Tell me hyper and hypo natremia and kalemia in detail with proper understanding with photos medicine mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Excellent! I now have all the key content and images. Let me now compile the comprehensive answer with everything gathered.
Electrolyte Disorders: Hypo/Hypernatremia & Hypo/Hyperkalemia
A complete MBBS-level guide based on Goldman-Cecil Medicine, Comprehensive Clinical Nephrology, Tietz Textbook of Laboratory Medicine, Medical Physiology (Boron & Boulpaep), and Ganong's Review.
PART 1: SODIUM (Na+) DISORDERS
Normal Values
- Normal serum Na+: 135-145 mmol/L
- Sodium is the primary determinant of plasma osmolality and ECF volume
- Normal plasma osmolality: 280-295 mOsm/kg
HYPONATREMIA (Na+ < 135 mmol/L)
Definition & Epidemiology
Hyponatremia is the most common electrolyte disorder in hospitalized patients, with incidence as high as 15-30% in acutely and chronically hospitalized patients. A serum Na+ <135 mmol/L is associated with a ~45% relative increase in ICU admission rates.
- Goldman-Cecil Medicine
- Tietz Textbook of Laboratory Medicine, 7th Edition
First Step: Measure Plasma Osmolality
Hyponatremia is NOT always hypo-osmolar. It has THREE osmolar states:
| Type | Plasma Osmolality | Cause |
|---|---|---|
| Hypo-osmolar | Low (<280 mOsm/kg) | True hyponatremia (most common) |
| Iso-osmolar | Normal (280-295) | Pseudohyponatremia (hyperlipidemia, hyperproteinemia) |
| Hyper-osmolar | High (>295) | Hyperglycemia, mannitol, uremia |
Pseudohyponatremia is a lab artifact where excess lipid or protein displaces aqueous plasma volume - the true sodium in water is normal. Direct ion-selective electrodes (ISE) avoid this pitfall.
Diagnostic Algorithm for Hyponatremia
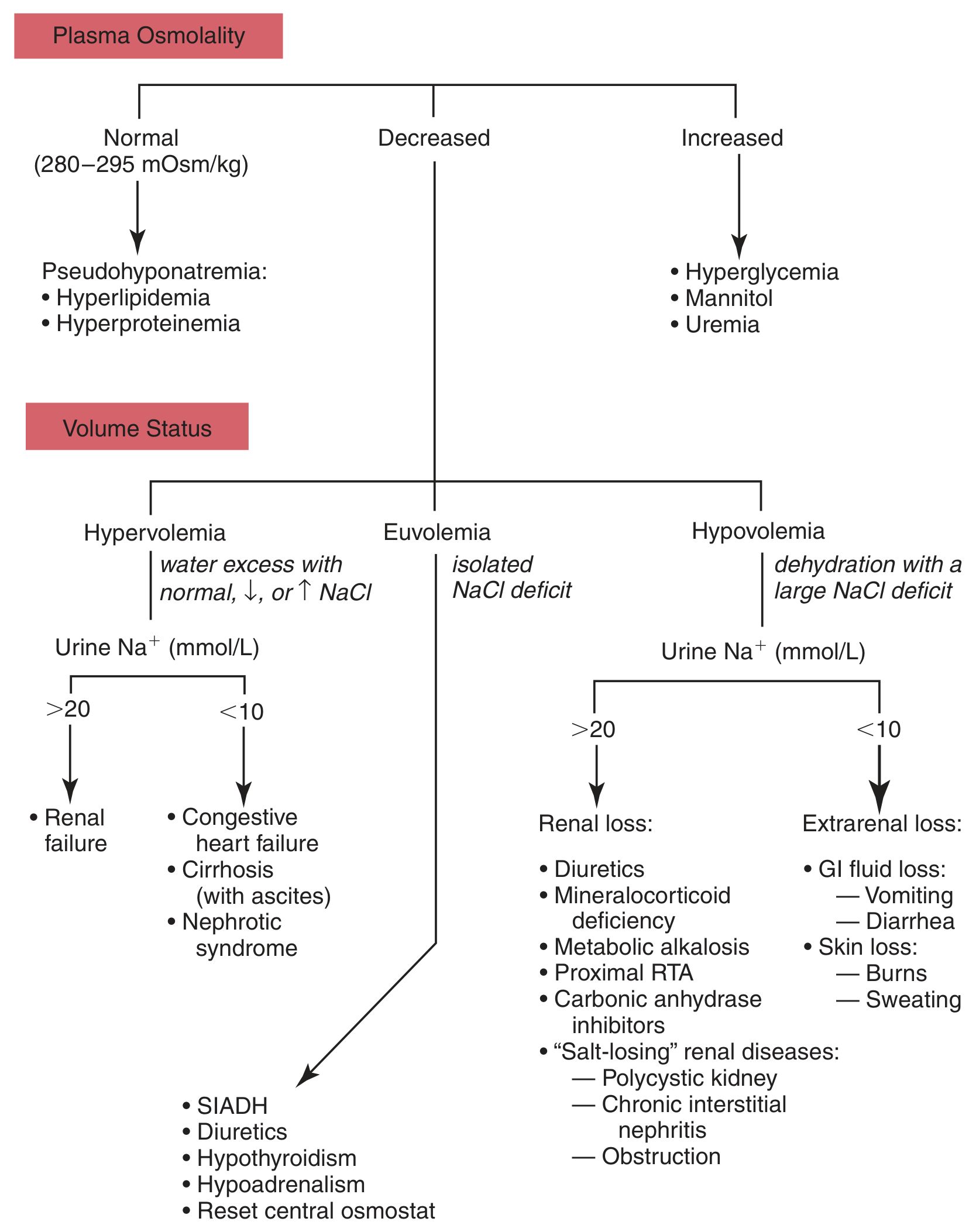
Algorithm for differential diagnosis of hyponatremia based on plasma osmolality and volume status. - Tietz Textbook of Laboratory Medicine, 7th Edition
Hypo-osmolar Hyponatremia: Classify by Volume Status
1. HYPOVOLEMIC Hyponatremia (Urine Na+ is the key)
