Trachea notes
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the content needed. Let me now compile comprehensive trachea notes.
The Trachea - Comprehensive Notes
Overview
The trachea is a fibrocartilaginous air tube that serves as the primary conduit for ventilation between the larynx and the bronchi. It also warms and humidifies inspired air and clears secretions via mucociliary transport.
Gross Anatomy
Dimensions
- Length: 10-12 cm (average adult male: 11.8 cm, range 10-13 cm)
- External diameter: 2.3 cm (AP) x 1.8 cm (transverse) in males; 2.0 cm x 1.4 cm in females
- Paediatric: 3 mm diameter at birth
- Wall thickness: approximately 3 mm
- Shape in cross-section: D-shaped (ovoid)
Extent and Position
- Begins: Lower border of the cricoid cartilage (vertebral level C6)
- Ends: Bifurcation at the carina (level T4/T5 posteriorly, manubrium anteriorly)
- Lies anterior to the esophagus and passes slightly posteriorly from neck to mediastinum
- Mobile: moves upward during swallowing, down and forward on inspiration
Relations
Anterior (cervical)
- Skin, superficial and deep cervical fascia
- Sternohyoid and sternothyroid muscles
- Thyroid isthmus (overlies 2nd-4th tracheal cartilages)
- Inferior thyroid veins
Anterior (mediastinal)
- Left brachiocephalic vein and artery
- Arch of the aorta (crosses left side)
- Left common carotid artery
- Deep cardiac plexus
- Pre-tracheal lymph nodes
- Innominate (brachiocephalic) artery crosses obliquely anterior at ~3rd ring/sternal notch level - important surgical landmark for tracheostomy
Lateral
- Lobes of the thyroid gland
- Carotid sheath and contents
- Para-tracheal lymph nodes
Posterolateral
- Recurrent laryngeal nerves in the tracheo-oesophageal groove (bilaterally)
Posterior
- Esophagus (directly posterior throughout)
Note in infants: The brachiocephalic vein may lie above the suprasternal notch, placing it at risk during tracheal surgery.
Cartilages
- 18-22 C-shaped (incomplete) rings of hyaline cartilage
- ~2 rings per cm; each ring ~4 mm in height
- Maintain patency against the negative pressure of inspiration and prevent collapse during expiration
- The first cartilage is broader and may fuse with the cricoid (or be separated by the cricotracheal ligament)
