Truss
Searching the Web
truss structure types engineering overview
Here is a solid overview of trusses in structural engineering:
What is a Truss?
A truss is an assembly of straight members (bars or beams) connected at joints called nodes. The key defining feature is that all joints are treated as pin (revolute) connections, meaning they can rotate freely. This makes every member a two-force member - it carries only axial force: either tension (pull) or compression (push). No bending occurs in the members.
Because all triangles are inherently rigid, a truss is built from triangulated arrangements.
Key Assumptions (Ideal Truss)
- All joints are frictionless pins
- Loads are applied only at joints
- Members are straight and weightless
- Members carry axial forces only (no shear, no bending)
Common Types
| Type | Description | Typical Use |
|---|---|---|
| Pratt | Vertical members in compression, diagonals in tension | Bridges, roofs |
| Warren | Diagonal members alternate in tension/compression, no verticals | Bridges |
| Howe | Verticals in tension, diagonals in compression | Older timber bridges |
| Fink | Fan-like arrangement from a central peak | Roof trusses |
| K-Truss | K-shaped panels, reduces member lengths | Large-span bridges |
| Vierendeel | No diagonals - NOT a true truss (has bending) | Architectural frames |
| Bowstring | Curved top chord | Long-span roofs |
Analysis Methods
- Method of Joints - Resolve forces at each joint using equilibrium (ΣFx = 0, ΣFy = 0)
- Method of Sections - Cut through the truss and apply equilibrium to an isolated portion; useful when only a few member forces are needed
- Graphical Method (Maxwell Diagram) - Older graphical technique
Determinacy
A truss is statically determinate when:
m + r = 2j
Where:
-
m = number of members
-
r = number of reactions
-
j = number of joints
-
If m + r < 2j → mechanism (unstable)
-
If m + r > 2j → statically indeterminate
Applications
- Bridges - Railway bridges (Pratt, Warren), highway spans
- Roof structures - Residential and industrial roof trusses (Fink, Howe)
- Towers - Transmission towers, communication masts
- Space frames - 3D trusses for large roofs (stadiums, airports)
- Cranes and gantries
Materials
- Steel - Most common for large structures (high strength-to-weight ratio)
- Timber - Traditional roof trusses
- Aluminum - Lightweight applications (aircraft, temporary structures)
- Reinforced concrete - Rare, but used in some roof systems
Is there a specific aspect you'd like to go deeper on - analysis, a particular truss type, design, or something else?
Truss in hernia
Reading File
Finding Sources
Searching the Web
truss hernia surgical instrument use complications
Finding Sources
Reading Web Page
https://drkirankj.com/what-is-a-hernia-truss-does-it-really-…
Reading File
Reading File
Reading File
Excellent textbook content retrieved. I now have comprehensive information to give a thorough answer.
Truss in Hernia
A hernia truss (also called a hernia belt) is a mechanical supportive device consisting of a belt with a firm pad that is applied over the hernia site - specifically over the hernial defect - after the hernia has been manually or spontaneously reduced back into the abdominal cavity.
Historical Background
The hernia truss is one of the oldest interventions in surgery. In the 1700s, Ambrose Paré first recommended the use of a hernia truss. It was widely used for centuries before the era of modern surgical repair.
- Fischer's Mastery of Surgery, 8th ed.
How It Works
The mechanism is straightforward:
- The hernia contents (bowel/omentum) are first reduced (pushed back into the abdomen)
- The truss is then strapped on so the pad presses firmly over the hernial defect (the hole in the abdominal wall)
- This creates a mechanical barrier that prevents the contents from re-protruding when the patient coughs, strains, or increases intra-abdominal pressure
Types of Hernia for Which It Is Used
Primarily used for inguinal hernias (both direct and indirect). Occasionally used for umbilical hernias. Applied after groin reduction for symptom relief.
Current Clinical Indications (Limited)
The truss is now rarely recommended. Specific situations where it may still be considered:
| Indication | Notes |
|---|---|
| Temporary relief before planned surgery | Bridge while awaiting elective repair |
| High surgical risk patients | Elderly, medically unfit who cannot undergo anaesthesia |
| Patient refusal of surgery | Temporary symptom control |
| Post-reduction support | After closed reduction in emergency setting |
"A truss should be used only temporarily to prevent recurrent protrusion before surgery can be arranged."
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
"A truss can be used to control a hernia but nowadays few surgeons recommend this approach."
- Bailey and Love's Short Practice of Surgery, 28th ed.
Complications and Drawbacks of Prolonged Truss Use
This is clinically important - trusses can cause significant harm:
| Complication | Mechanism |
|---|---|
| Skin changes | Discoloration, brown pigmentation (haemosiderin deposition), wrinkled atrophic skin with prolonged use |
| Atrophy of spermatic cord | Pressure from truss over time |
| Fibrosis of tissues | Makes subsequent surgical repair more difficult |
| Hernia enlargement | Truss does not prevent gradual enlargement of defect |
| Risk of incarceration/strangulation | If worn with hernia unreduced - can trap bowel and cut off blood supply |
| Skin irritation and pressure sores | Especially with prolonged/incorrect use |
| Atrophy of subcutaneous tissue | Wrinkled overlying skin |
"With prolonged usage, atrophy of the spermatic cord has been reported and eventual surgical repair is made more difficult due to fibrosis of the tissues."
