I now have comprehensive content from the top ENT textbooks. Let me compile the full viva answer.
CSOM - Viva Questions & Answers
Based on Shambaugh Surgery of the Ear, KJ Lee's Essential Otolaryngology, Cummings Otolaryngology, and Scott-Brown's Otorhinolaryngology
1. What is CSOM? Define it.
Chronic Suppurative Otitis Media (CSOM) is defined as chronic inflammation of the middle ear and mastoid, manifesting most commonly as hearing loss and intermittent otorrhea. It is insidious in onset and usually painless. CSOM can occur with or without cholesteatoma.
- Shambaugh Surgery of the Ear, p. 527
2. What are the types of CSOM?
| Type | Also Called | Features |
|---|
| Tubotympanic (safe/mucosal) | Inactive mucosal | Central TM perforation, mucopurulent discharge, no cholesteatoma, not dangerous |
| Atticoantral (unsafe/squamous) | Active squamous | Marginal/attic perforation, cholesteatoma present, dangerous - risk of complications |
- Pars flaccida retraction leads to atticoantral type
- Pars tensa retraction leads to tubotympanic type
- KJ Lee's Essential Otolaryngology, p. 445
3. What is cholesteatoma?
A cholesteatoma is an abnormal collection of keratinizing squamous epithelium in the middle ear or mastoid. It is a destructive, expanding lesion that erodes bone through osteoclastic activity.
Types:
- Congenital - behind intact TM, no history of ear disease; white pearly mass
- Primary acquired - from retraction pocket without prior perforation
- Secondary acquired - ingrowth of squamous epithelium through a perforation
4. What are the theories of pathogenesis of cholesteatoma?
Four classical theories (Cummings Otolaryngology, p. block 31):
-
Invagination/Retraction theory (most accepted) - ET dysfunction causes negative middle ear pressure → pars flaccida (being less fibrous) retracts → keratin accumulates in deepening pocket → cholesteatoma. The pars flaccida is most susceptible.
-
Epithelial invasion/Migration theory - Squamous epithelium migrates through the margins of a TM perforation into the middle ear (secondary acquired cholesteatoma).
-
Basal cell hyperplasia/Papillary ingrowth theory - Basal layer of the tympanic membrane proliferates and invades the middle ear; supported by hyperproliferation of keratinocytes.
-
Squamous metaplasia theory - Middle ear respiratory epithelium undergoes metaplastic change to squamous epithelium under repeated inflammation.
- Mucosal traction theory (Jackler): traction from fibrotic middle ear mucosa pulls TM inward.
5. What is the most common organism in CSOM?
- Pseudomonas aeruginosa - most common pathogen in OM biofilms
- Staphylococcus aureus
- Non-typeable H. influenzae, Moraxella catarrhalis
- Often polymicrobial; organisms exist in biofilms which are highly resistant to antibiotics
Biofilms: organized networks of sessile bacteria encased in oligopolysaccharide matrix, with:
- Escape from phagocytosis and humoral immunity
- Decreased metabolic rate
- Different gene expression
- Efflux pumps for antibiotics
- KJ Lee's Essential Otolaryngology, p. 445-446
6. What is the role of Eustachian tube in CSOM?
ET dysfunction is the central pathophysiological mechanism:
- Decreased aeration of middle ear space
- Nitrogen-absorbing mastoid cells reduce middle ear volume
- Negative pressure develops in ME space
- TM retraction follows, especially at pars flaccida
- Sets the stage for cholesteatoma formation
7. What are the clinical features of CSOM?
Symptoms:
- Intermittent otorrhea - often foul-smelling (especially with cholesteatoma)
- Hearing loss - typically conductive or mixed
- Aural fullness
Warning signs (suggest complications):
- Otalgia/headache - suspect intracranial involvement or malignancy
- Vertigo - suspect labyrinthine fistula or labyrinthitis
- Facial weakness - facial nerve involvement
Signs:
- TM perforation (central in tubotympanic; marginal/attic in atticoantral)
- Granulation tissue / aural polyps (aural polyp = cholesteatoma until proven otherwise)
- Retraction pockets
- White pearly debris (cholesteatoma)
- Scutal erosion
8. What is the pathology of CSOM?
Pathological findings (Schuknecht's description):
- Osteitis - osteoclastic bone resorption; most commonly involves the incus (81%), then stapes (57%), then malleus (43%)
- Mucosal edema with submucosal gland formation (converts mucosa to secretory type)
- Granulation tissue (present in 93-98% of CSOM specimens)