- Renal losses (Urine Na+ >20 mmol/L): Diuretics, mineralocorticoid deficiency (Addison's), metabolic alkalosis, salt-losing nephropathy (polycystic kidney, chronic interstitial nephritis), renal tubular acidosis
- Extrarenal losses (Urine Na+ <10 mmol/L): Vomiting, diarrhea, burns, sweating
2. HYPERVOLEMIC Hyponatremia
- Urine Na+ >20: Acute/chronic renal failure
- Urine Na+ <10: Congestive heart failure, cirrhosis (with ascites), nephrotic syndrome
- Mechanism: Reduced effective circulating volume activates ADH and RAAS, causing water retention
3. EUVOLEMIC Hyponatremia (most common cause = SIADH)
- SIADH (Syndrome of Inappropriate ADH secretion)
- Hypothyroidism, hypoadrenalism, reset osmostat
- Diuretics
SIADH - Key Points
SIADH is characterized by:
- Hypo-osmolar hyponatremia
- Urine osmolality inappropriately high (>100 mOsm/kg)
- Urine Na+ >20 mmol/L
- No edema, no volume depletion
- Causes: CNS disorders (meningitis, stroke, head trauma), pulmonary disease (TB, pneumonia, SCLC), drugs (SSRIs, carbamazepine, cyclophosphamide, NSAIDs), postoperative state
Clinical Features of Hyponatremia
Symptoms are due to cerebral edema from water moving into CNS cells:
- Na+ 125-135: Nausea, malaise, headache
- Na+ <125: Confusion, lethargy, generalized weakness
- Na+ <120: Severe mental confusion
- Na+ <105: Seizures, coma
The rapidity of onset determines severity - acute hyponatremia causes symptoms at higher Na+ levels (e.g., ~125 mmol/L) than chronic hyponatremia.
Treatment of Hyponatremia
| Type | Treatment |
|---|---|
| Hypovolemic | Isotonic saline (0.9% NaCl) to restore volume |
| Hypervolemic | Fluid restriction + treat underlying cause |
| Euvolemic / SIADH | Fluid restriction; vasopressin receptor antagonists (tolvaptan, conivaptan); hypertonic saline for severe/symptomatic cases |
CRITICAL WARNING - Osmotic Demyelination Syndrome (ODS):
Correction must NOT exceed 8-10 mmol/L in 24 hours (or ~1-2 mmol/L/hour in symptomatic acute cases). Rapid correction causes osmotic demyelination (central pontine myelinolysis) - an irreversible, devastating neurologic injury.