- Mulholland and Greenfield's Surgery, 7th ed.
"If the patient is using a truss for a long time, discoloration and streaks of brown pigmentation due to deposition of haemosiderin may be seen. The subcutaneous tissue may be atrophied, so the skin may be wrinkled."
- S Das: A Manual on Clinical Surgery, 13th ed.
Key Rule Before Applying a Truss
The hernia MUST be fully reduced before applying the truss. Applying a truss over an unreduced hernia is dangerous - it can compress the hernial neck, leading to incarceration and strangulation (a surgical emergency with compromised blood supply to the bowel).
Why Surgery is Preferred Over a Truss
- Truss does not cure the hernia - the fascial defect remains
- Hernia tends to continue enlarging despite truss use
- Up to 70% crossover to surgery within 10 years even in watchful-waiting patients
- Modern hernia repair has a recurrence rate of <2% and is safe as a day-case procedure
- Insufficient evidence that trusses are as effective as surgery for symptom control
Summary
| Feature | Truss |
|---|---|
| Curative? | No |
| Prevents enlargement? | No |
| Prevents strangulation? | No |
| Current role | Temporary/palliative in poor surgical candidates |
| Preferred treatment | Surgical repair (open or laparoscopic) |
The truss remains a historical device that has been largely replaced by safe, effective surgical repair. Its use today is limited to very specific situations and should always be under surgical guidance.
Pectineus facia and its surrounding anatomy
Reading File
Finding Sources
Finding Sources
Searching the Web
pectineal fascia anatomy surrounding structures femoral canal hernia
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive textbook content and anatomy diagrams. Here is a full, well-sourced answer.
Pectineal Fascia and Its Surrounding Anatomy
The pectineal fascia (also called the fascia of the pectineus) is the fascial covering of the pectineus muscle on the floor of the femoral triangle. It is one of the most surgically relevant fascial layers in the groin, forming a key boundary of the femoral canal and the femoral ring.
1. The Pectineus Muscle - Foundation
Before understanding the fascia, understand the muscle it covers:
| Feature | Detail |
|---|---|
| Origin | Superior ramus of the pubis (pectineal line of pubis) |
| Insertion | Pectineal line of the femur (a bony ridge below the lesser trochanter) |
| Action | Adducts and flexes the hip joint |
| Innervation | Femoral nerve (L2-L4); also receives a branch from the obturator nerve (dual innervation) |
| Position | Forms the medial floor of the femoral triangle |
"Pectineus spans between the superior ramus of pubis and pectineal line of the femur. It adducts and flexes hip joint."
- Fischer's Mastery of Surgery, 8th ed.
2. The Pectineal (Cooper's) Ligament - Key Derivative
The tendon of the pectineus muscle inserts into the pectineal line via a dense condensation called the pectineal ligament, which is synonymous with Cooper's ligament.
