Schedule H drugs
Reading File
Finding Sources
Searching the Web
Schedule H drugs India Drugs Cosmetics Act regulations list
Reading File
Reading File
Here is a thorough overview of Schedule H Drugs under Indian drug law:
Schedule H Drugs - India
Legal Basis
Schedule H is an appendix to the Drugs and Cosmetics Rules, 1945, framed under the Drugs and Cosmetics Act, 1940. It is revised periodically based on advice from the Drugs Technical Advisory Board (DTAB), which is part of the Central Drugs Standard Control Organization (CDSCO) under the Ministry of Health and Family Welfare.
The current list (as notified in March 2006) contains 536 drugs, ranging from Abacavir to Zuclopenthixol.
Definition
Schedule H drugs are prescription-only medicines that:
- Can be sold only against a valid prescription from a registered medical practitioner
- Can only be dispensed in the quantity mentioned in the prescription
- Can be supplied only to licensed parties
- Must not be dispensed more than once unless specifically requested on the prescription
Labeling Requirements
The label/container must prominently display:
- The symbol "Rx"
- The warning: "Schedule H Drug - To be sold by retail on the prescription of a Registered Medical Practitioner only"
- The prescription must mention the name and address of the patient
(Parikh's Textbook of Medical Jurisprudence, p. 4960-4968)
Dispensing Requirements
The pharmacist must maintain a prescription register recording:
- Serial number of the entry
- Date of supply
- Name and address of the prescriber
- Name and address of the patient
- Name of the drug/preparation and quantity supplied
- Batch number and date of expiry (for Schedule C and L drugs)
- Signature of the qualified person supplying the medicine
Dispensing must be done only at an authorised premises (chemist's shop) by or under the supervision of a qualified pharmacist.
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 8184-8196)
Categories of Drugs Included
Schedule H covers a wide range of therapeutic classes, including:
| Category | Examples |
|---|---|
| Antibiotics | Amikacin, Ciprofloxacin, Clarithromycin, Clindamycin, Cefixime, Ceftriaxone |
| Antifungals | Ciclopirox olamine |
| Antivirals | Abacavir, Acyclovir, Nevirapine, Nelfinavir |
| Antihypertensives | Acebutolol, Nifedipine, Nadolol, Nebivolol |
| CNS drugs | Alprazolam, Chlordiazepoxide, Clobazam, Nitrazepam, Olanzapine |
| Antineoplastics | Aclarubicin, Bleomycin, Cisplatin, Nimustine |
| Hormones | ACTH, Norethisterone enanthate |
| Antidiabetics | Nateglinide |
| GI drugs | Cimetidine, Omeprazole, Mosapride |
| Antiprotozoals | Albendazole |
| NSAIDs | Celecoxib, Naproxen, Nimesulide |
| Immunosuppressants | Mycophenolate mofetil |
| Cardiovascular | Nicorandil, Nitroglycerin |
Schedule H vs Schedule H1 vs Schedule X
| Feature | Schedule H | Schedule H1 | Schedule X |
|---|---|---|---|
| Requires prescription | Yes | Yes | Yes |
| Record-keeping | Prescription register | Strict documentation under Rule 65(3)(h) | Mandatory documentation trail |
| Examples | General Rx drugs (536) | High-risk antibiotics, anti-TB, psychotropics, opioids | Habit-forming/narcotic drugs |
| Enforcement | Relatively lax | Stricter | Strictest |
| Label text | "Rx" + Sch H warning | "Rx" + Sch H1 warning | Special warning |
Schedule H1 (introduced later) targets drugs at high risk of misuse, antimicrobial resistance, or addiction - examples include 3rd/4th generation cephalosporins (Cefepime, Ceftriaxone), anti-TB drugs (Capreomycin, Clofazimine), opioids (Buprenorphine), and benzodiazepines (Alprazolam, Chlordiazepoxide).
