Osteomyelitis
Reading File
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks plus pathology images. Here is the full structured overview:
Osteomyelitis
Osteomyelitis is inflammation of bone and marrow, virtually always secondary to infection. It ranges from an acute systemic illness to a smoldering chronic condition and requires prompt diagnosis and treatment to prevent permanent bone destruction.
Definition and Classification
| Category | Basis |
|---|---|
| By duration | Acute, Subacute, Chronic |
| By route | Hematogenous, Contiguous spread, Direct inoculation |
| By pathogen | Pyogenic (bacterial), Mycobacterial, Fungal |
| By patient | Pediatric, Adult, Diabetic foot, Post-surgical |
Routes of Infection
Three main routes bring organisms to bone:
- Hematogenous spread - the most common route, especially in children
- Contiguous spread - from adjacent soft tissue infection, septic arthritis, or sinusitis
- Direct implantation - open fractures, orthopedic hardware, penetrating wounds
- Robbins & Kumar Basic Pathology, p. 779
Why the Metaphysis?
In children, hematogenous osteomyelitis preferentially involves the metaphyses of long bones (distal femur, proximal tibia, proximal humerus). The reason: terminal capillary loops in the metaphysis flow slowly, making turbulence and microtrauma ideal conditions for bacterial seeding during bacteremia. In neonates and infants, metaphyseal vessels still penetrate the growth plate, so epiphyseal and joint involvement is more common.
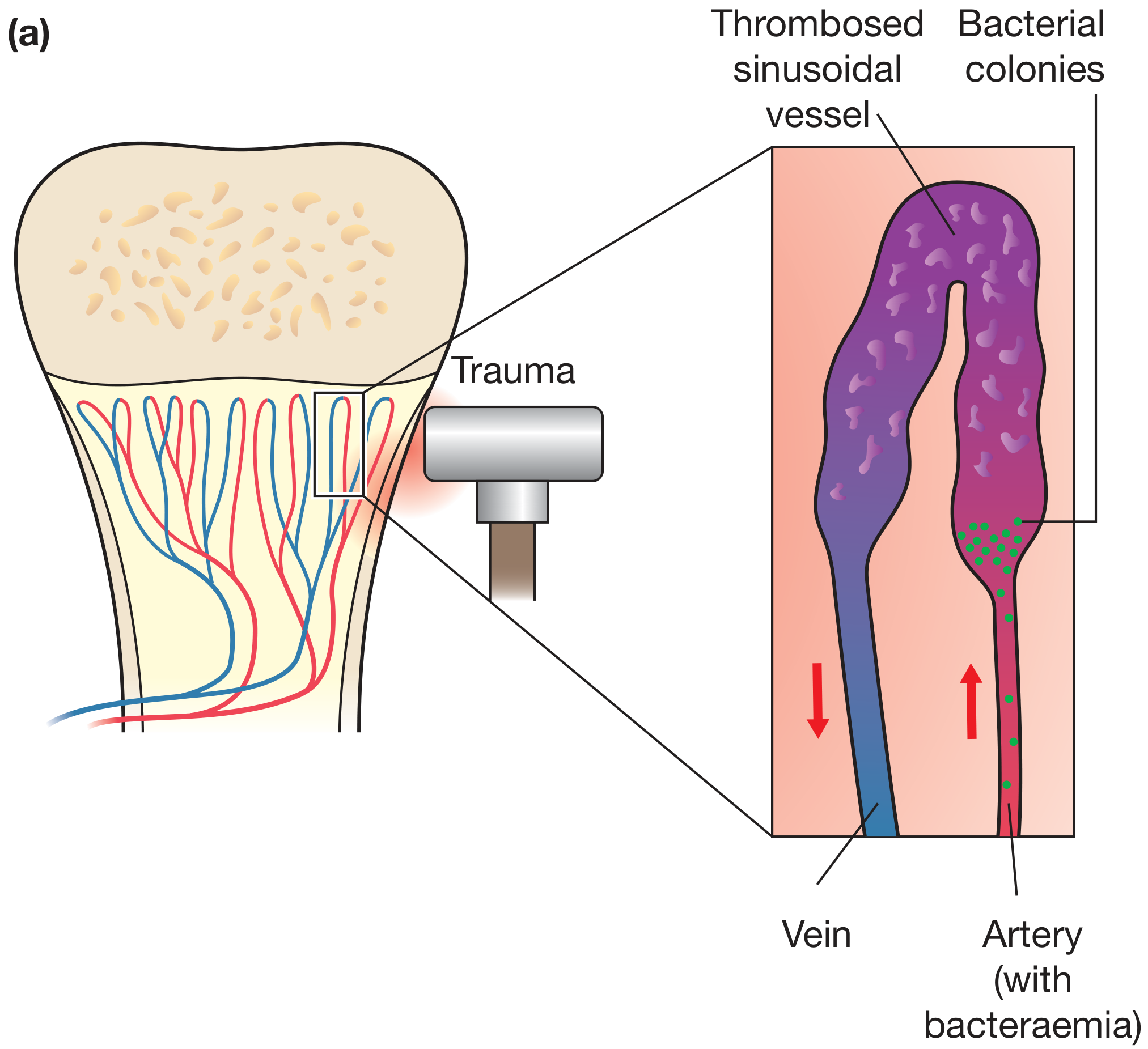
Figure: Trauma to the metaphysis causes slow flow/thrombosis of sinusoidal vessels; bacteria from the artery seed the area and proliferate - Bailey and Love's Short Practice of Surgery 28th Ed.
Microbiology
| Clinical Setting | Most Likely Organism(s) |
|---|---|
| Neonates | Group B Streptococcus, E. coli |
| Children (>1 year) | S. aureus, Streptococcus pyogenes, H. influenzae |
| Adults (general) | S. aureus (most common overall) |
| Diabetic foot / Direct spread | Mixed organisms, gram-negatives |
| Sickle cell disease | Salmonella (most common), S. aureus, gram-negative enterics |
| Post-surgical / implant | S. aureus, Coagulase-negative Staphylococci |
| Immunocompromised | Fungal (Candida, Aspergillus), Mycobacteria |
