral angle; posterior CP angle blunts first with smaller effusions).
Diaphragm Abnormalities
| Finding | Causes |
|---|---|
| Elevated right hemidiaphragm | Hepatomegaly, right lower lobe collapse, phrenic nerve palsy, right pleural effusion, subphrenic abscess |
| Elevated left hemidiaphragm | Gastric/splenic pathology, left lower lobe collapse, phrenic palsy |
| Bilateral elevation | Obesity, pregnancy, ascites, supine position, bilateral basal atelectasis, peritonitis |
| Flat/depressed diaphragm | Emphysema (hyperinflation), severe asthma attack |
| Diaphragmatic inversion | Tension pneumothorax, large pleural effusion, large basal bullae |
7. Pleura
Pleural Effusion
- Small amounts of free fluid initially collect under the lower lobes (subpulmonary position) and may be invisible on erect PA film.
- As volume increases:
- ~200-500 mL: blunting of the posterior then lateral costophrenic angle
- ~1000 mL: the opacity reaches the 4th anterior rib; classic concave (meniscus) upper margin, higher laterally
- Massive effusion: opacification of the entire hemithorax with contralateral mediastinal shift
The image below shows a massive left pleural effusion with CT correlation:
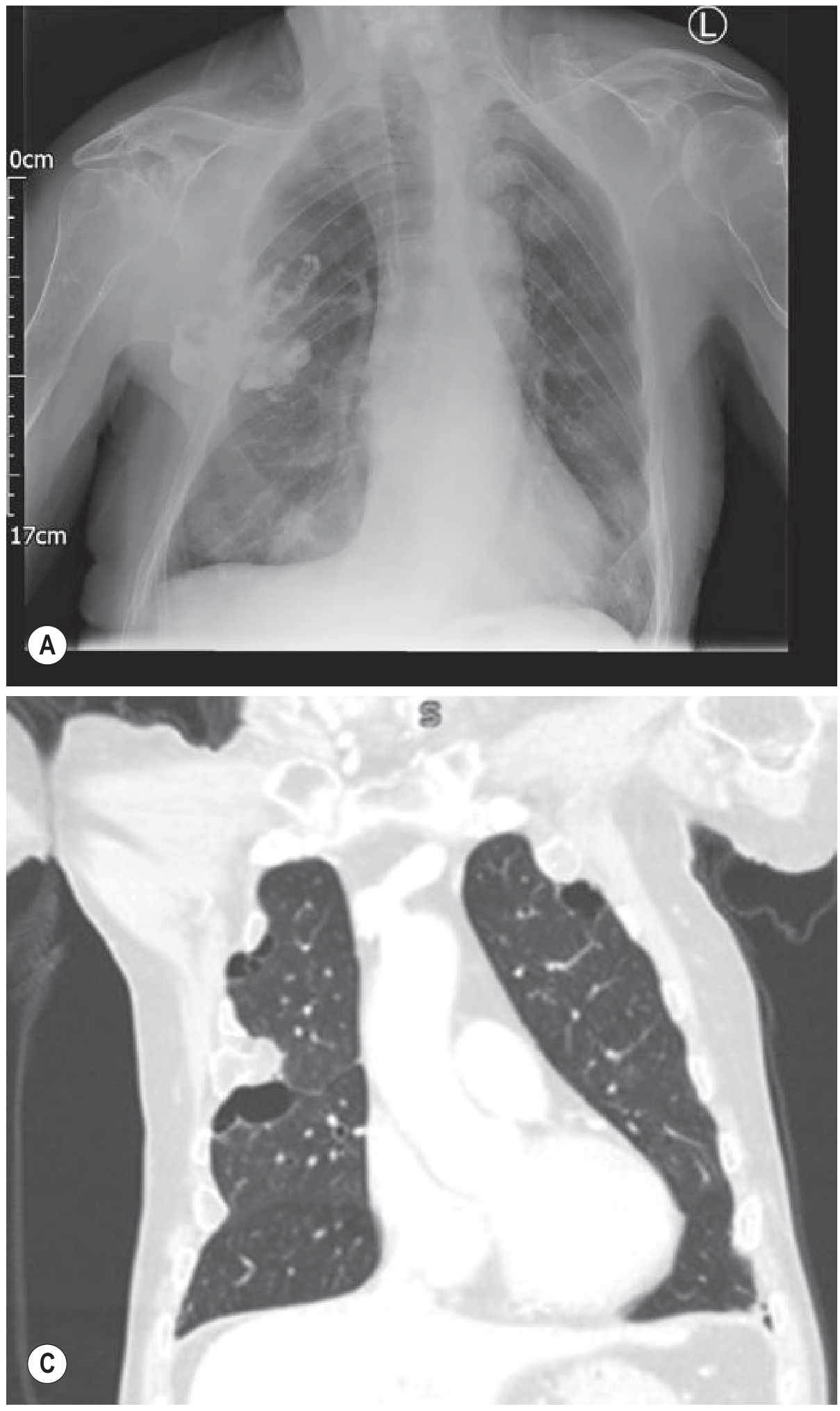
Absence of mediastinal shift with a large effusion is a red flag - suggests either ipsilateral lung collapse or extensive pleural malignancy (mesothelioma, metastatic carcinoma).