HYPERNATREMIA (Na+ > 145 mmol/L)
Definition
Hypernatremia (plasma Na+ >144-145 mmol/L) always reflects hypertonicity - there is always an increased concentration of osmotically active solutes. It is considerably less common than hyponatremia because even a 1% increase in serum osmolality triggers thirst.
- Goldman-Cecil Medicine
Mortality in critically ill patients with hypernatremia: 40-60%, with prolonged ICU stay.
Why Thirst is the Guardian
In any awake, alert person with a normal thirst mechanism and access to water, hypernatremia should not develop. Most cases occur in:
- Patients with altered mental status
- Infants
- Elderly patients with impaired thirst (hypodipsia)
- Hospitalized patients unable to access fluids
Causes Classified by Volume Status
Diagnostic Algorithm for Hypernatremia
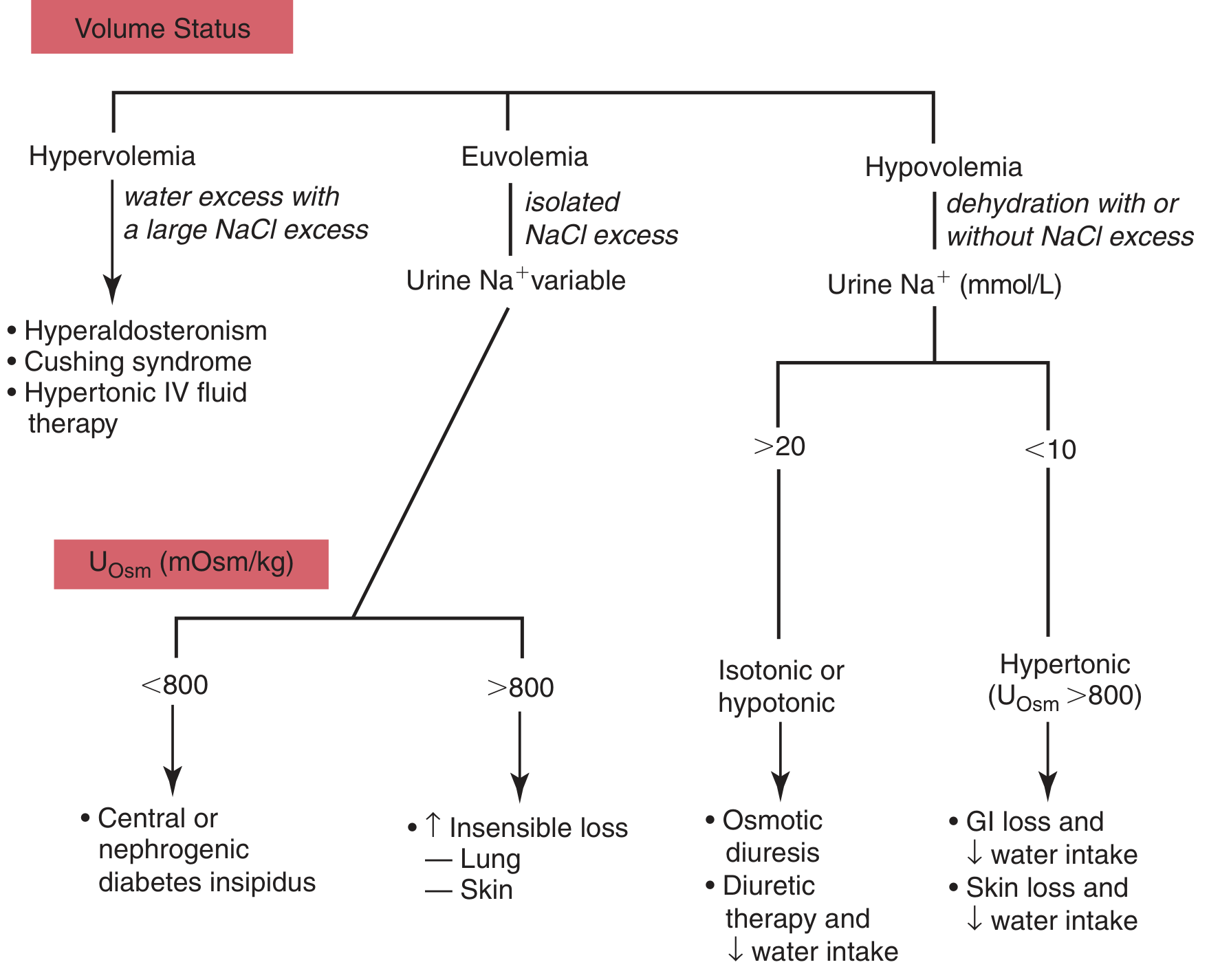
Algorithm for differential diagnosis of hypernatremia based on volume status and urine Na+/osmolality. - Tietz Textbook of Laboratory Medicine, 7th Edition
| Volume Status | Cause |
|---|---|
| Hypovolemic | Extrarenal: diarrhea, burns, sweating (Uosm >800, UNa <20) |
| Euvolemic | Diabetes insipidus (central or nephrogenic) |
| Hypervolemic | Hypertonic saline excess, Cushing syndrome, hyperaldosteronism, hypertonic NaHCO3 |
Diabetes Insipidus (DI) - Key Cause of Hypernatremia
| Central DI | Nephrogenic DI | |
|---|---|---|
| Defect | Failure to release ADH | Failure of kidney to respond to ADH |
| Causes | Hypothalamic/pituitary tumor, head injury, surgery, hemorrhage | Lithium, demeclocycline, V2-receptor mutation, AQP2 mutation |
| Urine osmolality | Very low (100-150 mOsm/kg) | Low |
| Treatment | Desmopressin (synthetic ADH) | Treat cause; low-salt diet; thiazides |
Daily urine output in DI can reach up to 20 liters.
Clinical Features of Hypernatremia
Primary neurologic symptoms due to shrinkage of CNS cells as water leaves cells:
- Tremors, irritability, ataxia
- Confusion
- Coma
- Seizures, focal neurologic deficits
Acute hypernatremia: symptoms at Na+ ~160 mmol/L. Chronic hypernatremia: symptoms may not appear until Na+ >175 mmol/L (brain adapts by generating "idiogenic osmoles").
Treatment of Hypernatremia
Goal: Correct the water deficit slowly.
Correction rate: No faster than 10 mmol/L/24 hours (0.5 mmol/L/hour).
Rapid correction of chronic hypernatremia causes dangerous cerebral edema because CNS cells still contain excess idiogenic osmoles and will absorb too much water.