Key point: No organism is identified in nearly 50% of patients. Staphylococcal cell wall proteins bind collagen, facilitating bone adhesion. MRSA and strains carrying the Panton-Valentine leukocidin (PVL) gene are associated with increased morbidity.
- Robbins & Kumar Basic Pathology, p. 779
Pathology and Stages
Acute Phase (0-48 hours)
- Bacteria proliferate → neutrophilic infiltration
- Bone cell and marrow necrosis within 48 hours
- Infection spreads via Haversian canals through cortex to periosteum
- Periosteum elevates → subperiosteal abscess → further vascular compromise
Progression
- Pus tracks through cortex, elevates periosteum, renders cortical bone avascular
- Rupture of periosteum → soft tissue abscess → may reach skin as draining sinus
- Epiphyseal spread → septic arthritis with articular cartilage destruction
Chronic Phase (after 1+ week)
- Cytokines from chronic inflammatory cells drive osteoclastic resorption
- Dead devitalized bone = sequestrum
- Reactive new bone shell around the sequestrum = involucrum ("bone-within-a-bone")
- Chronic osteomyelitis histology: marrow fibrosis, sequestrum, lymphocytic and plasma cell infiltrate
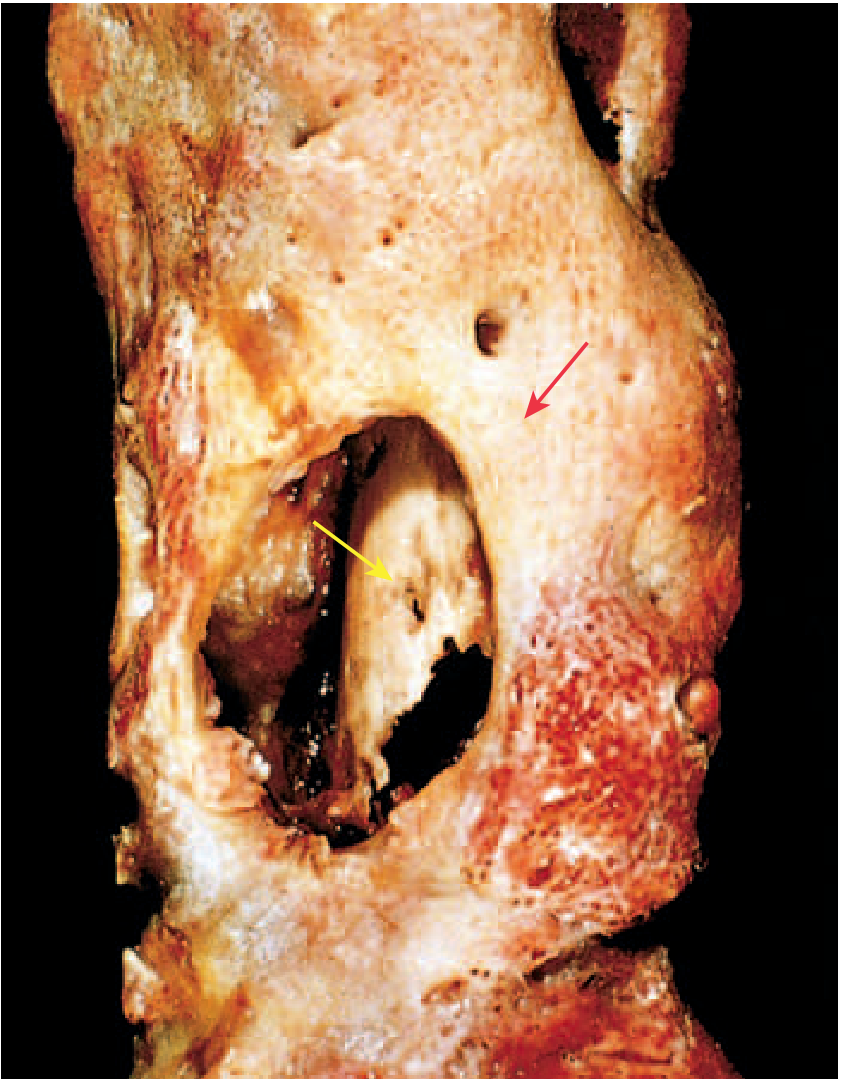
Figure: Resected femur in draining osteomyelitis. The involucrum (yellow arrow) is the shell of viable new bone; the sequestrum (red arrow) is the original necrotic cortex - Robbins & Kumar Basic Pathology
Brodie abscess = a well-defined lytic lesion with a sclerotic rim, seen in subacute/chronic infection.
Clinical Features
| Setting | Presentation |
|---|---|
| Acute hematogenous (child) | Fever, malaise, leukocytosis, throbbing local pain, limb swelling/tenderness |
| Adult / insidious onset | Localized pain only; fever may be absent |
| Infants | Unexplained fever, pseudoparalysis of the limb |
| Chronic | Draining sinus, recurrent flare-ups after years of dormancy |
| Vertebral (Pott's disease) | Back pain, fever, weight loss; may present as psoas abscess |
Important differentials:
- Septic arthritis (coexisting metaphyseal osteomyelitis must always be considered if joint aspirate is negative for organisms)
- Bone infarction in sickle cell disease (identical clinical picture; empiric antibiotics recommended until differentiated)
- Ewing sarcoma (especially in children - can mimic osteomyelitis clinically and radiologically)
Investigations
Laboratory
