Glaucoma to basic to clinical
Reading File
Finding Sources
Searching PubMed
glaucoma pathophysiology treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive material from multiple authoritative sources. Let me compile the full clinical overview.
Glaucoma: From Basic Science to Clinical Practice
1. Definition
Glaucoma is an optic neuropathy in which progressive damage to retinal ganglion cells (RGCs) and their axons results in characteristic loss of the neuroretinal rim, enlargement of the optic cup, and corresponding visual field loss. The primary site of damage is at the lamina cribrosa, where optic nerve axons exit the eye. IOP is the principal modifiable risk factor, but not the sole cause - 20-50% of patients have normal IOP (normal-tension glaucoma).
- Goldman-Cecil Medicine, p. 4131 - Ganong's Review of Medical Physiology, p. 199
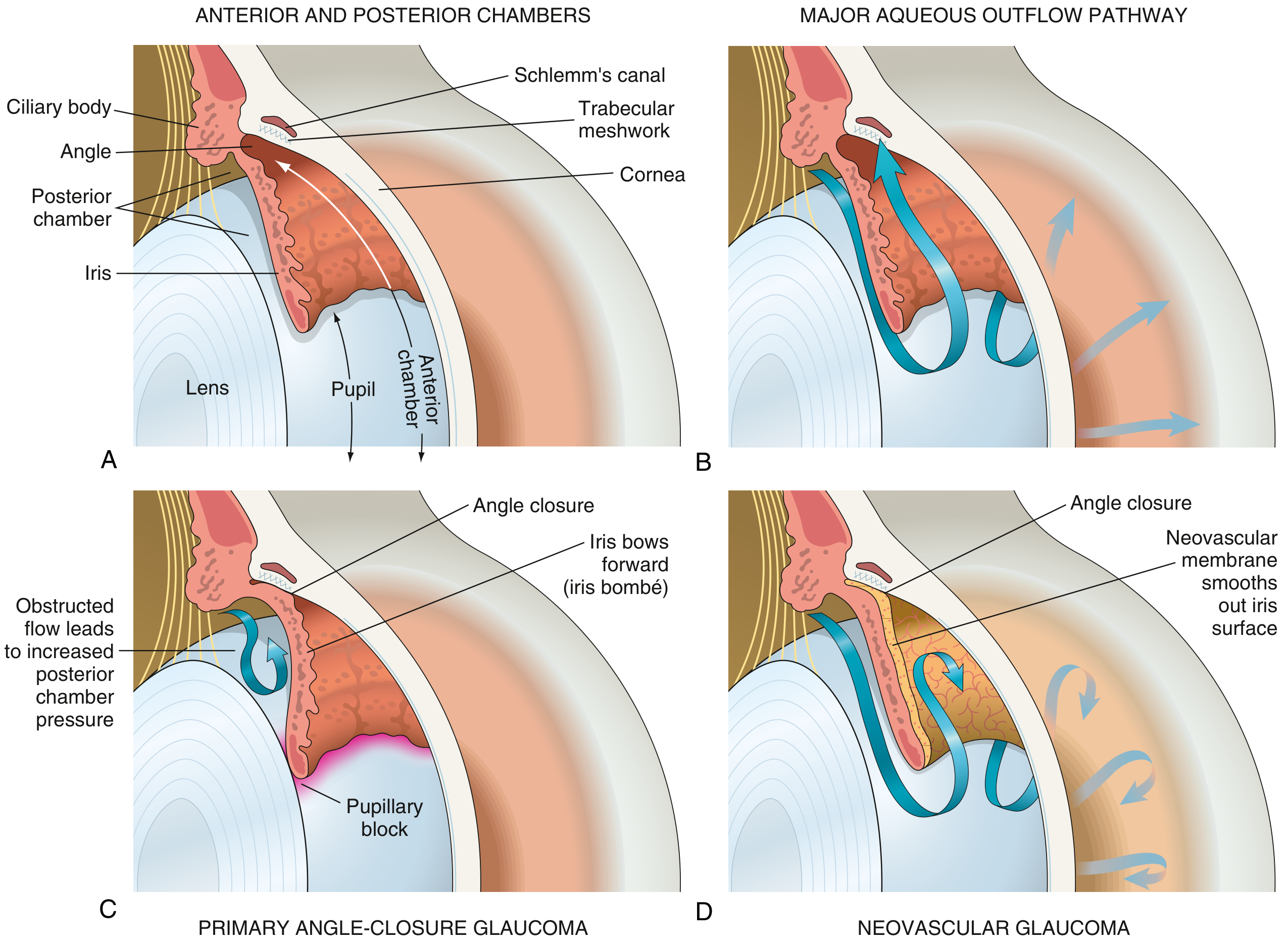
2. Basic Science: Aqueous Humor Dynamics
Production
Aqueous humor is produced by the nonpigmented ciliary epithelium of the pars plicata of the ciliary body (posterior chamber). The process involves active secretion, ultrafiltration, and simple diffusion.