- Hypovolemic: 0.9% NaCl first to restore perfusion, then switch to 5% dextrose (D5W) or 0.45% NaCl
- Euvolemic (DI): Free water replacement (oral or IV D5W)
- Hypervolemic: Diuretics + free water replacement
Water deficit formula:
Water Deficit (L) = 0.6 × weight (kg) × [(serum Na / 140) - 1]
PART 2: POTASSIUM (K+) DISORDERS
Normal Values & Physiology
- Normal serum K+: 3.5-5.0 mmol/L
- >98% of total body K+ is intracellular (ICF concentration ~150 mmol/L)
- Only ~2% is extracellular (ECF ~4 mmol/L)
- Small shifts between ICF and ECF produce dramatic changes in serum K+
Regulators of K+ Distribution
| Factor | Effect on Serum K+ |
|---|---|
| Insulin | Drives K+ INTO cells (decrease) |
| Beta-2 agonists | Drives K+ INTO cells (decrease) |
| Acidosis | K+ moves OUT of cells (increase) |
| Alkalosis | K+ moves INTO cells (decrease) |
| Aldosterone | Increases renal K+ excretion (decrease) |
| Osmolarity increase | K+ moves OUT of cells (increase) |
HYPOKALEMIA (K+ < 3.5 mmol/L)
Causes
1. Increased Renal Losses (most common cause)
- Diuretics (loop diuretics, thiazides) - commonest cause
- Hyperaldosteronism (primary - Conn's syndrome; secondary)
- Cushing's syndrome / corticosteroid excess
- Renal tubular disorders: Bartter syndrome, Gitelman syndrome, RTA
- Amphotericin B, aminoglycosides
2. Extrarenal Losses
- Severe diarrhea (intestinal secretions are K+-rich)
- Vomiting (directly + aldosterone activation from volume loss)
- Burns, excessive sweating
3. Transcellular Shift (K+ moves into cells)
- Insulin administration (treatment of DKA) - large K+ influx into cells
- Alkalosis - H+ leaves cells, K+ enters in exchange
- Beta-2 agonists (salbutamol, in asthma treatment)
- Catecholamine surge (acute MI, acute stress)
4. Inadequate Intake
- Starvation, anorexia
- IV fluids without K+ supplementation
- Pica (clay ingestion - binds K+ in GI tract)
Clinical Features of Hypokalemia
Mild (3.0-3.5 mmol/L): Often asymptomatic; possible increased ventricular ectopy
Moderate (<3.0 mmol/L):
- Muscle weakness, fatigue
- Constipation, ileus
- Muscle cramps
- Palpitations
- Polyuria (nephrogenic DI-like effect)
Severe (<2.5 mmol/L):
- Generalized muscle weakness - can progress to paralysis
- Rhabdomyolysis with potential AKI
- Torsades de pointes (life-threatening arrhythmia)