Other Related Drug Schedules under D&C Rules 1945
- Schedule C - Biological and special products (vaccines, sera, diagnostic antigens)
- Schedule E1 - Poisonous substances under Ayurvedic/Siddha/Unani systems
- Schedule F - Vaccines (Part I), Antisera (Part II), Diagnostic antigens (Part III)
- Schedule G - ~65 drugs (e.g., antihistamines, insulin) requiring "Caution" labeling
- Schedule I - List of 51 diseases for which no drug may be advertised
- Schedule L - Drugs for sale only to hospitals/institutions, not to individuals
- Schedule X - Habit-forming/psychotropic drugs with strictest controls
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 8172-8182; Wikipedia - Schedule H)
Key Point for Exams (MCQ)
"Under the Drugs and Cosmetics Rules, 1945, a Schedule H drug means drugs that can be sold by retail only on the prescription of a registered medical practitioner."
Medical legal issues of a... Incomplete consent.
Finding Sources
Searching the Web
incomplete consent medical legal issues informed consent defects India
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Here is a structured overview of the medico-legal issues of incomplete (defective/invalid) consent:
Medico-Legal Issues of Incomplete Consent
1. Definition
Consent means voluntary agreement, compliance, or permission. Section 13 of the Indian Contract Act defines it as: "two or more persons are said to consent when they agree upon the same thing in the same sense" (meeting of minds).
Section 14 states that consent is free only when it is not caused by:
- (i) Coercion (S.15)
- (ii) Undue influence (S.16)
- (iii) Fraud (S.17)
- (iv) Misrepresentation (S.18)
- (v) Mistake (S.20-22)
(PC Dikshit Textbook of Forensic Medicine and Toxicology, p. 2041-2052)
2. Legal Requirement: Informed Consent
For consent to be legally valid, it must be informed and intelligent - given after understanding what it is given for and the risks involved. The doctor must inform the patient about:
| Information Element | Details |
|---|---|
| (a) Diagnosis | Current condition |
| (b) Nature of treatment/procedure | What will be done |
| (c) Risks involved | Potential complications |
| (d) Prospects of success | Realistic outcomes |
| (e) Prognosis without treatment | Consequences of refusal |
| (f) Alternative methods | Other options available |
What the law requires is two things: (1) the patient be fully informed of every material risk, and (2) the consent itself be based on such disclosure.
(Parikh's Textbook of Medical Jurisprudence, p. 3239-3253)
3. When Consent is INVALID (Incomplete/Defective)
The consent given may be invalid because:
| Ground | Example |
|---|---|
| (a) Act consented to is unlawful | Consent for a criminal abortion |
| (b) Given by one with no legal capacity | A minor (<18 yrs) or a mentally ill person |
| (c) Not an informed consent | Patient not told of risks, diagnosis, alternatives |
| (d) Obtained by misrepresentation or fraud | Doctor concealed material facts |
| (e) Given under coercion or undue influence | Consent signed under duress |
| (f) Blanket/general consent | "Do whatever is best" forms with no specific procedure mentioned |
| (g) Consent for one procedure - different procedure done | Consent for appendectomy but hysterectomy performed |
(Parikh's Textbook of Medical Jurisprudence, p. 3286-3325)
4. Legal Consequences of Incomplete Consent
A. Assault and Battery (Criminal/Tort)
"To examine, treat or operate upon a patient without consent is regarded as assault in law, even if it does not cause any harm, even if it is beneficial and done in good faith - for which the patient may sue for damages."
