Bronchopulmonary segments anaesthetic implicaitons
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
bronchopulmonary segments diagram anatomy
Loading Image
Loading Image
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile it.
Bronchopulmonary Segments — Anaesthetic Implications
Anatomy Review
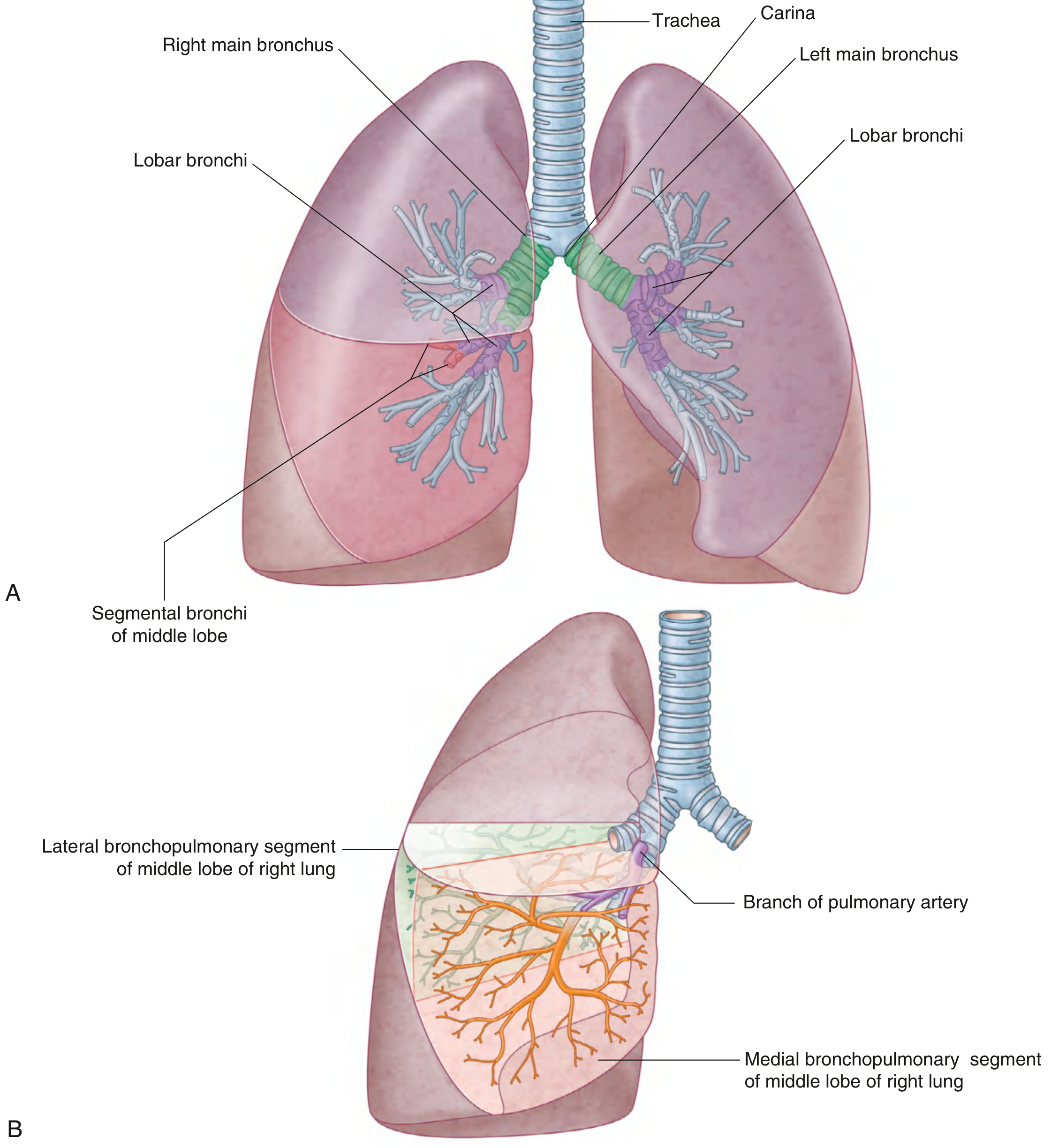
Each bronchopulmonary segment is the area of lung supplied by a segmental (tertiary) bronchus and its accompanying pulmonary artery branch. Pulmonary veins run intersegmentally, demarcating segment boundaries. Each segment is shaped like an irregular cone with its apex at the hilum and base at the pleural surface.