- Bradycardia, tachycardia, atrial/ventricular fibrillation
- Metabolic alkalosis (K+/H+ exchange in cells)
ECG in Hypokalemia:
- Flattened or inverted T waves
- Prominent U waves (most characteristic)
- ST segment depression
- Prolonged QU interval
Treatment of Hypokalemia
| Severity | Treatment |
|---|---|
| Mild (3.0-3.5) | Oral KCl supplementation; dietary K+ (bananas, oranges) |
| Moderate-severe (<3.0) | IV KCl infusion (max 10-20 mEq/hour via peripheral, 40 mEq/hour via central with monitoring) |
| Diuretic-induced | Add K+-sparing diuretic (spironolactone, amiloride) |
Always check and correct magnesium! Hypomagnesemia causes refractory hypokalemia because Mg2+ is needed to maintain intracellular K+. Correcting K+ without correcting Mg2+ will fail.
Preferred salt: KCl (most cases), unless metabolic acidosis present (use potassium citrate).
HYPERKALEMIA (K+ > 5.0 mmol/L)
Severity Classification
| Grade | Serum K+ | ECG changes |
|---|---|---|
| Mild | 5-6 mEq/L without ECG changes | None |
| Moderate | 5-6 with ECG changes, or 6.1-6.5 without | Peaked T waves |
| Severe | >6.5, or 6.1-6.5 with ECG changes | Widened QRS, sine wave |
Causes
1. Pseudohyperkalemia (MUST RULE OUT FIRST)
- Traumatic hemolysis during blood draw (most common cause of "high K+")
- Prolonged tourniquet time or fist clenching
- Extreme leukocytosis (>70,000/cm3) or thrombocytosis (>500×10⁹/L) - K+ released during clotting
- Diagnosed by: serum K+ >0.3 mmol/L higher than simultaneous plasma K+
- Key clue: concomitant elevation of LDH suggests hemolysis
2. Transcellular Shift (K+ moves out of cells)
- Acidosis - H+ enters cells, K+ exits (each 0.1 pH unit drop raises K+ by ~0.6 mEq/L)
- Insulin deficiency (DKA) - combined with hyperosmolarity
- Beta-blockers
- Digitalis toxicity (inhibits Na-K ATPase pump)
- Massive cell breakdown: crush injury, rhabdomyolysis, tumor lysis syndrome, massive hemolysis, burns, GI bleeding with intestinal K+ absorption
3. Decreased Renal Excretion (most common cause of sustained hyperkalemia)
- Advanced renal failure (most common)
- Adrenal insufficiency (Addison's disease) - low aldosterone
- Hypoaldosteronism (type IV RTA, hyporeninemic hypoaldosteronism in diabetics)
- Drugs: ACE inhibitors, ARBs, K+-sparing diuretics (spironolactone, amiloride, triamterene), NSAIDs, trimethoprim, heparin
ECG Changes in Hyperkalemia (Progressive - CRITICAL!)