- Assault = threatening a patient with physical examination or procedure without consent
- Battery = the actual unlawful touching/procedure without valid consent
- Battery is an intentional tort - does not require proof of harm or negligent intent
- A physician commits battery by treating a patient without consent, even if the treatment was successful
(PC Dikshit Textbook of Forensic Medicine, p. 2059; Scott-Brown's Otorhinolaryngology, Vol 1)
B. Negligence (Civil/Malpractice)
- Lack of informed consent (as opposed to no consent at all) is typically framed as professional negligence/malpractice
- The doctor failed to disclose information a reasonable patient would need to make a decision
- Requires proof that the incomplete disclosure caused harm
C. Professional Misconduct
- The Medical Council of India (MCI) considers operating without consent as serious professional misconduct
- Can result in disciplinary action, suspension, or erasure from the medical register
- Performing operations that result in sterilisation without consent of both spouses is misconduct
5. Specific Situations of Incomplete/Defective Consent
Minors
- Legal age for consent in India = 18 years
- A child >12 years may consent to physical/medical examination (IPC S.89)
- For any procedure on a child <18 years, parental/guardian consent is mandatory
- Case: A minor was taken for tonsillectomy by two adult sisters (not parents). The child died under anaesthesia. Court ruled there was no emergency to justify operating without parental consent; father recovered damages.
Blanket Consent Forms
- "Do whatever you think best for me" forms are not valid in court
- Consent must be procedure-specific
- An all-encompassing consent authorising any test/surgery is void
Unilaterally Executed Consent
- Consent signed only by the patient and not countersigned by the doctor is of questionable validity
- Witnessed consents are legally more dependable
Surgical vs. Anaesthesia Consent
- Surgical consent does not cover anaesthesia care - separate anaesthesia consent is required
Repeat Procedures
- Fresh consent must be obtained before every surgical re-exploration - consent from a prior procedure does not extend to a second one
Consent for Sterilisation
- Operations resulting in sterility require written consent of both husband and wife (MCI Ethics Regulations 2002)
6. Exceptions Where Consent May Be Incomplete or Absent (Legally Permitted)
| Exception | Condition |
|---|---|
| Emergency | Unconscious patient, life-threatening condition; consent implied; but surgical procedures must not go beyond the minimum needed to save life |
| Incompetence | Unconscious, delirious, severely psychotic patients; surrogate/proxy consent must be obtained if time allows |
| Therapeutic privilege | Full disclosure would cause serious psychological harm to the patient; doctor must document the reason and preferably obtain consent from a responsible relative |
| Waiver | Patient explicitly delegates decision to the physician or a third party |
If one of these exceptions applies, the physician must document the specific exception and circumstances. Emergency is the only situation where neither time nor disclosure may be possible.
(PC Dikshit Textbook of Forensic Medicine and Toxicology, p. 2127-2161)
7. Practical Medico-Legal Safeguards
- Consent must be procedure-specific, not general
- Must be obtained before (not during or after) sedation/anaesthesia
- Written consent has the advantage of easy proof and permanent form
- Oral consent is valid if properly witnessed by a disinterested third party
- Video-recording of the consent process (with prior consent for recording) is increasingly used for major/organ transplant procedures
- The patient's name and address must be mentioned on the prescription/consent form
- The patient retains the right to withdraw consent at any time
(Parikh's Textbook of Medical Jurisprudence, p. 3295-3325; PMC - Consent and the Indian Medical Practitioner)
Quick Summary for Exams
Incomplete consent = legally no consent.
- No consent at all → Assault + Battery (even if no harm, even if beneficial)
- Consent without adequate information → Negligence/Malpractice
- Either can also lead to professional misconduct charges before the MCI/State Medical Council
Surest sign of identification
Finding Sources
Searching the Web
surest sign of identification forensic medicine dental fingerprint DNA
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Surest Sign of Identification in Forensic Medicine
The Answer
Fingerprints (Dactylography) are classically considered the surest/most reliable sign of personal identification in forensic medicine - yielding what textbooks call "absolute identification."
In modern forensic practice, DNA fingerprinting is the current gold standard, as it is even more discriminatory. The two are complementary: fingerprints are faster and cheaper; DNA is definitive even from trace biological material.
1. Fingerprints (Dactylography) - The Classical Surest Sign
Why fingerprints are the surest:
"Absolute identification is possible" - the fingerprint system is the only guide to establish identity which is unfailing in practice.