Causes of opacification of a hemithorax:
- Pleural effusion (massive)
- Consolidation (lobar pneumonia)
- Collapse
- Fibrothorax
- Combination (e.g., effusion + collapse)
Pneumothorax
- Visible as a sharp white pleural line with absent lung markings peripheral to it.
- Best seen in the apex on erect PA film. If suspected but not seen, obtain an expiratory film (accentuates the contrast) or lateral decubitus.
- On supine AP films (ICU), air collects anteriorly and inferiorly - look for the "deep sulcus sign" (abnormally deep lateral costophrenic angle).
- Tension pneumothorax: contralateral mediastinal shift, ipsilateral diaphragm depression - a clinical/radiological emergency.
8. Lung Fields and Hila
Normal Lung Markings
- Lung markings (pulmonary vessels) taper toward the periphery.
- In the erect position, vessels in the lower zones are larger than those in the upper zones (gravity-dependent blood flow).
- Upper lobe blood diversion: vessels in the upper zones appear equal to or larger than lower zone vessels - indicates raised left atrial pressure (pulmonary venous hypertension, early heart failure).
Opacification Patterns
Consolidation
- Air space opacification with air bronchograms (air-filled bronchi visible as dark tubes within the opacity).
- Typically lobar or segmental, with preserved lung volume (unlike collapse).
- Causes: pneumonia, pulmonary edema (butterfly/bat wing pattern centrally), pulmonary hemorrhage, lung contusion.
Lobar Collapse (Atelectasis)
Each lobe collapses in a predictable direction, with characteristic radiographic signs:
| Lobe | Key Signs on CXR |
|---|---|
| Right upper lobe | Elevated right hilum, triangular opacity in right apex, trachea deviated right |
| Right middle lobe | Loss of right heart border (silhouette sign), triangular opacity medially on PA |
| Right lower lobe | Loss of right hemidiaphragm silhouette, triangular opacity at right base, displaced right hilum downward |
| Left upper lobe | Veil-like opacity over left lung, loss of left heart border, aortic knuckle still visible |
| Left lower lobe | Loss of left hemidiaphragm silhouette, "sail sign" behind heart, displaced left hilum downward |
The silhouette sign is fundamental: when two structures of the same radiodensity are in contact, their shared border is lost. For example, right middle lobe consolidation (same density as heart) obliterates the right heart border.
Ground-Glass Opacification (GGO)
- Hazy increased lung density without obliteration of vascular markings (unlike consolidation).
- On HRCT it is characteristic of early interstitial disease, alveolar edema, viral pneumonitis (COVID-19), drug reactions.
Interstitial Patterns
| Pattern | Description | Common Causes |
|---|---|---|
| Reticular | Network of fine lines | IPF, interstitial edema, lymphangitis carcinomatosa |
| Nodular | Multiple discrete nodules | Miliary TB, sarcoidosis, metastases, pneumoconiosis |
| Reticulonodular | Combination of lines and nodules | Sarcoidosis, subacute HP |
| Kerley B lines | Horizontal lines at periphery, ≤2 cm long | Interstitial edema, lymphangitis carcinomatosa |
Kerley B lines represent thickened interlobular septa (the secondary pulmonary lobule boundary), visible at the lung periphery perpendicular to the pleura. They are 1-2 cm long and best seen at the lung bases laterally.
The Hila
- The left hilum is normally 0.5-1.5 cm higher than the right.
- Normal hilar shadows are formed by the pulmonary arteries and upper pulmonary veins.