- CBC: leukocytosis, elevated ESR, CRP
- Blood cultures (positive in ~50% of hematogenous cases)
- Bone biopsy with culture - gold standard for organism identification
Imaging
| Modality | Finding | Notes |
|---|---|---|
| Plain X-ray | Lytic destruction, periosteal reaction, soft-tissue swelling | Changes lag 10-21 days behind onset |
| Ultrasound | Subperiosteal abscess, fluid collection | Best for infants; guides aspiration |
| Bone scintigraphy (Tc-99m) | Hot spots; useful for multifocal disease | Less specific; affected by infarction in sickle cell |
| CT | Cortical destruction, sequestra | Good for surgical planning; radiation cost |
| MRI | Bone marrow edema, abscess, soft tissue extension | Highest sensitivity and specificity; modality of choice |
MRI pearls:
-
Penumbra sign (subacute Brodie abscess): peripheral high-signal ring of granulation tissue surrounding a low-signal abscess cavity
-
T2 high signal of reactive edema may overestimate extent
-
Fat-suppressed contrast sequences confirm abscesses and granulation tissue
-
Whole-body MRI or skeletal scintigraphy for multifocal disease in neonates
-
Grainger & Allison's Diagnostic Radiology, p. (block 14)
Special Forms
Vertebral Osteomyelitis / Pott's Disease (TB)
- Spine involved in 40% of mycobacterial osteomyelitis cases
- Breaks through intervertebral discs → affects multiple vertebrae
- Extends into soft tissue → psoas abscess
- Histology: caseating granulomas
- More destructive and resistant to control than pyogenic osteomyelitis
- TB osteomyelitis: ~1-3% of all TB cases develop osseous infection
Diabetic Foot Osteomyelitis
- Usually via contiguous spread from chronic foot ulcers
- Often mixed flora; gram-negative organisms more common
- Probe-to-bone test: positive test has high specificity for underlying osteomyelitis
Sickle Cell Osteomyelitis
- Salmonella is the most common causative organism (not S. aureus)
- Differentiating from vaso-occlusive crisis is clinically very difficult
- No single lab test or imaging modality reliably differentiates the two
- Empiric antimicrobial therapy should be started until diagnosis confirmed
Treatment
Principles
- Identify the organism (bone biopsy/culture before antibiotics if clinically stable)
- Appropriate antibiotic therapy
- Surgical drainage when pus is present
Antibiotic Therapy