- Tympanosclerosis
- Cholesterol granulomas
- TM retraction and perforation
- Sclerotic mastoid - ongoing osteitis leads to dense, narrowed mastoid bone
9. What investigations are done in CSOM?
- Otomicroscopy with pneumatic insufflation - key examination, look for cholesteatoma
- Audiometry - conductive hearing loss; CHL >30 dB suggests ossicular erosion; SNHL if labyrinth involved
- High-resolution CT scan of temporal bones - for:
- Surgical planning
- Complicated CSOM (facial nerve paralysis, vertigo)
- Cholesteatoma identified on examination
- Revision tympanomastoidectomy cases
- MRI with contrast - suspected intracranial complications; diffusion-weighted MRI to detect cholesteatoma
- Biopsy of granulation tissue unresponsive to topical therapy - to rule out malignancy
10. What is the treatment of CSOM?
Primary Goal = "Safe, Dry Ear"
- Dry = no otorrhea
- Safe = no keratin collection, reduced risk of suppurative complications
Medical Treatment:
- Aural toilet (microsuction debridement)
- Topical antibiotics (4-6 week course following debridement):
- Fluoroquinolones (ciprofloxacin - first choice, non-ototoxic)
- Polymyxin B or neomycin ± steroid
- Note: Biofilms are frequently resistant to topical antibiotics
- Systemic antibiotics if medical failure or complications
Indications for Surgery:
- Cholesteatoma + medically refractory CSOM = nearly absolute indication for surgery
- Failed multiple attempts at medical treatment
- Symptoms suspicious of complications (vertigo, facial weakness, headache)
- Retraction pockets at risk of cholesteatoma formation
11. What surgical procedures are done for CSOM?
Three primary indications for mastoidectomy:
- Eradication of disease and infection
- Approach for removal of cholesteatoma
- Establishing aeration (less important)
Types of surgery:
| Surgery | Description | Use |
|---|
| Tympanoplasty | TM repair ± ossicular reconstruction | CSOM without cholesteatoma; hearing restoration |
| CWU (Canal Wall Up) mastoidectomy | Preserve posterior EAC wall | Less extensive disease; better cosmesis; better hearing aids; less post-op care |
| CWD (Canal Wall Down) mastoidectomy | Remove posterior EAC wall; creates open cavity | Extensive cholesteatoma; lower recurrence; needs lifelong cavity care |
12. What are the complications of CSOM?
Extracranial (Intratemporal):
- Acute mastoiditis / Subperiosteal abscess
- Facial nerve paralysis
- Labyrinthitis (serous or suppurative) → vertigo, SNHL
- Labyrinthine fistula (lateral SCC most common)
- Petrositis → Gradenigo syndrome (deep retro-orbital pain + otorrhea + CN VI palsy)
- Tympanosclerosis
- Ossicular discontinuity
Intracranial:
- Meningitis (most common intracranial complication)
- Brain abscess (temporal lobe or cerebellar)
- Sigmoid sinus thrombophlebitis
- Subdural/Epidural abscess
- Otic hydrocephalus
13. What is Gradenigo syndrome?
A triad resulting from petrositis (inflammation of the petrous apex):
- Persistent otorrhea (from middle ear infection)
- Deep retro-orbital pain (CN V - trigeminal irritation)
- Diplopia / CN VI palsy (abducens nerve)
Treatment: IV antibiotics + surgical drainage.
14. What is aural polyp and its significance?
An aural polyp is granulation tissue or a polyp arising from the middle ear or EAC. It should be considered cholesteatoma until proven otherwise. Biopsy of granulation tissue unresponsive to topical therapy should be done to rule out malignancy.