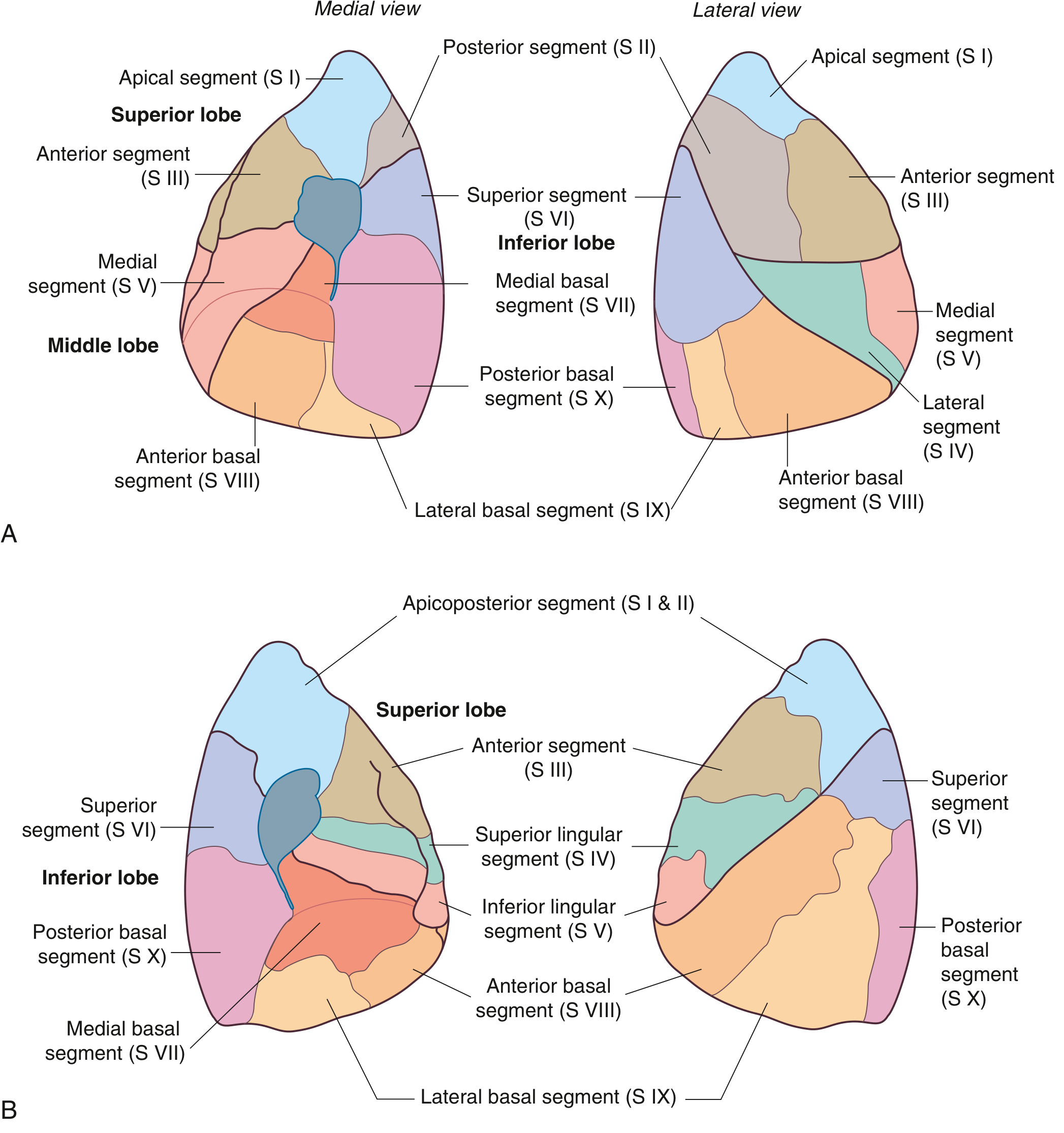
- Right lung: 10 segments (3 upper, 2 middle, 5 lower)
- Left lung: 9–10 segments (S I+II fuse → apicoposterior; S IV+V = lingula; 5 lower)
Each segment is the smallest functionally independent unit of lung that can be surgically isolated and removed without affecting adjacent regions. — Gray's Anatomy for Students
Anaesthetic Implications
1. Tracheobronchial Anatomy & Airway Management
Understanding segmental anatomy is essential for any intervention at or beyond the carina.
