Acute epilepsy management
Reading File
Finding Sources
Searching PubMed
"status epilepticus" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Now I have comprehensive, well-sourced content. Here is a thorough summary of acute epilepsy management:
Acute Epilepsy Management
Definition & Time-Based Framework
Status epilepticus (SE) is defined operationally as a seizure lasting >5 minutes, or two or more seizures without recovery of consciousness between them. After 5 minutes, seizures are less likely to self-terminate, less responsive to drugs, and more likely to cause permanent neuronal injury. The treatment goal is seizure termination within 30 minutes of presentation.
- Convulsive SE: prominent bilateral motor activity + impaired consciousness - a life-threatening emergency
- Nonconvulsive SE (NCSE): coma or fluctuating mental status without overt convulsions; diagnosed by EEG. Less urgent but still dangerous; look for prolonged post-ictal state, subtle twitching/eye deviation, or unexplained stupor
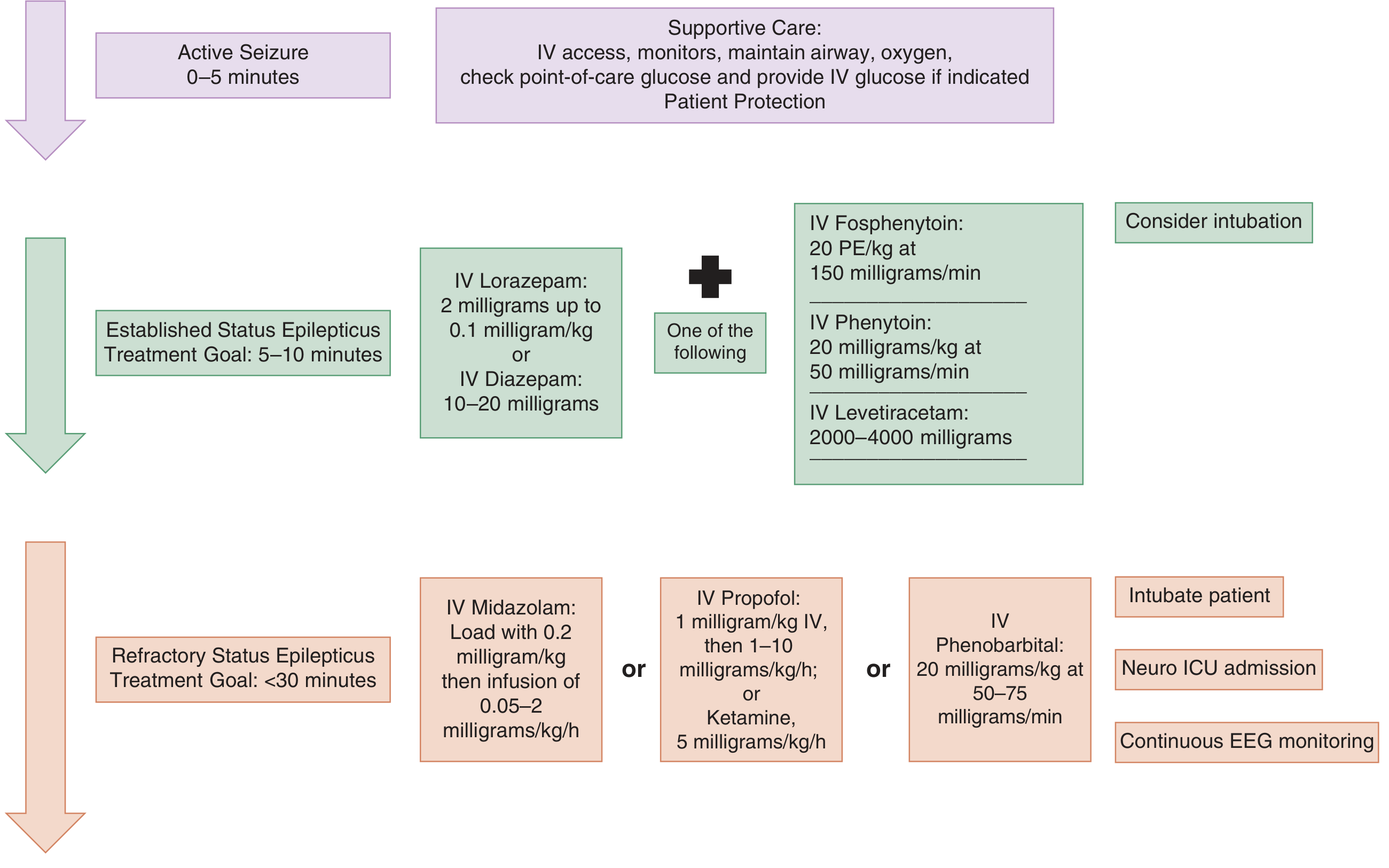
Guidelines for management of active seizures and status epilepticus - Tintinalli's Emergency Medicine
Phase 1: Immediate Stabilization (0-5 minutes)
ABCs first - all steps run simultaneously:
- Position patient to prevent aspiration; immobilize cervical spine if trauma suspected
- Administer oxygen (nasal cannula or face mask); have bag-valve-mask and suction ready
- Use a nasopharyngeal airway if tongue obstruction is present (oral airways risk vomiting on resolution)
- Monitor: HR, BP, RR, SpO2, temperature; treat hyperthermia with antipyretics/cooling blankets
- Elevate head of bed if raised ICP suspected
- Establish large-bore IV access (or IO if IV not obtainable within 1-2 min)
- Check bedside glucose immediately; give IV glucose if hypoglycemia is confirmed or suspected
- Labs: electrolytes, glucose, calcium, magnesium, renal/liver function, CBC, anticonvulsant levels (if applicable), toxicology screen, pregnancy test if appropriate
- Use normal saline - avoid glucose-containing solutions (incompatible with phenytoin)
Phase 2: First-Line Treatment - Benzodiazepines (5-10 minutes)
Benzodiazepines are the drugs of choice - they diffuse rapidly into the CNS and terminate seizures ~70% of the time. Delays >10 minutes in giving benzodiazepines are associated with higher death rates, longer seizure duration, and more complications.