"The pectineus muscle covers the floor of the vascular gap and inserts into the pectineal line, a ridge of bone, via the pectineal or Cooper's ligament."
- Sabiston Textbook of Surgery
"Cooper's (pectineal) ligament is the lateral portion of the lacunar ligament that is fused to the periosteum of the pubic tubercle."
- Schwartz's Principles of Surgery, 11th ed.

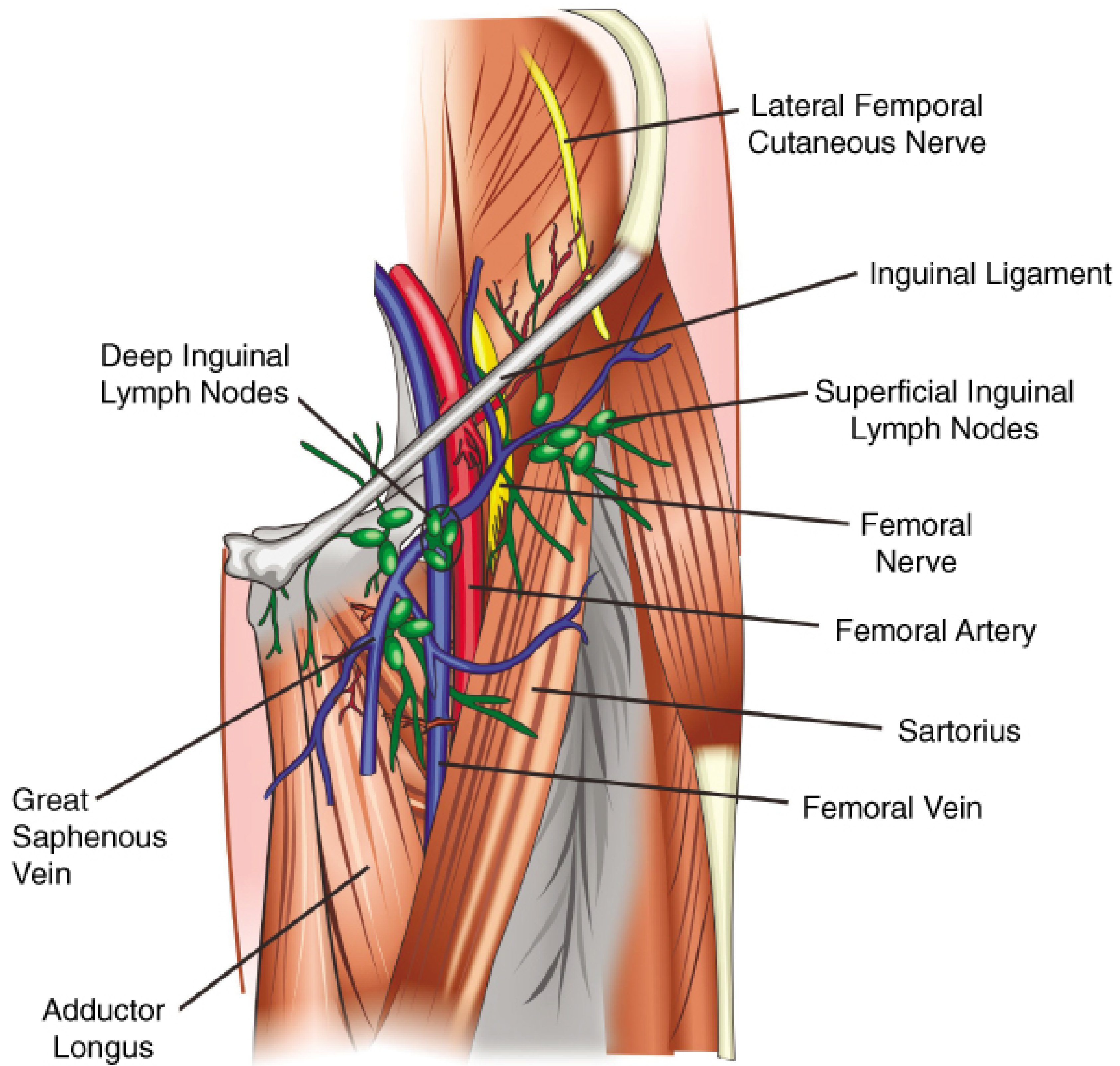
3. The Femoral Triangle - Key Regional Structure
The pectineal fascia forms part of the floor of the femoral triangle:
| Boundary | Structure |
|---|---|
| Superior | Inguinal ligament (Poupart's ligament) |
| Lateral | Sartorius muscle |
| Medial | Adductor longus muscle |
| Floor (medial) | Fascia of pectineus muscle |
| Floor (lateral) | Iliopsoas muscle (covered by iliopsoas fascia) |
| Roof | Skin + subcutaneous tissue + fascia lata |
The neurovascular contents of the femoral triangle from lateral to medial are summarized by the mnemonic NAVEL:
- N - Femoral Nerve
- A - Femoral Artery
- V - Femoral Vein
- E - Empty space (femoral canal)
- L - Lymphatics
4. The Femoral Canal and Femoral Ring - Critical Relations
The femoral canal is the most medial compartment of the femoral sheath, medial to the femoral vein. The femoral ring is its proximal (abdominal) opening.
Boundaries of the femoral ring:
| Wall | Structure |
|---|---|
| Anterior | Inguinal ligament (and iliopubic tract) |
| Posterior | Pectineus muscle and its fascia (pectineal fascia) |
| Medial | Lacunar ligament (ligament of Gimbernat) |
| Lateral | Femoral vein |
"The femoral ring is bounded anteriorly by the inguinal ligament, posteriorly by the pectineus muscle and its fascia, medially by the lacunar ligament, and laterally by the femoral vein."
- Gray's Anatomy for Students
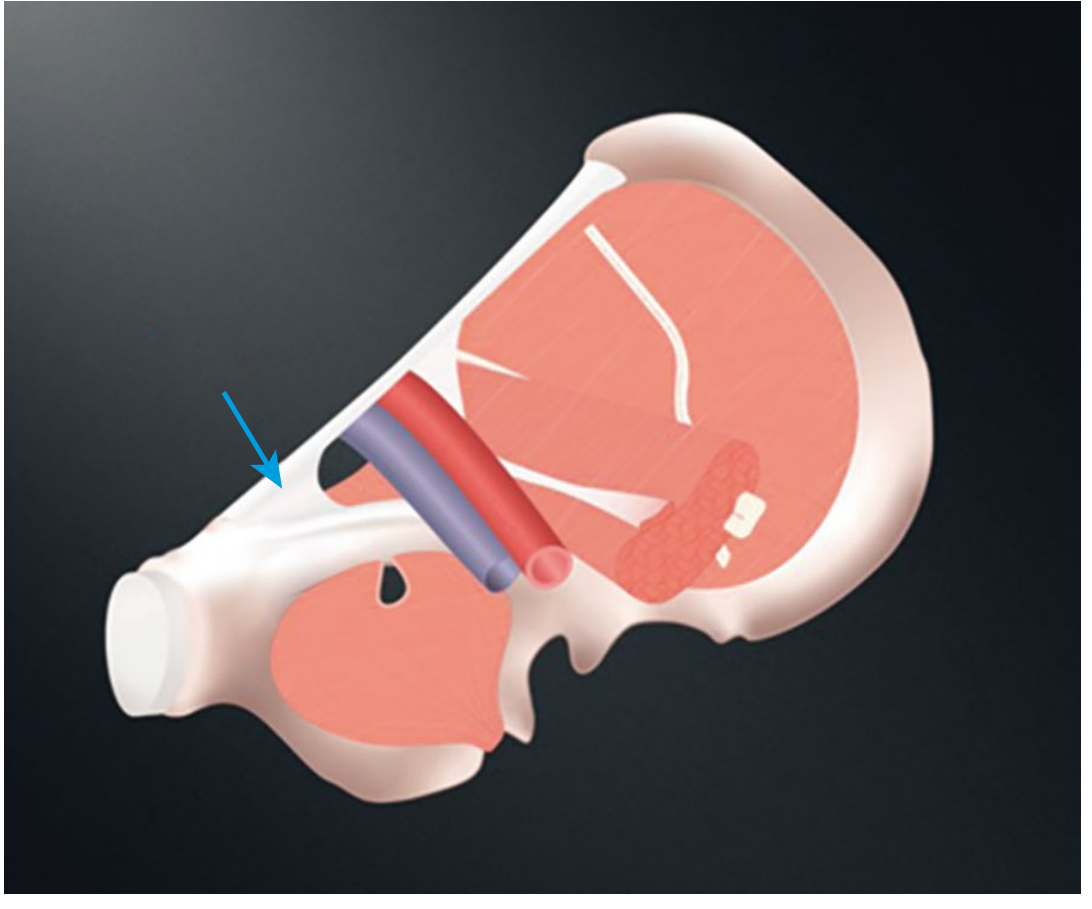
5. The Iliopectineal Arch - Dividing the Gap Below the Inguinal Ligament
The space below the inguinal ligament is divided into two compartments by the iliopectineal arch (a condensation of the iliopsoas fascia):
| Compartment | Contents |
|---|---|
| Lateral (muscular) | Iliopsoas muscle + femoral nerve + lateral femoral cutaneous nerve |
| Medial (vascular) | Femoral artery, femoral vein, femoral canal (lymphatics) |
"The gap below the inguinal ligament is divided into two spaces by another condensation of the iliopsoas fascia, known as the ilio-pectineal arch. The medial aspect is vascular, and the lateral is muscular."
- Sabiston Textbook of Surgery
The lateral muscular aspect is covered by iliopsoas fascia, which protects the femoral nerve and must be preserved during hernia repair to prevent nerve injury.
6. The Lacunar Ligament - Medial Neighbor
Medial to the pectineal fascia, the lacunar ligament (ligament of Gimbernat) is formed by the triangular fanning of the inguinal ligament as it joins the pubic tubercle. It then extends further medially along the superior pubic ramus as the pectineal (Cooper's) ligament.