Drainage - Two Pathways
| Pathway | Route | Proportion |
|---|---|---|
| Trabecular (conventional) | Trabecular meshwork → Schlemm's canal → episcleral veins | ~75-90% |
| Uveoscleral (unconventional) | Across ciliary muscle bundles → supraciliary and suprachoroidal space | ~10-25% |
When drainage fails to match production, IOP rises. Normal IOP = 10-21 mmHg (population mean ~15 mmHg; >21 mmHg = ocular hypertension by statistical definition).
IOP elevation causes:
-
Mechanical compression of RGC axons at lamina cribrosa
-
Impaired axoplasmic transport
-
Ischemia of the optic nerve head
-
Progressive RGC apoptosis
-
Goldman-Cecil Medicine, p. 4131 - Ganong's Review of Medical Physiology, p. 199
3. Classification
GLAUCOMA
├── PRIMARY
│ ├── Primary Open-Angle Glaucoma (POAG) ← most common worldwide
│ ├── Primary Angle-Closure Glaucoma (PACG) ← most common in Asia
│ └── Normal-Tension Glaucoma (NTG)
└── SECONDARY
├── Open-angle: pseudoexfoliation, pigmentary, steroid-induced, trauma
└── Angle-closure: neovascular, phacomorphic, plateau iris
4. Primary Open-Angle Glaucoma (POAG)
Epidemiology & Risk Factors
- Most prevalent type in people of European and African descent
- Prevalence in >70 year-olds: ~6% (White), ~16% (Black), ~3% (Asian)
- Affects both genders equally
Key risk factors (Kanski's Clinical Ophthalmology, p. 364):
- Elevated IOP - the higher, the greater the risk; asymmetry ≥4 mmHg is significant
- Age - older individuals at higher risk
- Race - Black patients develop POAG up to 4x more often, earlier, and more severely
- Family history - first-degree relatives: siblings ×4 risk, offspring ×2 risk
- Myopia - associated with increased incidence and susceptibility
- Large optic disc - more vulnerable to IOP-induced laminar deformation
- Low ocular perfusion pressure - vascular risk
- Anti-VEGF therapy - repeated injections (especially bevacizumab) can cause sustained IOP rise
- MYOC gene mutations - myocilin protein in trabecular meshwork; OPTN gene (optineurin) also implicated; >127 GWAS loci identified
Pathophysiology
Increased resistance to aqueous outflow at the trabecular meshwork with anatomically open anterior chamber angle. The angle appears open on gonioscopy but the trabecular cells are dysfunctional. RGCs are damaged preferentially at the superior and inferior poles of the optic disc (corresponding to arcuate nerve fiber bundles), causing characteristic arcuate visual field defects.
Optic Disc Changes (Clinical Signs)
- Neuroretinal rim (NRR) thinning - normally follows the ISNT rule (Inferior > Superior > Nasal > Temporal). Violation of this rule is suspicious.
- Cup-to-disc (C/D) ratio increase - vertical C/D >0.7 in only 2% of normal population; asymmetry ≥0.2 between eyes is suspicious
- Notching of the neuroretinal rim (especially inferotemporal or superotemporal)
- RNFL defects - wedge-shaped, best seen with red-free light
- Disc hemorrhages (splinter/Drance hemorrhages) - indicator of progression
- Peripapillary atrophy (beta-zone PPA)
Kanski's Clinical Ophthalmology, p. 228-235
Visual Field Defects (progression pattern)
- Early: Small paracentral depressions (superonasally), increased variability
- Moderate: Arcuate (Bjerrum) scotoma, nasal step (Rönne step)
- Advanced: Ring scotoma, tunnel vision, central island
- End-stage: Complete loss of central and peripheral vision
Kanski's Clinical Ophthalmology, p. 379
Diagnosis
- Tonometry (Goldman applanation) - note: corneal thickness (pachymetry) affects accuracy
- Gonioscopy - open angle confirmed
- Optic disc exam - dilated fundoscopy + OCT of RNFL
- Automated perimetry (Humphrey 24-2 or 30-2) - SAP; 10-2 for advanced
- OCT (optical coherence tomography) - RNFL thickness measurement is now standard
5. Primary Angle-Closure Glaucoma (PACG)
Mechanism
The peripheral iris mechanically occludes the trabecular meshwork (iridotrabecular contact - ITC), blocking aqueous outflow. This is called pupillary block - resistance to flow from posterior to anterior chamber causes iris bombé (forward bowing).