| Drug | Route | Dose |
|---|---|---|
| Lorazepam | IV | 2 mg up to 0.1 mg/kg (max 4 mg) |
| Diazepam | IV | 10-20 mg |
| Midazolam | IM/intranasal/buccal | Preferred if no IV access |
| Diazepam | Rectal | If above unavailable (least preferred) |
- Lorazepam vs. diazepam: Lorazepam is less lipophilic, does not redistribute as rapidly from brain to fat, and has a longer effective duration. Clinical trials have not definitively favored one over the other, but lorazepam is generally preferred IV
- Give a second dose only after 5 minutes of continued seizure following the first dose
- Adverse effects: respiratory depression, hypotension, impaired consciousness - monitor closely
Phase 2b: Concurrent Second-Line Loading (5-10 minutes, alongside benzodiazepines)
At established SE, start a second-line agent at the same time as or immediately after the benzodiazepine. Options are roughly equivalent in efficacy (seizure cessation in ~50% of benzodiazepine-refractory cases):
| Drug | Dose | Key Notes |
|---|---|---|
| Fosphenytoin | 20 PE/kg IV at 150 mg PE/min | Water-soluble; IM-compatible; far less cardiotoxic and sclerosing than phenytoin; converts to phenytoin in plasma |
| Phenytoin | 20 mg/kg IV at ≤50 mg/min | Cardiotoxic, must be in NS only, causes local tissue injury; monitor ECG |
| Levetiracetam | 2000-4000 mg IV | Favorable safety profile; may have fewer adverse events than phenytoin (one RCT); no hepatic/platelet contraindications |
| Valproic acid | 40 mg/kg IV (max 3000 mg) | Contraindicated in liver disease, thrombocytopenia, suspected metabolic disease |
| Lacosamide | IV loading | Well tolerated but requires ECG monitoring (cardiac conduction effects) |
| Phenobarbital | 20 mg/kg IV at 50-75 mg/min | Highly effective but causes prolonged sedation, respiratory depression, hypotension |
If the first second-line agent fails, try a second second-line agent before escalating to anesthesia.
Phase 3: Refractory Status Epilepticus (<30 minutes)
Defined as seizures continuing or recurring ≥30 minutes despite first- and second-line treatment. Requires:
- Intubation (use a short-acting paralytic such as succinylcholine to avoid masking seizure activity)
- Continuous EEG monitoring (mandatory after paralytic use; also for NCSE)
- Neuro ICU admission
- Anesthetic-dose agents:
| Drug | Dose |
|---|---|
| Midazolam infusion | Load 0.2 mg/kg IV, then 0.05-2 mg/kg/h |
| Propofol infusion | 1 mg/kg IV, then 1-10 mg/kg/h |
| Ketamine infusion | 5 mg/kg/h (also useful if intubating a seizing patient - has antiepileptic activity) |
| Pentobarbital / Thiopental | Anesthetic burst-suppression dosing |
| Phenobarbital IV | 20 mg/kg at 50-75 mg/min |
When intubating a seizing patient, select a sedative with antiepileptic properties (propofol or ketamine) rather than a purely sedating agent.
Pathophysiology of Prolonged Seizures
Understanding why treatment becomes harder over time:
- After 5 min: GABA-A receptors are internalized (downregulated) - explaining reduced benzodiazepine effect
- Simultaneously, NMDA (glutamate) receptors are upregulated - excitatory drive increases
- Blood-brain barrier breaks down, allowing excitatory molecules (K+, albumin) to enter CNS
- After 20 min: systemic complications develop - hypotension, hypoxia, metabolic acidosis, hyperthermia, hypoglycemia, cardiac dysrhythmias, pulmonary edema
Common Causes to Identify and Treat
- Subtherapeutic antiepileptic drug levels (in known epileptics)
- Acute stroke (ischemic or hemorrhagic)
- Anoxia/hypoxia
- CNS infection (meningitis, encephalitis)
- Traumatic brain injury
- Metabolic: hyponatremia, hypoglycemia, hypocalcemia, hypomagnesemia
- Drug toxicity or alcohol/drug withdrawal
Special Situations
Post-cardiac arrest: Continuous EEG monitoring recommended. Do not use prophylactic anticonvulsants. If seizures occur, lorazepam 0.1 mg/kg followed by a second-line agent (levetiracetam, valproic acid, or fosphenytoin - all equally effective).
Intracerebral hemorrhage: Prophylactic anticonvulsants are NOT recommended (associated with worse outcomes).
TBI: If seizure prophylaxis is used, prefer levetiracetam 500 mg BID for 7 days over phenytoin (phenytoin associated with worse neurocognitive outcomes).
Nonconvulsive SE: Same medication hierarchy as convulsive SE, but less urgency allows slower, more cautious dosing. EEG is essential for diagnosis and monitoring.
Key Evidence Update (2024-2025)
Recent systematic reviews support the current stepwise approach:
- Vignatelli et al. (2024), Epilepsia - Systematic review of adult SE management guidelines (PMID 38606469)
- Chiriboga et al. (2024), Epilepsia - Ketamine meta-analysis in pediatric SE supports its use in refractory cases (PMID 38881333)
Sources: Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Katzung's Basic and Clinical Pharmacology 16e; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.