"The fibrous band that curves downward from the medial attachment of the inguinal ligament is called the lacunar ligament, which extends further medially as the pectineal ligament (Cooper's ligament) and runs along the superior pubic ramus. This sharp-edged ligament defines the medial boundary of the vascular compartment (femoral ring) and may entrap the hernial sac in patients with a femoral hernia."
- Thieme Atlas of Anatomy: General Anatomy and Musculoskeletal System
7. The Iliopectineal Bursa - Clinically Important
The iliopectineal bursa lies deep to the iliopsoas where it passes over the hip joint capsule, just posterior to the pectineal area. It is the largest bursa in the hip region and communicates with the hip joint cavity in ~15% of individuals - meaning hip joint inflammation can directly cause iliopectineal bursitis, presenting as a groin mass that may be mistaken for a neoplasm on MRI.
8. Summary - Structures Surrounding the Pectineal Fascia
Inguinal Ligament (superior)
|
Femoral Artery | Femoral Vein | [Femoral Canal]
|
PECTINEAL FASCIA (posterior floor of femoral ring)
|
Pectineus Muscle
|
Pectineal Line of Femur
|
Cooper's (Pectineal) Ligament
Medial: Lacunar ligament → Cooper's ligament
Lateral: Iliopsoas fascia (covering iliopsoas + femoral nerve)
Superficial roof: Fascia lata → Cribriform fascia → Skin
Surgical Relevance
- The pectineal fascia forms the posterior wall of the femoral ring - so femoral hernias lie directly anterior to it
- Cooper's ligament repair (McVay repair) sutures the inguinal structures to the pectineal ligament, using this structure as a firm anchor
- The aberrant obturator artery (enlarged pubic branch of inferior epigastric) may course along the lacunar ligament - if cut during femoral hernia repair, it causes severe bleeding (the "corona mortis" variant)
- The iliopsoas fascia over the lateral compartment must be kept intact to protect the femoral nerve during laparoscopic repair
Sources: Gray's Anatomy for Students; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11th ed.; Fischer's Mastery of Surgery, 8th ed.; Thieme Atlas of Anatomy
Henrys procedure
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and surgical illustrations. Here is the full answer.
Henry's Procedure (Anterior/Volar Approach to the Radius)
Henry's approach (also called the anterior or volar approach to the radius) is the standard surgical approach to the radial shaft, described by A.K. Henry. It is the most widely used approach for operative fixation of radial shaft fractures and provides access to the entire length of the radius from the bicipital tuberosity down to the distal articular surface.
"The length of the radius can be approached from either the volar-based approach described by Henry or by a dorsal-based approach..."
- Rockwood and Green's Fractures in Adults, 10th ed.