Predisposing anatomy: Hyperopia, shallow anterior chamber, shorter axial length, thicker lens (cataracts), plateau iris configuration.
Triggers for acute attack: Pupillary dilation (dim lighting, stress, topical or systemic mydriatics, anticholinergics, sympathomimetics, cocaine, nebulized bronchodilators).
Tintinalli's Emergency Medicine, p. 653-655
Acute Angle-Closure Crisis - Clinical Presentation
| Feature | Description |
|---|---|
| Pain | Severe, sudden-onset ocular/periorbital pain; can radiate to the jaw |
| Vision | Blurred vision, halos around lights (corneal edema) |
| Nausea/Vomiting | May mimic an acute abdomen - a diagnostic pitfall |
| Conjunctival injection | Ciliary flush (perilimbal redness) |
| Cornea | Hazy/cloudy due to epithelial edema |
| Pupil | Mid-dilated (4-6 mm), fixed, non-reactive |
| IOP | Acutely elevated, often 40-80 mmHg |
Gonioscopy Grading (Shaffer System)
- Grade 4 (35-45°): Wide open - ciliary body visible
- Grade 3 (25-35°): Open - scleral spur visible
- Grade 2 (20°): Trabeculum visible but not scleral spur - risk of closure
- Grade 1 (10°): Very narrow - only Schwalbe line visible
- Grade 0: Closed (iridocorneal contact)
Kanski's Clinical Ophthalmology, p. 389-390
6. Secondary Glaucomas
| Type | Mechanism |
|---|---|
| Pseudoexfoliation (PXF) | Abnormal fibrillogranular material (fibrillin defect) deposits on lens/trabeculum; particularly common in Scandinavians and Saudi Arabians; highest risk secondary POAG |
| Pigmentary glaucoma | Iris pigment dispersed into trabecular meshwork |
| Neovascular (NVG) | VEGF-driven neovascular membrane over iris and angle (from chronic retinal ischemia - DR, CRVO) |
| Steroid-induced | Topical/systemic steroids - IOP rise in ~5% of normal; up to 90% if positive family history of glaucoma |
| Traumatic | Red cell debris (ghost cell glaucoma), angle recession |
| Uveitic | Inflammatory trabeculitis, posterior synechiae |
| Phacomorphic | Swollen lens pushing iris forward |
Goldman-Cecil Medicine, p. 4132; Goodman & Gilman p. 1480
7. Normal-Tension Glaucoma (NTG)
IOP is within the statistically normal range (≤21 mmHg), yet characteristic glaucomatous optic nerve damage occurs. Vascular insufficiency to the optic nerve head plays a central role. The translaminar pressure gradient (difference between IOP and orbital CSF pressure) may be more important than absolute IOP. Associated with disc hemorrhages, systemic hypotension, vasospasm (migraine), and sleep apnea.
8. Pharmacology - Drug Classes for Glaucoma
All medications work by either reducing aqueous production or increasing outflow (trabecular or uveoscleral).