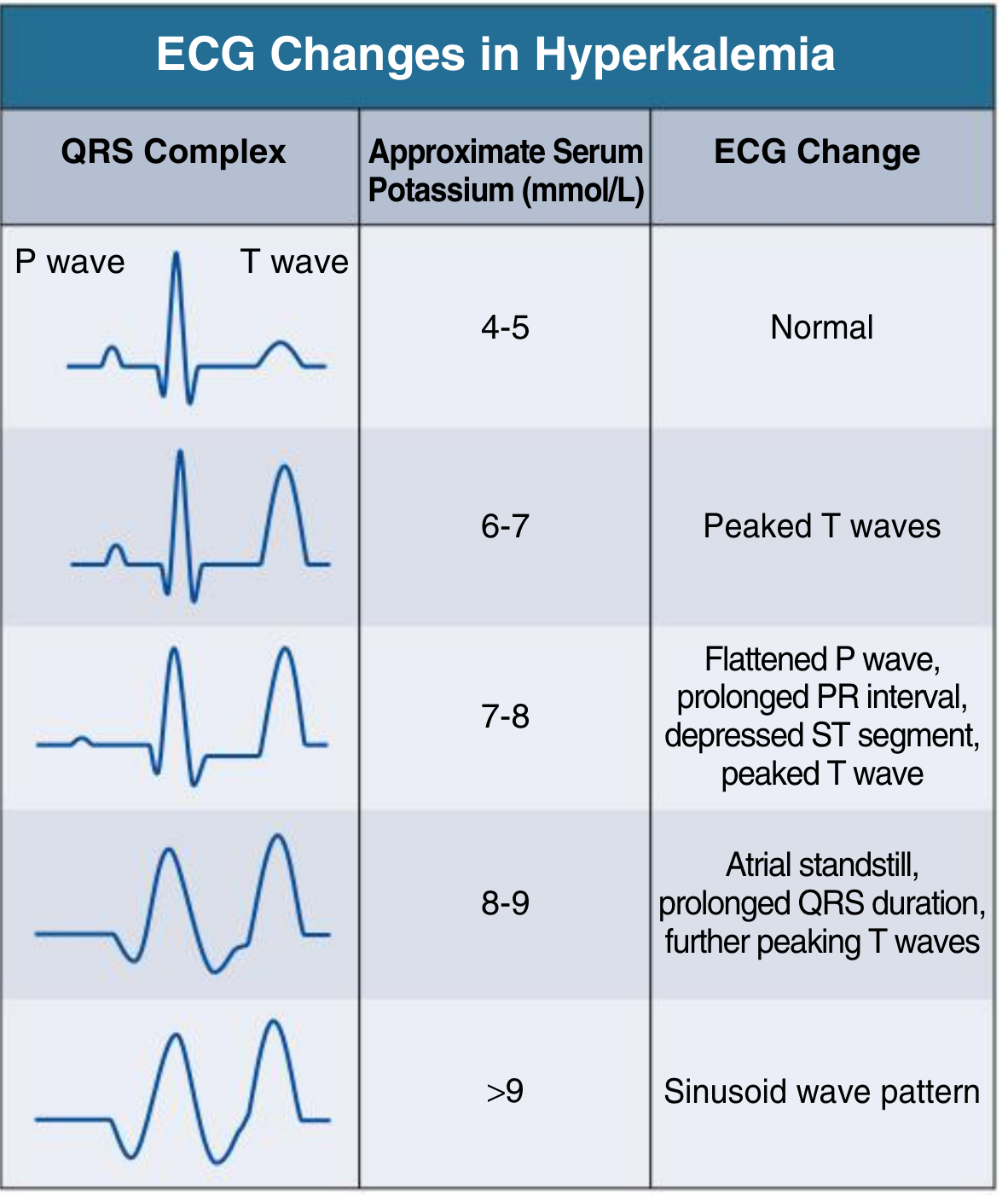
Progressive ECG changes with rising serum potassium. Ventricular fibrillation may occur at any stage of this progression. - Comprehensive Clinical Nephrology, 7th Edition
Sequence to memorize:
- K+ 6-7: Peaked (tented) T waves - earliest change
- K+ 7-8: Flattened P waves, prolonged PR interval, depressed ST segment
- K+ 8-9: Atrial standstill (P waves disappear), widened QRS
- K+ >9: Sine wave pattern - QRS merges with T wave
- Terminal: Ventricular fibrillation, cardiac arrest
Note: ECG changes do NOT always correlate perfectly with K+ levels. A patient can jump from mild to severe cardiac effects unpredictably. ECG is MANDATORY for all hyperkalemic patients.