Indications
- Fractures of the radial shaft (diaphysis) - particularly the distal 4/5ths
- Both-bone forearm fractures (radius + ulna)
- Radial osteotomy / corrective osteotomy for malunion
- Removal of hardware / implants along the radius
- Tumour excision involving the radial shaft
- Volar plating of distal radius fractures (modified Henry approach)
"The volar approach of Henry is used in nearly all fractures of the radius."
- Campbell's Operative Orthopaedics, 15th ed. 2026
Patient Positioning
- Patient supine
- Arm extended on a hand table, forearm supinated
- Tourniquet applied to the upper arm
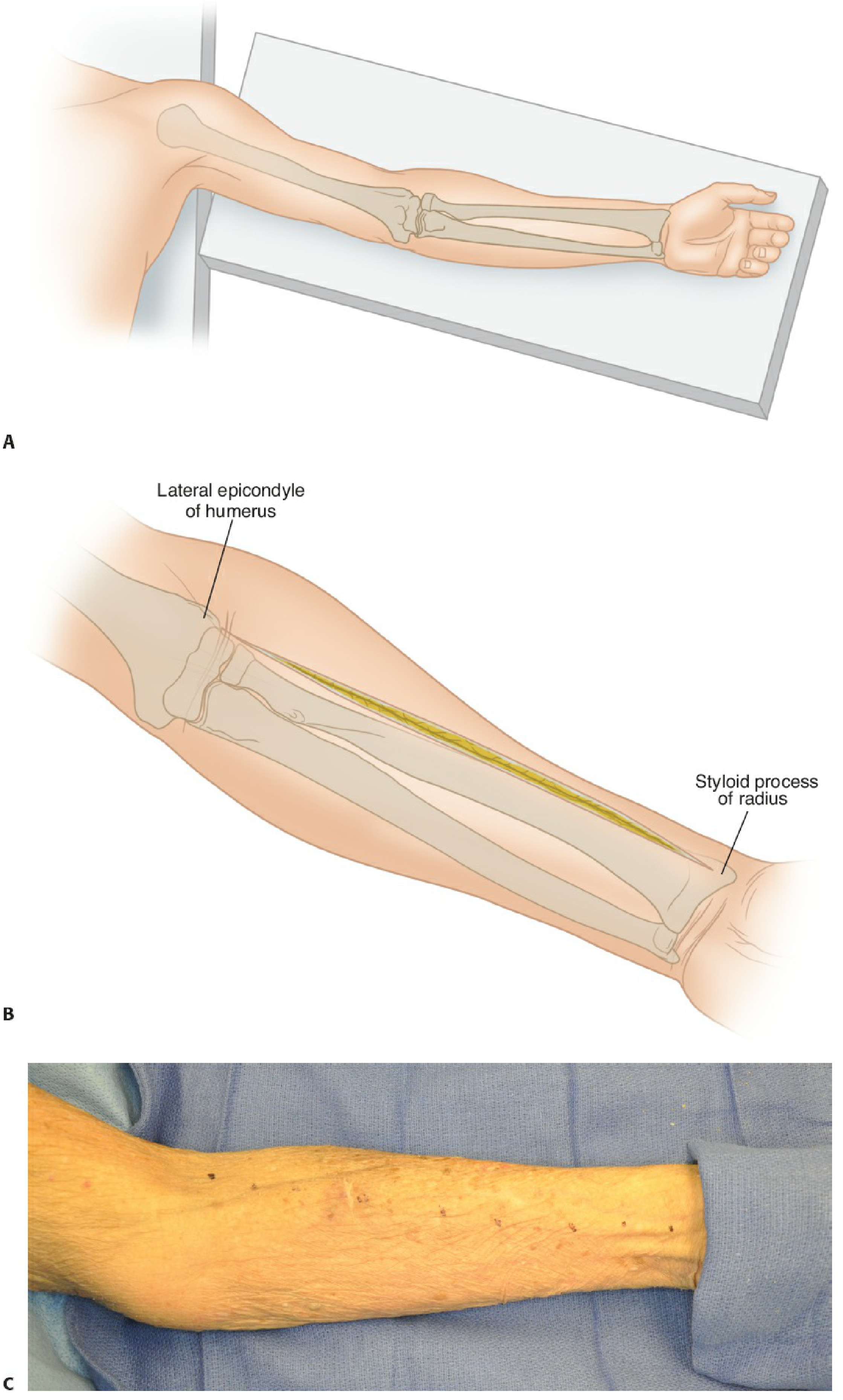
Skin Incision
A longitudinal incision is drawn along a line connecting:
- Proximally: lateral aspect of the biceps tendon (at the antecubital fossa)
- Distally: radial styloid
This places the incision along the ulnar border of the brachioradialis muscle. The length of incision is adjusted depending on the fracture level.
The Internervous Plane (KEY Concept)
Henry's approach exploits a true internervous interval, making it safe because neither nerve is put at risk by the dissection plane itself:
| Level | Lateral muscle | Medial muscle | Nerve on lateral side | Nerve on medial side |
|---|---|---|---|---|
| Proximal/Middle third | Brachioradialis | Pronator teres (PT) | Radial nerve | Median nerve |
| Distal third | Brachioradialis | Flexor carpi radialis (FCR) | Radial nerve | Median nerve |
"The approach proceeds through a true internervous interval since the brachioradialis is innervated by the radial nerve and both PT and FCR are innervated by the median nerve."
- Rockwood and Green's Fractures in Adults, 10th ed.