- Empiric first-line: Anti-staphylococcal cover (flucloxacillin/nafcillin IV); adjust based on culture
- MRSA: Vancomycin or linezolid
- Duration: Debated - typically 4-6 weeks; some protocols allow early switch to oral if clinical and hematological improvement
- Shortened IV-to-oral regimens are for uncomplicated cases only - those clinically and hematologically improving
- MRSA and PVL-positive strains require longer or combination therapy
Surgical Indications
- Failure to respond to antibiotics
- Subperiosteal or soft tissue abscess requiring drainage
- Presence of sequestrum (chronic osteomyelitis)
- Spinal cord compromise in vertebral osteomyelitis
Supportive
- Rest and splintage of the affected limb
- Adequate analgesia
Complications
| Complication | Notes |
|---|---|
| Pathologic fracture | Structural weakness from bone destruction |
| Septic arthritis | Via direct spread through epiphysis/capsule |
| Growth disturbance | Physeal damage in children |
| Secondary (reactive) amyloidosis | Complication of longstanding chronic infection |
| Squamous cell carcinoma | In chronic draining sinus tracts (Marjolin's ulcer) |
| Sarcoma | Arising in chronically infected bone |
| Endocarditis / sepsis | Hematogenous seeding from bone focus |
| Chronicity | 5-25% of acute cases fail to resolve |
Mycobacterial vs. Pyogenic Osteomyelitis
| Feature | Pyogenic | Mycobacterial (TB) |
|---|---|---|
| Onset | Acute / subacute | Insidious (months-years) |
| Fever | High | Low-grade |
| Location preference | Metaphysis of long bones | Spine (40%), long bones |
| Disc involvement | Spared (early) | Crossed disc space |
| Histology | Neutrophils, necrosis | Caseating granulomas |
| Abscess | Subperiosteal | Psoas abscess (spine) |
| Destructiveness | Moderate | Severe, hard to control |
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition, Ch. 44
- Robbins & Kumar Basic Pathology, pp. 778-779
- Grainger & Allison's Diagnostic Radiology, Ch. 73
- Firestein & Kelley's Textbook of Rheumatology, Ch. 125
Recent evidence (2025): A systematic review and meta-analysis (PMID 40607967) identified key risk factors for osteomyelitis including diabetes, immunosuppression, prior bone surgery, and peripheral vascular disease - consistent with current clinical understanding.
This is a shared conversation. Sign in to Orris to start your own chat.