Clinical Features of Hyperkalemia
- Often asymptomatic until severe
- Muscle pain and weakness (skeletal muscle most sensitive)
- Numbness, paresthesias
- Severe: respiratory failure from diaphragm weakness
- Nausea
- Cardiac arrhythmias (see ECG above) - major mortality risk
- In hyperkalemic periodic paralysis (rare AD disorder, prevalence 1:100,000): transient episodes of paralysis; resting membrane potential shifts from -90 mV to -60 mV, inactivating Na+ channels
Treatment of Hyperkalemia
The three-pronged approach: Stabilize - Shift - Remove
Step 1: Cardiac Membrane Stabilization (works in minutes)
- IV Calcium gluconate (10% solution, 10 mL over 2-3 min)
- Raises threshold for action potentials, reduces membrane excitability
- Does NOT lower serum K+ - just protects the heart
- Indicated when ECG changes are present
- Effect lasts ~30-60 minutes - must follow with definitive treatment
Step 2: Shift K+ into Cells (works in 15-30 min)
- IV Insulin (10 units) + Glucose (50 mL of 50% dextrose) - drives K+ into cells
- Salbutamol (albuterol) nebulization - beta-2 agonist effect
- IV sodium bicarbonate - useful if concurrent metabolic acidosis; promotes K+/H+ exchange
Step 3: Remove K+ from the Body (definitive)
- Furosemide (loop diuretic) - increases renal K+ excretion (if kidneys functional)
- Sodium polystyrene sulfonate (Kayexalate) or newer agents patiromer / sodium zirconium cyclosilicate - K+-binding resins in GI tract
- Hemodialysis - fastest, most effective; indicated for renal failure or extreme hyperkalemia
Step 4: Low K+ diet + Treat underlying cause
Evaluation of Hyperkalemia (Algorithmic Approach)
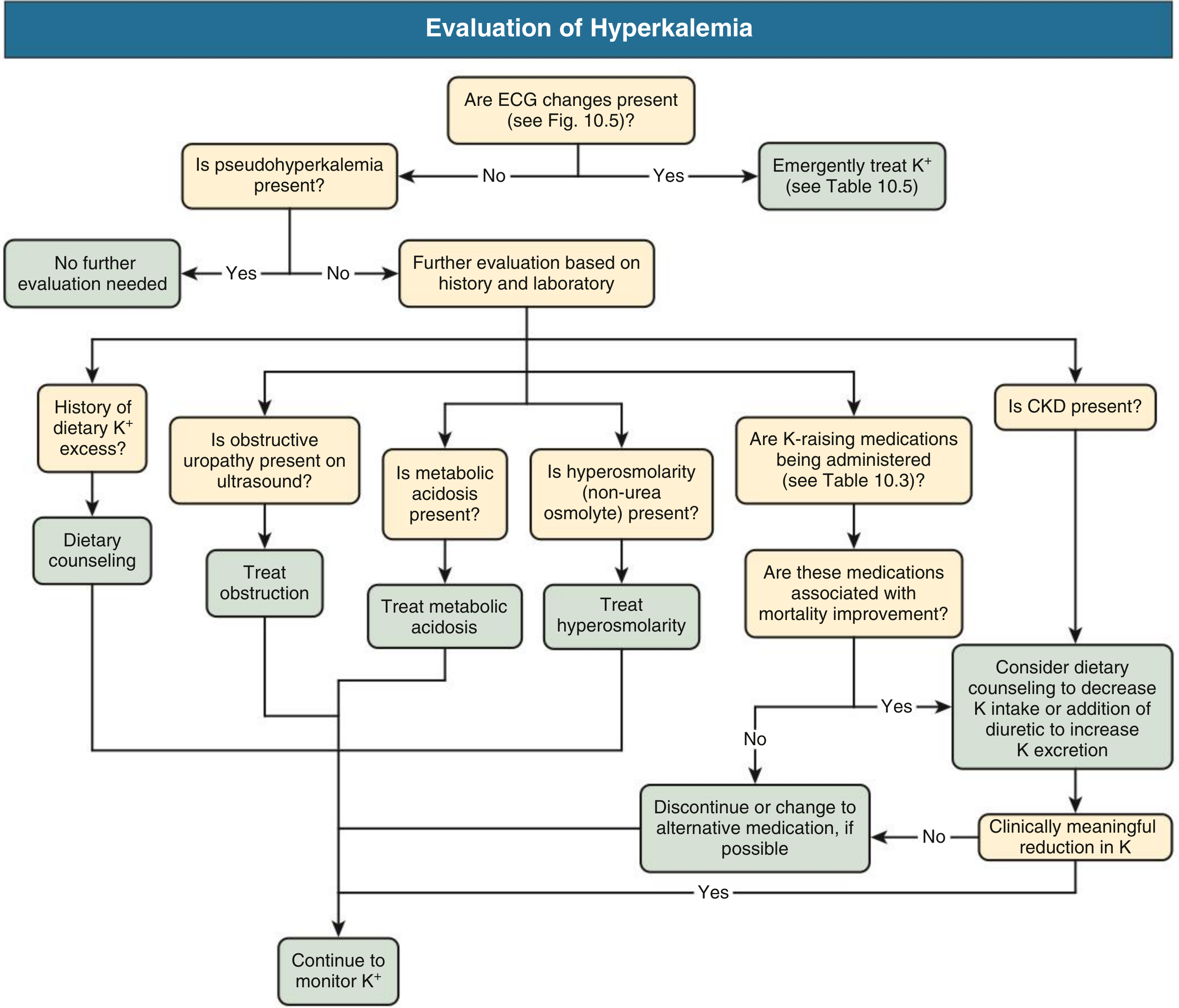