- The last ring above the carina is thick and broad, forming a bridge between the two main bronchi; its inferior border curves downward to form the carina
- Cartilage rings can become calcified with age (may even undergo ossification with marrow spaces visible on histology)
- Two or more rings may fuse or bifurcate
Posterior Wall - Trachealis Muscle & Fibrous Membrane
- The open posterior ends of the C-shaped rings face the esophagus
- These free ends are bridged by:
- Trachealis muscle - smooth muscle with transverse and longitudinal fibres
- A sheet of fibroelastic tissue continuous with the perichondrium
- The fibrous membrane encircles the rings, is composed of collagen and elastin in crossing orientations - permits expansion and aids elastic recoil
- Trachealis functions:
- Relaxes during swallowing - allows esophagus to bulge into the tracheal space
- Contracts forcefully in cough - narrows the lumen to increase expiratory velocity and dislodge secretions/debris
Histology
Wall Layers (from lumen outward)
| Layer | Composition |
|---|---|
| Mucosa | Ciliated pseudostratified epithelium + elastic fiber-rich lamina propria |
| Submucosa | Slightly denser connective tissue; contains seromucous glands, neurovascular structures, lymphoid patches |
| Cartilaginous layer | C-shaped hyaline cartilage rings covered by perichondrium |
| Adventitia | Connective tissue binding trachea to adjacent structures |
Tracheal Wall Histology (H&E)
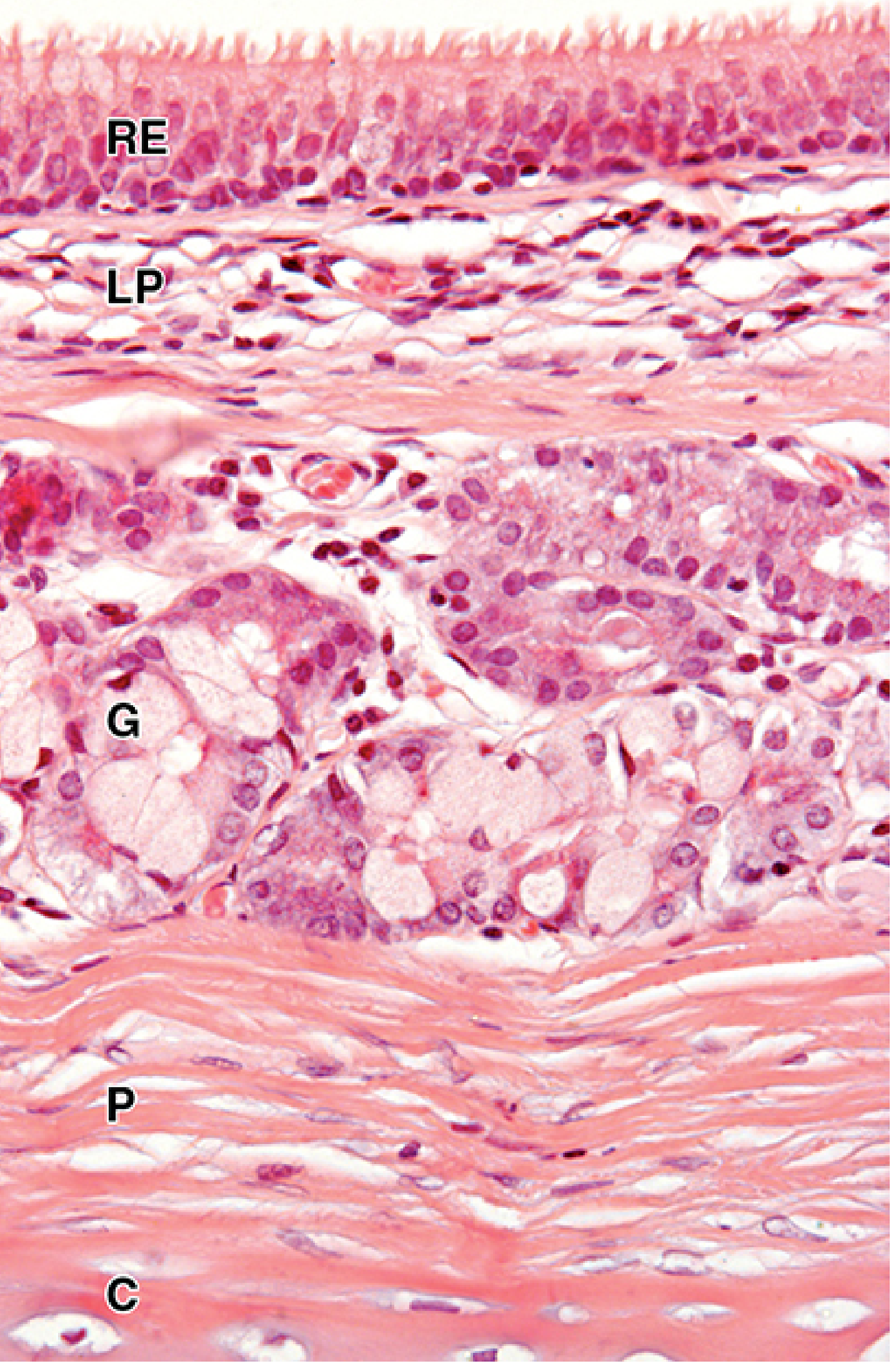
Tracheal wall: respiratory epithelium (RE) overlying lamina propria (LP) with seromucous glands (G), perichondrium (P), and C-shaped hyaline cartilage (C). (Junqueira's Basic Histology, x50 H&E)
Trachea and Esophagus Cross-Section
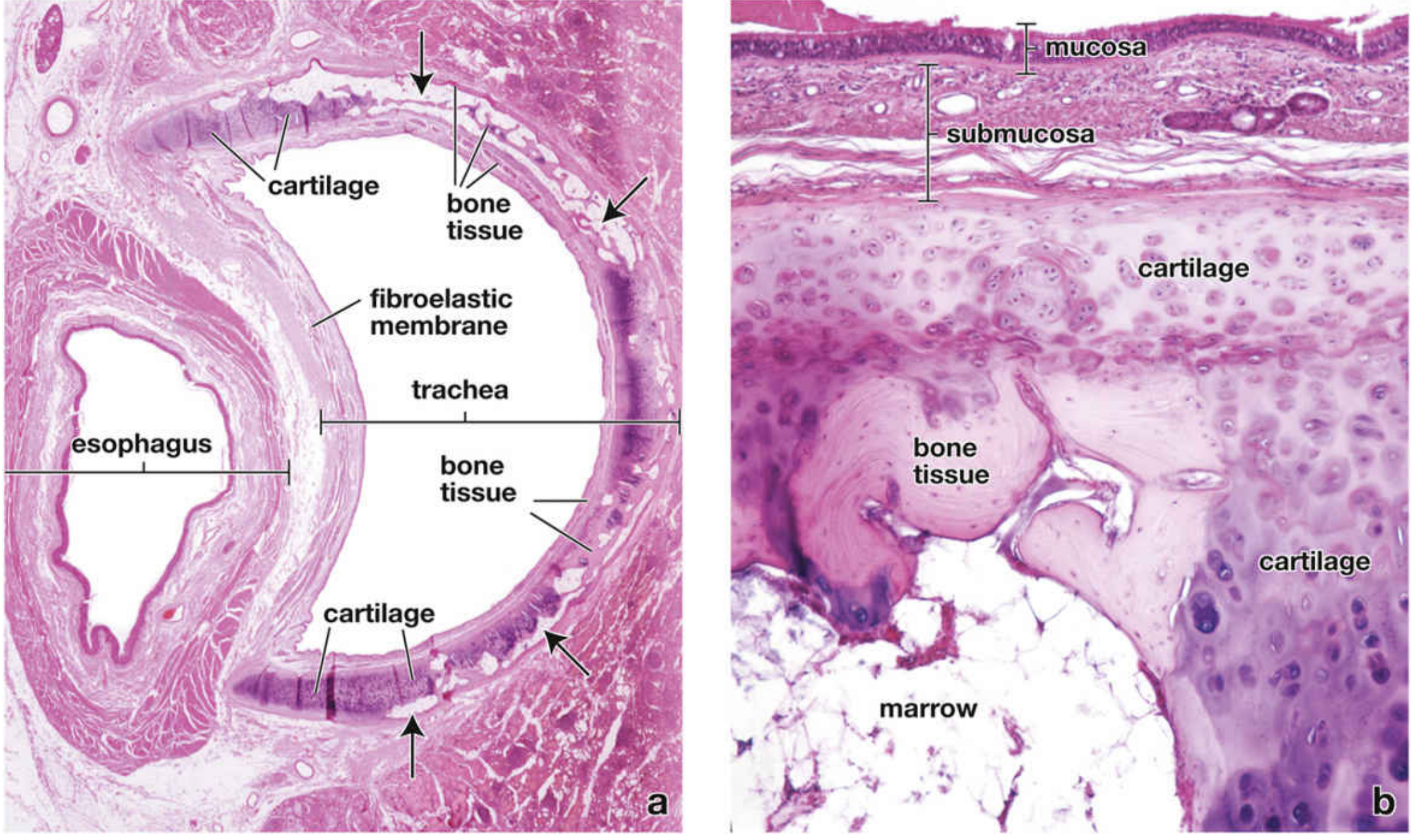
Cross-section at the base of the neck. Left: Low-power view showing the D-shaped tracheal lumen, C-shaped cartilage (with partial ossification in aging), fibroelastic membrane posteriorly, and the esophagus. Right: High-power showing mucosa, submucosa, and cartilage undergoing ossification with marrow spaces. (Histology: A Text and Atlas)
Epithelium (Respiratory / Pseudostratified Ciliated Columnar)
Principal cell types:
- Ciliated columnar cells (most numerous)
- Extend full thickness of epithelium
- Each cell has ~250 cilia
- Basal bodies form a dark line just below the cilia on H&E
- Beat in coordinated waves (mucociliary escalator) - sweeps mucus toward the pharynx
- Goblet (mucous) cells
- Contain mucinogen granules
- Surface has blunt microvilli (stippled on SEM)
- Secrete mucus that traps inhaled particles
- Basal cells
- Confined to the basal layer near the basement membrane
- Stem cell function - regenerate other cell types
- Brush cells - sparse; sensory function
- Small granule cells (DNES/neuroendocrine) - sparse
Glands
- Seromucous glands in the lamina propria and submucosa (mainly mucous with some serous/mixed)
- Secretion is largely autonomically controlled
- Produce a mucin-rich protective barrier that traps debris and microorganisms
Blood Supply
- Blood supply enters lateral walls in a distributed segmental fashion
- Cervical trachea: supplied by inferior thyroid artery (via 3 tracheoesophageal branches, which may pass anterior or posterior to the recurrent laryngeal nerves)
- Segmental arteries branch superiorly and inferiorly over several rings, forming longitudinal anastomoses along the lateral walls
- Anterior branches further anastomose near the midline
- Posterior branches supply the membranous wall (also receives supply from oesophageal arteries)
- Venous drainage: inferior thyroid plexus
- Thoracic trachea / carina / bronchial tree: supplied by bronchial arteries (usually 3: 2 left = direct aortic branches; 1 right = from 3rd right posterior intercostal artery)
- Bronchial veins drain into the azygos vein (right) and accessory hemiazygos (left)
Surgical note: The blood supply enters posterolaterally. During tracheostomy, the inferior thyroidal artery/vein and anterior jugular veins may lie anteriorly between skin and trachea.
Lymphatic Drainage
- Lymphatics arise from a submucosal plexus and connect with a plexus in the outer fibrous membrane
- Drain into pretracheal nodes then para-tracheal nodes (Level VI)
- Para-tracheal nodes drain into internal thoracic and brachiocephalic lymph nodes
- These form bronchomediastinal trunks draining into:
- Right lymphatic duct (right side)