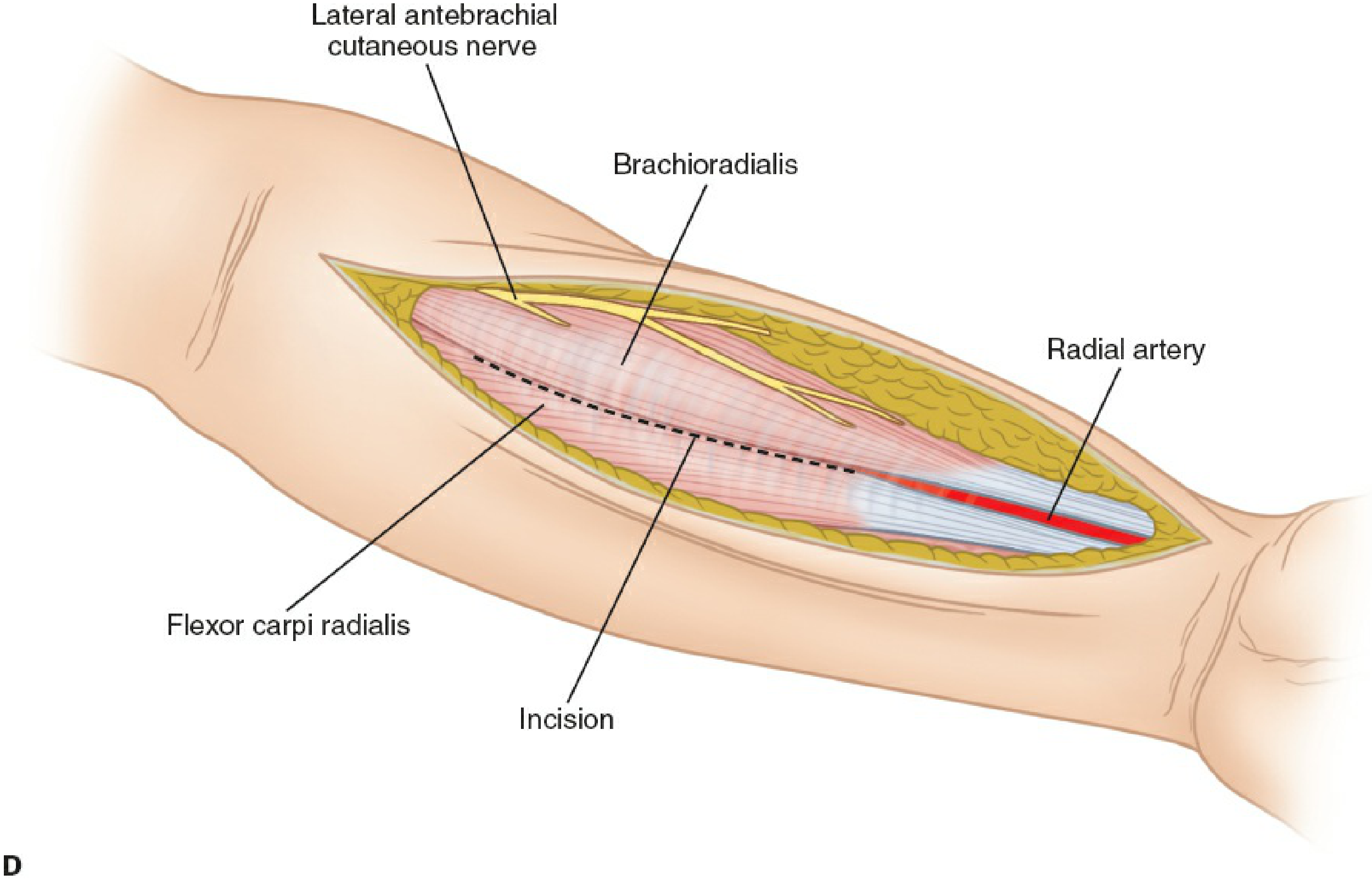
Step-by-Step Surgical Technique
1. Superficial Dissection
- Incise skin and fascia
- Identify the interval between brachioradialis (lateral) and PT/FCR (medial)
- The radial artery runs under brachioradialis in the proximal/middle third, then surfaces between FCR and brachioradialis distally
- To retract the radial artery medially: ligate the vascular branches (leash of Henry) - small branches from the radial artery to the brachioradialis
- The superficial branch of the radial nerve (SBRN) runs under brachioradialis and must be retracted laterally with the brachioradialis
2. Deep Dissection - Varies by Fracture Level
| Level | Forearm Position | Deep Structure Released |
|---|---|---|
| Proximal third (supinator) | Full supination | Supinator stripped subperiosteally off radius; PIN displaced posteriorly by supination |
| Middle third (pronator teres) | Pronation | PT insertion incised/elevated subperiosteally |
| Distal third | Supination | FPL retracted ulnarly; pronator quadratus (PQ) released from radial origin and reflected |
"From distal to proximal, the radial shaft is covered by pronator quadratus, flexor digitorum superficialis, pronator teres, and supinator. Note that to gain proximal access to the radius, the recurrent radial artery has to be ligated."
- Rockwood and Green's Fractures in Adults
The "Leash of Henry"
A cluster of small radial artery branches that tether the brachioradialis to the radial artery in the proximal forearm. These must be identified, ligated, and divided to allow medial retraction of the radial artery and ulnar retraction of brachioradialis, opening the deep dissection window.