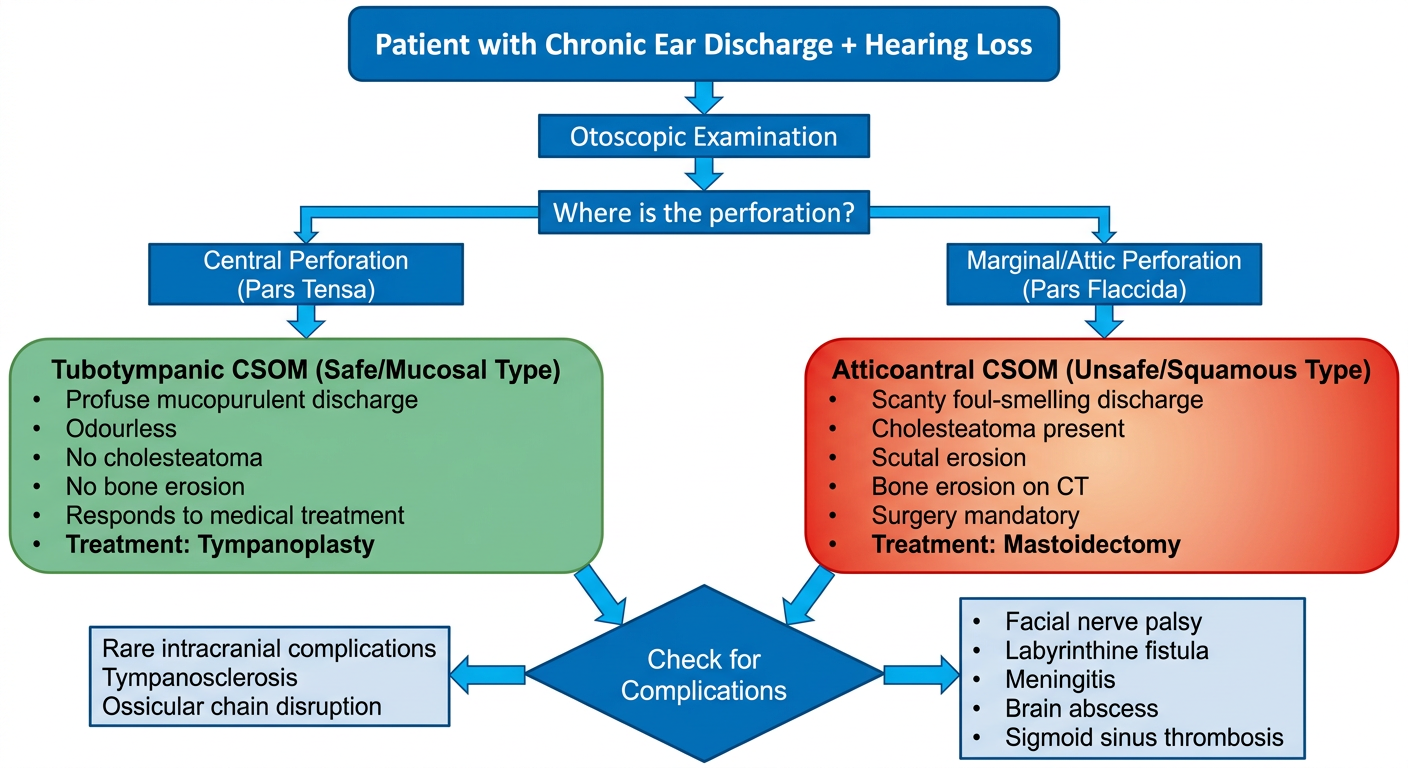
15. What is the difference between Safe and Unsafe CSOM?
| Feature | Safe (Tubotympanic) | Unsafe (Atticoantral) |
|---|
| Perforation | Central (pars tensa) | Marginal / Attic (pars flaccida) |
| Cholesteatoma | Absent | Present |
| Discharge | Mucopurulent, odourless | Foul-smelling, scanty |
| Bone erosion | Rare | Common |
| Complications | Less common | Common |
| Danger | Not dangerous | Dangerous |
| Surgery | Tympanoplasty | Mastoidectomy ± tympanoplasty |
16. What are biofilms and their relevance in CSOM?
Biofilms are highly organized, communicative networks of sessile bacteria that:
- Gain protection from changes in temperature and pH
- Escape phagocytosis and humoral immunity (impenetrable matrix)
- Are frequently polymicrobial
- Produce efflux pumps for antibiotics
- Can be intracellular (act as reservoirs)
- Are found adherent to respiratory epithelium
This explains the antibiotic resistance seen in chronic CSOM and why medical treatment often fails.
17. What hearing loss pattern is seen in CSOM?
- Conductive hearing loss (CHL) - most common
- CHL >30 dB suggests ossicular erosion
- Mixed hearing loss can occur if cochlea is affected
- Sensorineural component (5-33 dB SNHL) from bacterial toxins crossing round window, labyrinthitis, or inner ear involvement
- Interestingly, hearing can sometimes be preserved even with ossicular erosion if cholesteatoma transmits sound directly to the oval window
Sources: Shambaugh Surgery of the Ear | KJ Lee's Essential Otolaryngology | Cummings Otolaryngology | Scott-Brown's Otorhinolaryngology | Textbook of Family Medicine 9e