- Thoracic duct (left side)
Nerve Supply
- Autonomic:
- Parasympathetic (vagus) - bronchoconstriction, increased secretion
- Sympathetic - bronchodilation, decreased secretion
- The recurrent laryngeal nerves run in the tracheo-oesophageal groove posterolaterally and are at risk during tracheal and thyroid surgery
Carina and Bifurcation
- Trachea bifurcates at the carina at T4-T5 (posteriorly) / manubrium level (anteriorly)
- Right main bronchus: angle of 25-30° with the carina; length ~5 cm; diameter ~17 mm (males)
- Left main bronchus: angle of 45° with the carina; longer and more horizontal
- Clinical implication: aspirated foreign bodies preferentially enter the right main bronchus due to its wider angle and more vertical course
Physiology Summary
| Function | Mechanism |
|---|---|
| Air conduction | Patency maintained by cartilage rings |
| Warming & humidification | Mucosal vasculature and glands; air reaches 37°C/100% humidity by isothermal saturation point (just distal to carina) |
| Mucociliary clearance | Coordinated ciliary beating moves mucus toward pharynx |
| Cough | Trachealis contraction narrows lumen, increases expiratory air velocity |
| Swallowing | Trachealis relaxation allows esophagus to bulge |
Airflow resistance rule: A 50% reduction in inner diameter increases resistance 16-fold (turbulent flow: 32-fold). At 5-6 mm lumen, only ~30% expiratory flow rate is maintained.
Key Clinical Points
- Tracheostomy landmarks: Thyroid isthmus over 2nd-4th rings; innominate artery crosses ~3rd ring
- Tracheal stenosis: Post-intubation (cuff pressure >20 cmH2O exceeds capillary perfusion pressure); post-tracheostomy (A-shaped scar); "sand-glass" stenosis from cuff injury
- Recurrent laryngeal nerve runs in the tracheo-oesophageal groove - at risk in thyroid/tracheal surgery
- Foreign body aspiration - right bronchus more commonly affected
- Age changes: Cartilage rings undergo progressive calcification and may ossify (marrow spaces visible)
Sources: Gray's Anatomy for Students | Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Junqueira's Basic Histology (17e) | Histology: A Text and Atlas | Current Surgical Therapy (14e) | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.