A) Prostaglandin Analogues (First-line)
Examples: Latanoprost 0.005%, Travoprost 0.004%, Bimatoprost 0.01%, Tafluprost
- Mechanism: FP receptor agonists → increase uveoscleral outflow
- Dosing: Once daily (evening preferred)
- IOP reduction: 25-35% (most potent single agents)
- Side effects: Increased iris/periorbital pigmentation, eyelash growth (hypertrichosis), conjunctival hyperemia, macular edema (in aphakic/pseudophakic patients)
- Contraindicated/caution: Uveitis, cystoid macular edema
B) Beta-Adrenergic Antagonists (Beta-Blockers)
Examples: Timolol 0.25-0.5% (non-selective), Betaxolol 0.5% (beta-1 selective)
- Mechanism: Block beta-2 receptors on ciliary epithelium → decrease aqueous production (~50% reduction in production)
- Dosing: Timolol 0.5% BID (most commonly used)
- IOP reduction: 20-25%
- Systemic side effects: Bradycardia, bronchospasm (contraindicated in asthma/COPD), fatigue, depression, sexual dysfunction, masking of hypoglycemia
- Local side effects: Corneal anesthesia (non-selective agents)
C) Carbonic Anhydrase Inhibitors (CAIs)
Examples: Dorzolamide 2% (topical, TID), Brinzolamide 1% (topical); Acetazolamide (systemic, 250-500 mg oral/IV)
- Mechanism: Inhibit carbonic anhydrase II in ciliary epithelium → reduce aqueous secretion (~15-20%)
- Use: Topical as second/third-line; systemic acetazolamide for acute angle-closure emergency
- Side effects - topical: Local stinging, bitter taste, corneal edema (in endothelial disease)
- Side effects - systemic (acetazolamide): Paresthesias (very common), metabolic acidosis, hypokalemia, renal stones, aplastic anemia (rare), sulfonamide cross-reactivity - contraindicated in sulfa allergy
D) Alpha-2 Adrenergic Agonists
Examples: Brimonidine 0.1-0.2%, Apraclonidine
- Mechanism: Alpha-2 stimulation → decrease aqueous production + increase uveoscleral outflow
- Dosing: Brimonidine TID
- IOP reduction: ~20-25%
- Side effects: Allergic conjunctivitis (up to 10-15%), drowsiness (crosses BBB), dry mouth
- Contraindicated: Neonates/infants (CNS depression - apnea risk), MAO inhibitor users
E) Rho-Kinase (ROCK) Inhibitors (Newest Class)
Example: Netarsudil 0.02% (once daily)
- Mechanism: Inhibit ROCK → relax trabecular meshwork cells → increase conventional (trabecular) outflow + reduce episcleral venous pressure
- IOP reduction: ~20%
- Side effects: Conjunctival hyperemia, corneal verticillata (whorl-like deposits), subconjunctival hemorrhage
- Note: First drug class to directly target trabecular meshwork outflow
F) Cholinergic Agonists (Miotics) - Largely Historical
Examples: Pilocarpine 1-4%, Carbachol, Physostigmine
- Mechanism: M3 receptor → ciliary muscle contraction → opens trabecular meshwork → increases conventional outflow; also causes pupillary constriction (helpful in angle closure)
- Side effects: Miosis (reduced vision in dim light, especially with posterior subcapsular cataract), brow ache, induced myopia, risk of retinal detachment
- Current use: Pilocarpine still used in acute angle-closure to break the attack (miosis pulls iris away from angle)
G) Combination Products
- Timolol + Dorzolamide (Cosopt)
- Timolol + Brimonidine (Combigan)
- Timolol + Latanoprost (Xalacom)
- Reduces drop burden and improves adherence
Goodman & Gilman Pharmacological Basis of Therapeutics, pp. 1480-1481; Ganong's Physiology, p. 199
9. Non-Pharmacological Treatment
Laser Therapy
1. Selective Laser Trabeculoplasty (SLT)
- Applies energy to trabecular meshwork → macrophage-mediated remodeling → improved outflow
- Can be considered first-line for POAG (as effective as medications in many patients per the LiGHT trial)
- Repeatable; takes ~4-6 weeks for full effect
- A 2024 systematic review and meta-analysis (PMID 39018052) confirmed SLT is non-inferior to medical therapy for open-angle glaucoma/ocular hypertension
2. Laser Peripheral Iridotomy (LPI)
- Creates a small hole in peripheral iris → bypasses pupillary block → equalizes pressure between chambers
- Definitive treatment for acute angle-closure crisis and prophylaxis for fellow eye
- Nd:YAG laser most commonly used
3. Laser Iridoplasty
- Used for plateau iris syndrome (not corrected by LPI alone)
Surgical Treatment
Trabeculectomy (Guarded Filtering Surgery)
- Gold-standard surgical procedure
- Creates a fistula from anterior chamber to subconjunctival space (bleb)
- Antimetabolites (Mitomycin C, 5-FU) applied intraoperatively to prevent scarring and bleb failure
- Risk of hypotony, bleb-related infection (blebitis, endophthalmitis)
Glaucoma Drainage Devices (Tube Shunts)
- Ahmed, Baerveldt, Molteno valves
- Tube from anterior chamber to an episcleral reservoir plate
- Used in refractory cases, neovascular glaucoma, failed trabeculectomy
- A 2025 meta-analysis (PMID 39394492) compared PreserFlo MicroShunt vs trabeculectomy - similar IOP control with a favorable safety profile for MicroShunt
Minimally Invasive Glaucoma Surgery (MIGS)
- iStent, Hydrus microstent, goniotomy, trabectome
- Lower efficacy than trabeculectomy but much safer - suited for mild-moderate POAG often combined with cataract surgery
Cyclodestructive Procedures
- Diode laser cyclophotocoagulation/cycloablation
- Destroys ciliary body to reduce aqueous production
- Reserved for refractory/end-stage cases or blind painful eyes
Kanski's Clinical Ophthalmology; Goldman-Cecil Medicine, p. 4133
10. Acute Angle-Closure - Emergency Management
This is an ophthalmologic emergency. IOP can exceed 60-80 mmHg, risking permanent vision loss within hours.