Key anatomical asymmetries relevant to anaesthesia:
| Feature | Right Main Bronchus | Left Main Bronchus |
|---|---|---|
| Angle from trachea | More vertical (~25°) | More horizontal (~45°) |
| Length to first branch | ~1–2.5 cm to RUL orifice | ~5 cm to bifurcation |
| Diameter | Larger | Smaller |
The right upper lobe bronchus arises only 1–2.5 cm from the carina — this short distance is the single most important anatomical consideration in thoracic anaesthesia:
- A right-sided double-lumen tube (DLT) must have a special slotted endobronchial cuff portal to allow right upper lobe ventilation; misplacement easily obstructs the RUL.
- Left-sided DLTs are preferred for most cases because the longer left main bronchus provides a larger margin for safe positioning.
— Morgan and Mikhail's Clinical Anesthesiology, 7e
2. One-Lung Ventilation (OLV) — Segment-Specific Indications
OLV is required for procedures targeting individual lobes or segments. Indications organised by whether they are patient-related or procedure-related:
| Patient-Related | Procedure-Related |
|---|---|
| Confine infection/bleeding to one lung | Segmental/lobar resection |
| Bronchopleural fistula | Pneumonectomy |
| Large bulla/cyst | Lobectomy |
| Tracheobronchial disruption | Thoracoscopy / VATS |
| Severe unilateral hypoxemia | Esophageal surgery, aortic aneurysm repair |
Techniques for OLV:
- Double-lumen bronchial tube (DLT) — most common
- Single-lumen tube + bronchial blocker (e.g., Arndt, Cohen, EZ-Blocker)
- Conventional ETT advanced into a mainstem bronchus
- Tubeless techniques (VATS with high-flow apneic oxygenation)
— Morgan and Mikhail's Clinical Anesthesiology, 7e
3. Right-Sided DLT — When Required
Despite the preference for left-sided DLTs, right-sided tubes are specifically indicated when:
- Distorted anatomy of the left main bronchus (endobronchial or exobronchial mass)
- Compression of the left main bronchus by a descending thoracic aortic aneurysm
- Left-sided pneumonectomy
- Left-sided single lung transplantation
- Left-sided sleeve resection
The right upper lobe bronchus orifice (S I, S II, S III) is at risk of occlusion — always verify with fibreoptic bronchoscopy.