"Isolate and ligate the leash of Henry (radial artery branches) proximally and strip the supinator from its insertion subperiosteally."
- Miller's Review of Orthopaedics, 9th ed.
Critical Structures at Risk
| Structure | Risk | Protection |
|---|---|---|
| Posterior interosseous nerve (PIN) | During proximal exposure of radius through supinator | Fully supinate forearm - moves PIN posteriorly/laterally away from dissection |
| Superficial branch of radial nerve (SBRN) | Throughout approach, runs under brachioradialis | Retract laterally with brachioradialis |
| Radial artery | Proximally (medial to biceps tendon) and distally (with brachioradialis retraction) | Identify and protect at all levels; ligate leash of Henry carefully |
| Recurrent radial artery | Proximal exposure near radial neck | Ligate to allow proximal retraction |
| Median nerve | Retraction of medial column | Avoid aggressive retraction on PT/FCR |
"Retraction around the radial neck should be avoided to prevent injury to the PIN."
- Rockwood and Green's Fractures, 10th ed.
Comparison: Henry vs. Thompson Approach
| Feature | Henry (Anterior/Volar) | Thompson (Posterior) |
|---|---|---|
| Internervous plane | Brachioradialis (radial) / PT or FCR (median) | ECRB (radial/PIN) / EDC or EPL (PIN) |
| Best for | Distal 4/5 of radius, volar plate fixation | Proximal radius, radial head/neck |
| Main nerve at risk | PIN, SBRN, radial artery | PIN |
| Access | Full radial shaft volar surface | Dorsolateral radius |
Modified Henry Approach
A modified Henry approach extends the same principle to the elbow/proximal radius, dissecting between the biceps tendon and pronator teres with lacertus fibrosus division, exposing the radial head, capitellum, and proximal radial shaft. The radial nerve (and its branches) must be meticulously identified at this level.
"Modified Henry volar approach to elbow joint: Fascia incised to expose brachioradialis laterally and biceps/brachialis medially. Lacertus fibrosus divided. Dissection deepened between biceps tendon and pronator teres medially and brachioradialis laterally."
- Campbell's Operative Orthopaedics, 15th ed. 2026
Summary
| Feature | Detail |
|---|---|
| Approach | Anterior/volar forearm |
| Internervous plane | Brachioradialis (radial n.) / PT or FCR (median n.) |
| Exposure | Full radial shaft, especially distal 4/5 |
| Forearm supinated | Proximal exposure (protect PIN) |
| Forearm pronated | Middle exposure (PT release) |
| Key step | Ligate leash of Henry; protect SBRN + PIN |
| Main use | ORIF radius shaft fractures; volar plating distal radius |
Sources: Rockwood and Green's Fractures in Adults, 10th ed. 2025; Campbell's Operative Orthopaedics, 15th ed. 2026; Miller's Review of Orthopaedics, 9th ed.
Henrys procedure in femoral hernia
Finding Sources
Finding Sources
Searching the Web
Henry's operation femoral hernia preperitoneal approach surgical technique
Finding Sources
Finding Sources
Reading Web Page
https://www.intechopen.com/chapters/77514
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Cheatle Henry operation femoral hernia technique midline extraperitoneal approach steps
Finding Sources
Reading Web Page
https://journals.sagepub.com/doi/10.1177/155335069400100203
Finding Sources
Searching the Web
"Henry's operation" femoral hernia "midline" OR "extraperitoneal" steps surgical technique anatomy
Now I have everything I need. Let me compile the comprehensive answer.
Henry's Operation for Femoral Hernia
Henry's operation (fully termed "Operation for femoral hernia by a midline extraperitoneal approach", described by A.K. Henry in 1936 in The Lancet) is a preperitoneal/extraperitoneal approach to femoral hernia repair. It is also known as the Cheatle-Henry operation or the suprapubic extraperitoneal approach, because Cheatle first described transabdominal preperitoneal herniorrhaphy in 1920, and Henry subsequently popularized the midline extraperitoneal variant.
Historical Context
| Surgeon | Year | Contribution |
|---|---|---|
| Cheatle | 1920 | First transabdominal preperitoneal herniorrhaphy |
| A.K. Henry | 1936 | Midline extraperitoneal approach for femoral hernia (Lancet) |
| McEvedy | 1950 | Lateral (paramedian) preperitoneal approach - a modification |
| Nyhus & Condon | 1960s | Popularized preperitoneal repair for all groin hernias |
Classification of Approaches to Femoral Hernia
There are three classical open approaches to femoral hernia repair:
| Approach | Entry | Best Use |
|---|---|---|
| 1. Low (crural / Lockwood) | Below inguinal ligament via femoral/groin incision | Elective, reducible hernia |
| 2. High (inguinal / McVay) | Above inguinal ligament through inguinal canal | Combined inguinal + femoral |
| 3. Preperitoneal (Henry / Cheatle-Henry) | Midline or paramedian extraperitoneal | Emergency - strangulated/incarcerated |
"A third type of femoral hernia repair is the preperitoneal repair. Access to the preperitoneal space is gained through an abdominal incision or laparoscopy. This approach is particularly useful during repair of a strangulated hernia since there is more space to allow for inspection of the bowel."