Step-wise approach:
-
Immediate IOP-lowering:
- Acetazolamide 500 mg IV (or 2 × 250 mg oral if IV unavailable)
- Topical timolol 0.5% - one drop
- Topical alpha-agonist (apraclonidine or brimonidine)
- IV mannitol 1-2 g/kg if IOP remains very high (osmotic agent)
-
Pupillary constriction:
- Pilocarpine 2-4% - once IOP begins to fall below ~40 mmHg (at very high IOP, sphincter is ischemic and pilocarpine is ineffective)
-
Definitive treatment:
- Nd:YAG laser iridotomy as soon as cornea clears
- Fellow eye treated prophylactically
- Lens extraction may be preferred in patients with significant cataract (lens contributes to angle crowding)
Tintinalli's Emergency Medicine, p. 655-680; Goldman-Cecil Medicine, p. 4133
11. Monitoring and Target IOP
A target IOP is individualized based on:
- Severity of existing damage (C/D ratio, mean deviation)
- Baseline IOP
- Central corneal thickness (CCT) - thin cornea falsely underestimates true IOP
- Rate of progression
- Patient age and life expectancy
A commonly used initial goal: IOP < 18 mmHg (based on AGIS data showing minimal progression below this level). If damage progresses despite target IOP, the target is lowered further, and surgical intervention considered.
A 2025 network meta-analysis (PMID 40701331) in Ophthalmology evaluated efficacy and drug interactions of glaucoma medications, confirming prostaglandin analogues as the most potent class for IOP reduction.
12. Key Clinical Pearls
| Pearl | Detail |
|---|---|
| Glaucoma = silent thief of sight | 40-50% of RGCs can be lost before visual field defect detected on standard perimetry |
| IOP fluctuation matters | Diurnal variation and peak IOP may be more important than single readings |
| Thin cornea | Underestimates IOP by Goldman applanation - higher true IOP than measured |
| Asymmetric disc cupping | ≥0.2 C/D asymmetry between eyes - always investigate |
| ISNT rule violation | Inferior rim narrowest (rather than broadest) is highly suspicious |
| Disc hemorrhage | Splinter hemorrhage at optic disc margin = early warning of progression; common in NTG |
| Angle-closure mimic | Severe nausea/vomiting may mislead to GI workup - always check IOP in sudden severe eye pain |
| Steroids cause glaucoma | Any patient starting long-term steroids needs IOP monitoring; risk much higher with glaucoma family history |
| NTG vascular link | Low blood pressure + nocturnal hypotension are treatable contributing factors |
| Bilateral disease | After unilateral angle-closure, the fellow eye has ~50% lifetime risk - treat prophylactically |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed.
- Goldman-Cecil Medicine International Edition (2025)
- Robbins & Kumar Basic Pathology
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Ganong's Review of Medical Physiology, 26th Ed.
- Tintinalli's Emergency Medicine: A Comprehensive Study
- Recent evidence: SLT vs medical therapy meta-analysis [PMID 39018052]; PreserFlo vs trabeculectomy meta-analysis [PMID 39394492]; glaucoma drug network meta-analysis [PMID 40701331]
This is a shared conversation. Sign in to Orris to start your own chat.