— Morgan and Mikhail's Clinical Anesthesiology, 7e
4. Fibreoptic Bronchoscopy — Segment Identification
Bronchoscopic confirmation of DLT/blocker position requires knowledge of segmental orifices:
- Right side: RUL (3 segmental orifices anteriorly), RML, RLL (including apical segment S VI going posteriorly, basal segments S VII–X)
- Left side: LUL (including lingula S IV/V), LLL (apical S VI and basal S VII–X)
- The apical (superior) segment of the lower lobes (S VI) — takes off posteriorly from the LLL/RLL bronchus just below the carina equivalent — is a common blind spot during suctioning
5. Aspiration Pneumonia — Dependent Segment Localisation
The anaesthetist must recognise which segments are gravity-dependent to predict and locate aspiration injury:
- Supine patient: Most dependent segments are the posterior segments of the upper lobes (S II right, apicoposterior S I+II left) and the superior segments of the lower lobes (S VI bilaterally)
- Right lateral decubitus: Right lower lobe basal segments (S VIII–X)
- Left lateral decubitus: Left lower lobe basal segments
"Aspiration pneumonia occurs with a focal infiltrate in a dependent bronchopulmonary segment — typically the superior segment of the right lower lobe or the posterior segments of the upper lobes." — Fishman's Pulmonary Diseases and Disorders
This is clinically relevant during:
- Induction/emergence in high-risk patients (full stomach, GORD, depressed consciousness)
- Positioning changes intraoperatively
6. Surgical Resection — Segmentectomy
A segmentectomy (anatomical sub-lobar resection) exploits the natural intersegmental planes defined by the pulmonary veins. The anaesthetist must plan for:
- OLV with the operative lung collapsed
- The intersegmental vein planes used by the surgeon to divide segments — veins run between segments, not within them (unlike arteries and bronchi which are intrasegmental)
- Re-expansion of retained segments at the end — may require selective re-inflation bronchoscopically
- Air leak test: Retained segment is reinflated under saline irrigation to check staple lines
7. Lobar/Segmental Collapse — Perioperative Recognition
Knowing segment anatomy helps interpret postoperative CXR patterns:
- RUL collapse: Elevation of horizontal fissure, opacity in right upper zone
- RML collapse: Loss of right heart border (segments S IV/V are anterior and medial)
- RLL collapse: Loss of right hemidiaphragm silhouette, posterior triangular opacity
- LLL collapse (most common postop): Retrocardiac triangular opacity, loss of left hemidiaphragm silhouette; S VI (apical lower) and basal segments S VIII–X
8. Bronchial Blocker Placement for Segmental Isolation
For VATS segmentectomy or selective lobar blockade, bronchial blockers are advanced into specific lobar/segmental bronchi under fibreoptic guidance. The anatomy dictates:
- Selective blocker in RUL bronchus is technically demanding due to the short distance (~1–2.5 cm from carina to RUL orifice)
- LUL blocker is comparatively easier given the longer left main bronchus
- Blocker displacement is a common intraoperative complication requiring re-positioning under bronchoscopy
Summary Table
| Anaesthetic Scenario | Key Segment Anatomy |
|---|---|
| DLT placement — left-sided preferred | Short right main bronchus (~1–2.5 cm to RUL) |
| Right-sided DLT — RUL ventilation slot | Segments S I, II, III require portal cuff |
| Aspiration (supine) | S VI (superior lower lobes), posterior S II |
| Aspiration (right lateral) | Right basal segments S VIII–X |
| Postop atelectasis — LLL collapse | S VI + basal S VIII–X; retrocardiac shadow |
| RML collapse | S IV (lateral) + S V (medial) — right heart border |
| Segmentectomy OLV planning | Intersegmental veins = surgical planes |
| Bronchial blocker — most difficult | RUL (S I–III) due to proximity to carina |
Sources:
- Gray's Anatomy for Students — Bronchopulmonary segments, p. 208–210
- Morgan and Mikhail's Clinical Anesthesiology, 7e — Techniques for OLV, DLT anatomy, p. 1025–1028
- Color Atlas of Human Anatomy Vol. 2 — Internal Organs — Bronchopulmonary segments and lobules, p. 214
- Fishman's Pulmonary Diseases and Disorders — Aspiration pneumonia, dependent segments
This is a shared conversation. Sign in to Orris to start your own chat.