- The right pulmonary artery lies anterior to the bronchi; the left pulmonary artery arches over the left main bronchus.
- Hilar enlargement: bilateral = sarcoidosis, lymphoma, bilateral hilar lymphadenopathy (BHL); unilateral = lymph node enlargement, pulmonary artery enlargement (proximal PE or pulmonary hypertension).
- Hilar displacement: upward = upper lobe collapse; downward = lower lobe collapse.
9. Lines, Tubes, and Devices
Always check position of any medical device:
| Device | Ideal Position |
|---|---|
| ETT | 3-7 cm above carina (at T2-T3 level) |
| Central venous catheter | Tip at SVC/right atrium junction |
| NG tube | Below diaphragm, left of midline (gastric body) |
| Chest drain | Apex for pneumothorax; base for effusion |
| Pacemaker lead | Right ventricular apex (RV); atrial lead = right atrial appendage |
| IABP | Tip 2-3 cm below left subclavian origin (arch of aorta) |
10. Common Abnormalities - Quick Reference
| Finding | Key X-ray Sign | Think of |
|---|---|---|
| Right heart border lost | Silhouette sign | Right middle lobe collapse/pneumonia |
| Left heart border lost | Silhouette sign | Left upper lobe/lingular collapse/pneumonia |
| "White hemithorax" + mediastinal shift away | Massive effusion | Malignancy, cardiac failure, trauma |
| "White hemithorax" + mediastinal shift toward | Collapse | Central obstructing tumor, mucus plug |
| No lung markings + white pleural line | Pneumothorax | Spontaneous (tall thin male), COPD, iatrogenic |
| Bat-wing/butterfly opacity | Bilateral perihilar consolidation | Pulmonary edema |
| Fleischer lines / Kerley B | Peripheral horizontal lines | Interstitial edema, lymphangitis |
| Bilateral hilar lymphadenopathy | Enlarged hila without cardiomegaly | Sarcoidosis (#1), lymphoma, TB, EAA |
| Cavitating lesion | Thick-walled air-containing space | Abscess, TB, squamous cell carcinoma, Wegener |
| Air under diaphragm | Free air visible on erect CXR | Bowel perforation (emergency) |
| "Sail sign" behind heart | Triangular opacity overlapping left cardiac border | Left lower lobe collapse |
11. Chest X-Ray in Trauma
Per Tintinalli's Emergency Medicine, plain CXR in trauma screens for:
- Pneumothorax (sensitivity ~50-80% vs. ~92% for ultrasound)
- Hemothorax
- Aortic/great vessel injury (mediastinal widening, obliterated aortic knuckle, tracheal deviation)
- Multiple rib fractures
- Sternal fracture (requires lateral view)
- Diaphragmatic rupture
- Pulmonary contusions
The NEXUS Chest Rules identify patients who can safely avoid imaging if ALL criteria absent: age ≤60, no rapid deceleration, no chest pain, no intoxication, normal alertness, no distracting injury, no chest wall tenderness. Sensitivity 98.8%, specificity 13.3% for thoracic injury.
12. HRCT Correlation
When plain CXR is abnormal, HRCT (1-2 mm collimation, high-spatial-frequency algorithm) is the next step for:
- Interstitial lung disease (fibrosis, EAA, sarcoidosis)
- Characterization of pulmonary nodules (volumetric assessment ≥0.6 mm)
- Pulmonary embolism (CTPA)
- Suspected bronchiectasis
- Diffuse alveolar processes
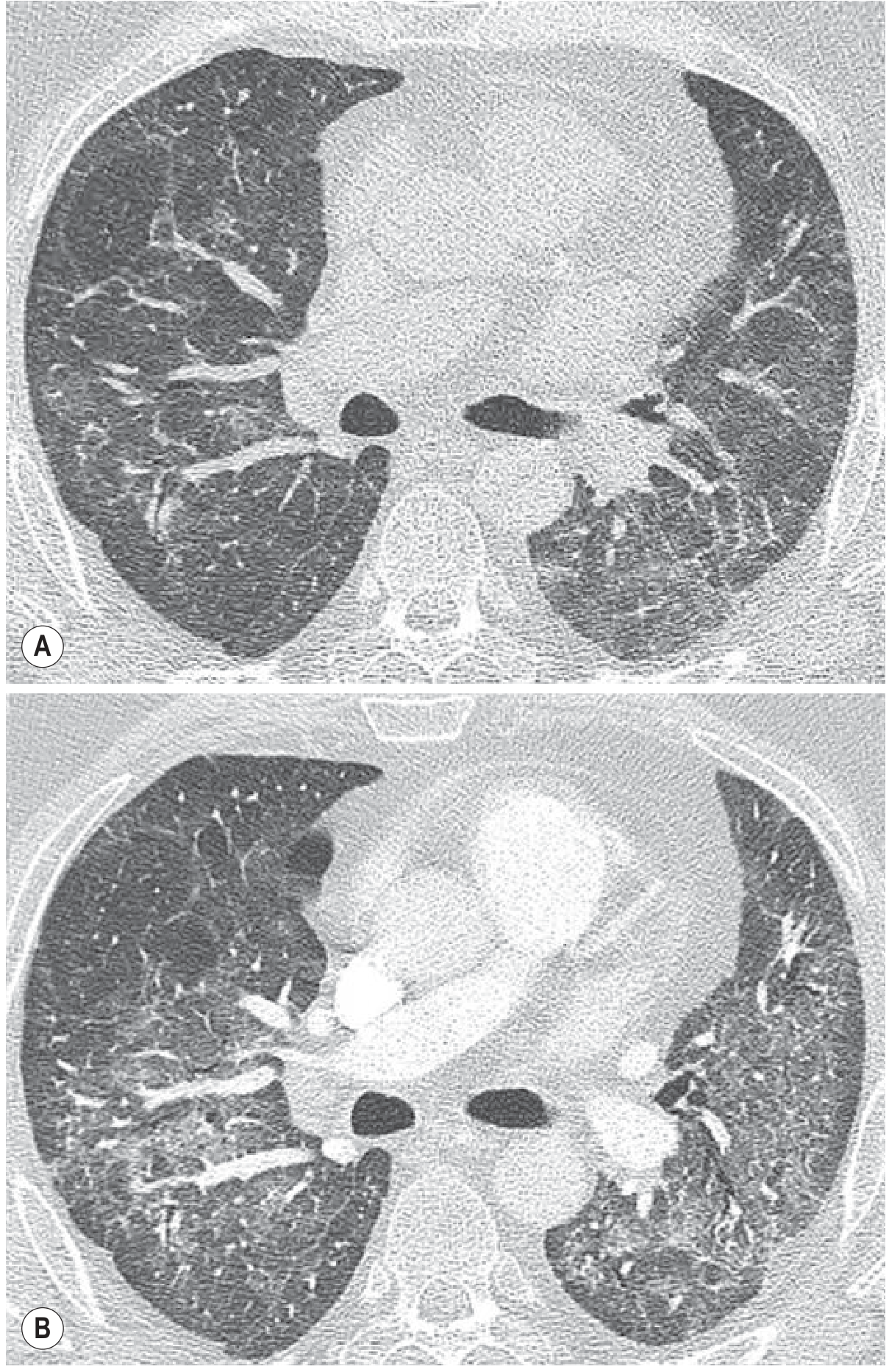
Normal HRCT lung windows vs. a patient with pathology are shown below:
Summary: A Systematic CXR Report Template
1. TECHNICAL QUALITY: PA/AP, rotation (symmetric clavicles?),
inspiration (posterior ribs visible?), exposure (vertebrae
through heart?)
2. AIRWAYS: Trachea midline? Carina angle? Paratracheal stripe?
3. BONES/SOFT TISSUES: Rib fractures? Lytic/sclerotic lesions?
Soft tissue abnormality?
4. CARDIAC: Size (CTR), borders, mediastinum width, aortic knuckle
5. DIAPHRAGM: Level (5th-6th AIS), symmetry, costophrenic angles
(sharp or blunted?)
6. PLEURA: Effusion? Pneumothorax? Pleural thickening?
7. LUNG FIELDS: Consolidation, collapse (silhouette signs),
nodules, masses, interstitial pattern
8. HILA: Left higher than right? Enlarged? Displaced?
9. DEVICES: ETT, CVC, NGT, drain positions correct?
10. EXTRAS: Sub-diaphragmatic air, surgical clips, foreign bodies
Sources: Grainger & Allison's Diagnostic Radiology (7th Ed.), Tintinalli's Emergency Medicine (9th Ed.), Roberts and Hedges' Clinical Procedures in Emergency Medicine - all accessed via the medical textbook library.
This is a shared conversation. Sign in to Orris to start your own chat.