- Mulholland and Greenfield's Surgery, 7th ed.
Indications for Henry's (Cheatle-Henry) Operation
- Strangulated femoral hernia - primary indication; best approach for bowel viability assessment and resection if needed
- Incarcerated femoral hernia - difficult to reduce from below
- Large femoral hernia sac with voluminous intra-abdominal contents
- Bilateral femoral hernias - single incision can address both sides
- Recurrent femoral hernia (avoids scar tissue from previous anterior repair)
- Suspected aberrant obturator artery (corona mortis) - safer from above
"If the femoral hernia sac is large and filled with voluminous intra-abdominal contents, a preperitoneal repair should be considered... This approach is particularly useful during repair of a strangulated hernia since there is more space to allow for inspection of the bowel to ensure viability."
- Maingot's Abdominal Operations
Surgical Technique - Step by Step
Position
- Patient supine
- Head-down (Trendelenburg) tilt helps displace bowel away from the operative field
Incision
- Vertical midline incision below the umbilicus, extending to the pubic symphysis (or a lower transverse/Pfannenstiel-style incision)
- Alternatively, a paramedian incision lateral to the rectus abdominis
Entry into Preperitoneal Space
- Skin and subcutaneous tissue divided
- Anterior rectus sheath incised
- Rectus abdominis retracted medially (not divided)
- Dissection carried deep to the rectus into the preperitoneal (extraperitoneal) space
- The peritoneum is NOT opened (extraperitoneal dissection) - it is gently swept upward and away
- The space of Retzius (retropubic preperitoneal space) is developed by blunt dissection
Identification and Reduction of Hernia
- The preperitoneal fat is dissected to expose the posterior surface of the inguinal region and the femoral ring
- The femoral hernia sac is identified protruding through the femoral ring (bounded anteriorly by the inguinal ligament, posteriorly by pectineal fascia/Cooper's ligament, medially by lacunar ligament, laterally by femoral vein)
- The sac is drawn upward (reduced from above) into the preperitoneal space
- If strangulated: the sac is opened, bowel viability assessed; ischaemic bowel resected and anastomosed in the preperitoneal space before full reduction
- The neck of the sac is transfixed and ligated; the sac excised
Repair of the Defect
- The femoral canal defect is closed:
- Suture repair: Cooper's (pectineal) ligament is sutured to the inguinal ligament/iliopubic tract - narrows the femoral ring
- Mesh repair: A preperitoneal mesh is placed to cover the entire myopectineal orifice - preferred in modern practice
Wound Closure
- The preperitoneal space is allowed to collapse
- Rectus sheath closed, then skin
Key Anatomical Relationships Encountered
| Structure | Significance During Henry's Operation |
|---|---|
| Space of Retzius | The preperitoneal working space entered via this approach |
| Cooper's (pectineal) ligament | Key suture anchor for defect closure |
| Femoral ring | The defect - accessed from above and behind |
| Femoral vein | Lateral boundary of femoral ring - must not be damaged |
| Lacunar ligament | Medial boundary - sharp edge can constrict strangulated bowel; may need to be divided (risk: aberrant obturator artery) |
| Aberrant obturator artery | Runs along lacunar ligament in ~30% - if cut → massive bleeding ("crown of death / corona mortis") |
| Inferior epigastric vessels | Run lateral to rectus; must be identified and preserved |
Advantages of Henry's Operation
- Provides the widest exposure of the femoral ring from inside
- Allows bowel inspection and resection without a separate laparotomy incision
- Can address bilateral hernias through the same midline incision
- Preperitoneal mesh placement here covers the entire myopectineal orifice - prevents recurrence of both inguinal and femoral hernias
- Avoids operating through scar tissue in recurrent cases
- Safe control of the aberrant obturator artery
Disadvantages / Risks
- More invasive than the low (crural) approach for elective simple hernias
- Risk of peritoneal entry - converts to intraperitoneal operation
- Learning curve for preperitoneal anatomy
- Recurrent femoral hernia if defect not fully covered
Modern Equivalent
The laparoscopic TEP (Total Extraperitoneal) and TAPP (Transabdominal Preperitoneal) repairs are the direct modern descendants of Henry's principle - using the same preperitoneal space with mesh to cover the myopectineal orifice, now done with laparoscopic instruments instead of an open midline incision.
"Cheatle-Henry operation is a safe and secure technique to operate on femoral hernia... With laparoscopic surgery, total extraperitoneal technique is done with a patch to cover the femoral ring."
- Cervantes-Castro et al., Cirugía y Cirujanos 2011 (PMID: 22380991)
Summary
| Feature | Detail |
|---|---|
| Full name | Henry's midline extraperitoneal approach |
| Also called | Cheatle-Henry operation; suprapubic preperitoneal repair |
| Approach | Midline/paramedian subumbilical incision |
| Plane | Preperitoneal (extraperitoneal) - peritoneum not opened |
| Best indication | Strangulated / incarcerated femoral hernia |
| Key anatomy | Space of Retzius, Cooper's ligament, femoral ring, aberrant obturator artery |
| Repair | Sutures to Cooper's ligament OR preperitoneal mesh |
| Modern equivalent | Laparoscopic TEP / TAPP |
This is a shared conversation. Sign in to Orris to start your own chat.