Workup of hyperkalemia - starting with ECG, ruling out pseudohyperkalemia, then systematic evaluation of cause. CKD = chronic kidney disease. - Comprehensive Clinical Nephrology, 7th Edition
QUICK COMPARISON TABLE
| Feature | Hyponatremia | Hypernatremia | Hypokalemia | Hyperkalemia |
|---|---|---|---|---|
| Definition | Na+ <135 | Na+ >145 | K+ <3.5 | K+ >5.0 |
| CNS symptoms | Cerebral edema (confusion, seizures) | Brain shrinkage (confusion, coma) | Minimal | Muscle weakness |
| Cardiac | Rarely affected | Rarely affected | Flattened T, U waves, Torsades | Peaked T, widened QRS, VF |
| Commonest cause | Diuretics/SIADH | DI/dehydration | Loop/thiazide diuretics | Renal failure/pseudohyperkalemia |
| Correction rate | Max 8-10 mmol/L/24h | Max 10 mmol/L/24h | Oral KCl (mild), IV KCl (severe) | Ca-gluconate + insulin/glucose |
| Over-correction danger | Osmotic demyelination (ODS) | Cerebral edema | Hyperkalemia | Hypokalemia |
MEMORY AIDS
For Hyponatremia causes (SIADH mnemonic):
- Small cell lung cancer (most common malignancy)
- Intracranial pathology
- Addison's/Adrenal insufficiency (also causes hyponatremia + hyperkalemia)
- Drugs (SSRIs, carbamazepine, opioids)
- Hypothyroidism
ECG in Hyperkalemia - "PRST going wrong":
- P - peaks (T waves), then P disappears
- R - R/QRS widens
- S - Sinusoid (terminal)
- T - Tented (first sign)
Hypokalemia ECG - "T is Flat, U is Fat" - flattened T waves + prominent U waves
Sources: Goldman-Cecil Medicine, 26th Edition | Comprehensive Clinical Nephrology, 7th Edition | Tietz Textbook of Laboratory Medicine, 7th Edition | Medical Physiology (Boron & Boulpaep) | Ganong's Review of Medical Physiology, 26th Edition | National Kidney Foundation Primer on Kidney Diseases, 8th Edition
This is a shared conversation. Sign in to Orris to start your own chat.