(Parikh's Textbook of Medical Jurisprudence, p. 6837)
Key properties that make fingerprints uniquely reliable:
| Property | Detail |
|---|---|
| Individuality | No two persons have identical fingerprints - 1 chance in 64 billion of two persons sharing the same pattern (Quetlet's rule) |
| Permanence | Patterns form by 24 weeks intrauterine life and remain unchanged throughout life and after death |
| Uniqueness even in twins | Pattern is different even in identical twins |
| Not inherited | Patterns are not passed from parent to child (paternity cannot be proven by fingerprints) |
| Recoverable from decomposed bodies | Prints can be obtained from putrefied bodies, burnt skin, or skin peeled off by drowning |
| No special equipment needed | Applicable to all ages, easily classified |
| Transmissible | Can be transmitted as coded/digitalised messages; AFIS (Automated Fingerprint Identification System) allows rapid identification |
Minimum points for positive ID:
- The Indian Supreme Court ruling states that a minimum of 8 ridge characteristics must match for positive fingerprint identification.
- In world crime records, no two identical fingerprint patterns have ever been reported.
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 8083-8095)
2. The Four Main Fingerprint Patterns
Arch (6-7%) - ridges run from one side to the other with an arch in the middle:
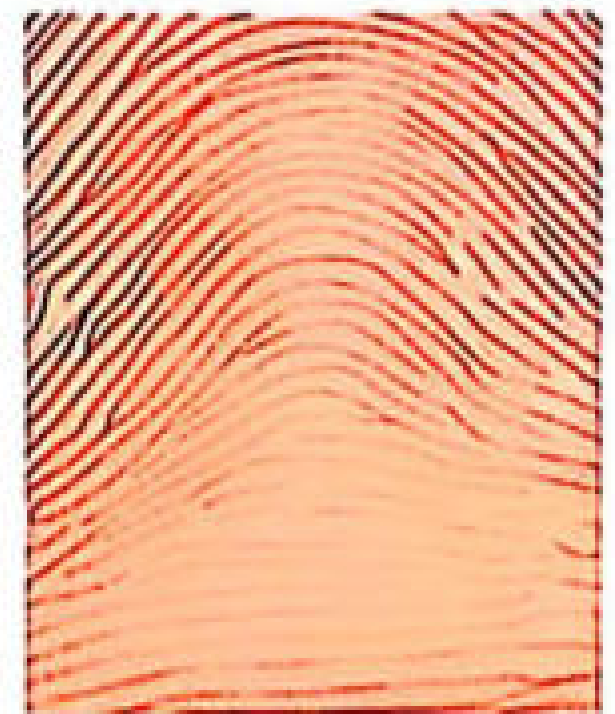
Loop (60-70%, commonest) - ridges enter from one side, form a curve, and exit the same side; has a Core and Delta:
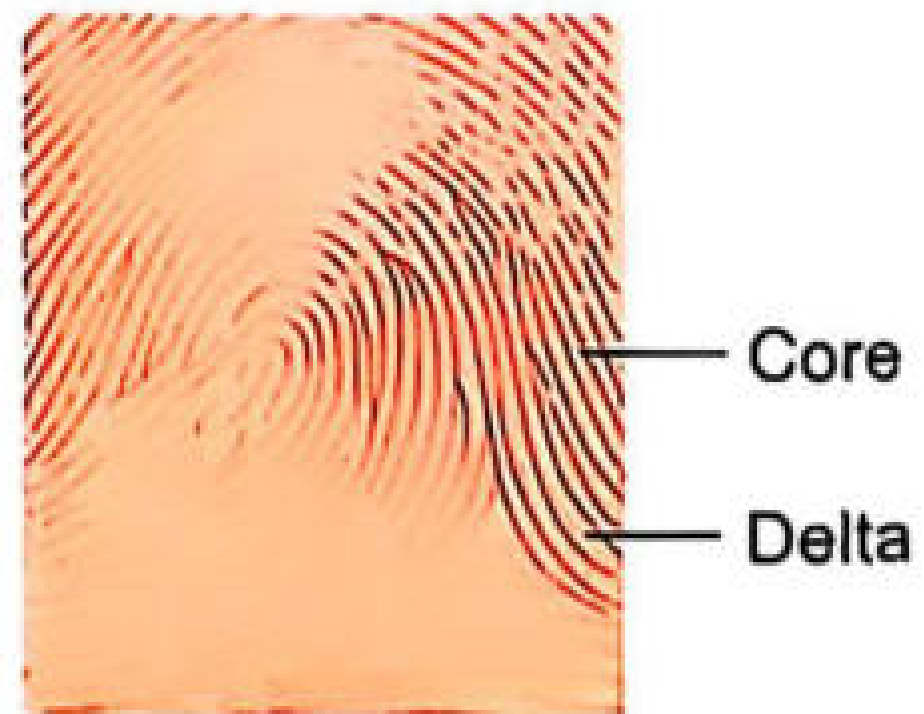
Whorl (25-35%) - ridges form circles/spirals around the core; has Core and Delta:
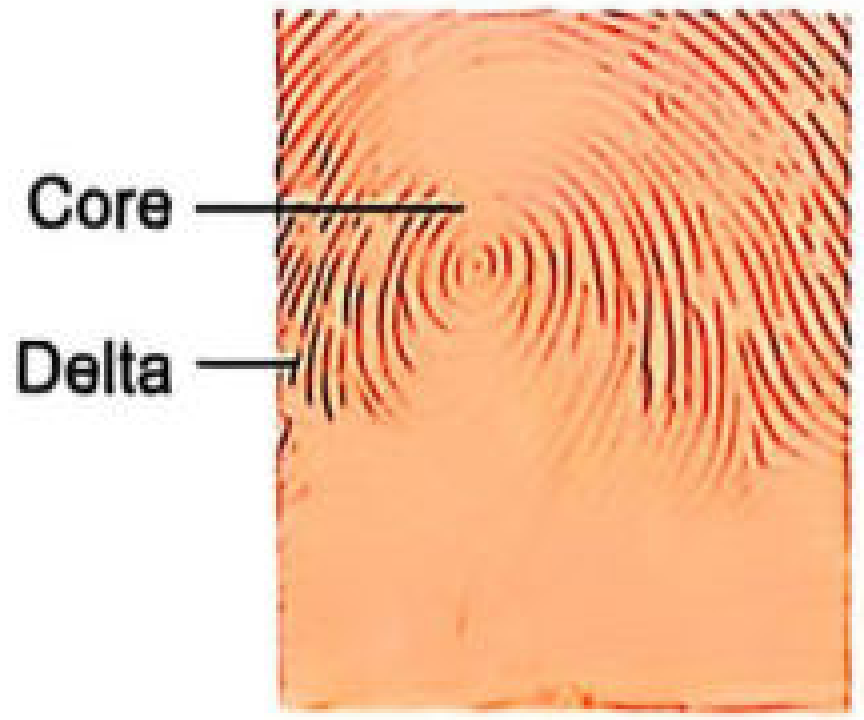
Composite (1-2%) - combination of two or more types.
3. Identification Process (How Fingerprints are Compared)
Final identification is made by comparison of ridge characteristics (NOT by pattern alone):
- Ridge endings
- Bifurcations
- Lake formations
- Island formations
The sequence and arrangement of these characteristics across the ridge areas is what uniquely identifies an individual.
Poroscopy (described by Henry Locard): Study of microscopic pores on fingerprint ridges. Each mm of ridge contains 9-18 pores. Useful when only fragments of fingerprints are available with no identifiable pattern.
4. DNA Fingerprinting - The Modern Gold Standard
Developed by Dr. Alec Jeffreys in 1984/1985, DNA fingerprinting revolutionised forensic identification:
| Feature | Detail |
|---|---|
| Unique to every individual | Except identical twins (even more discriminatory than fingerprints) |
| Source | Blood, saliva, semen, hair root, teeth (dental pulp), bone marrow |
| Teeth as best DNA source | Dental pulp is surrounded by dentin and enamel - forms a "dental armor" protecting DNA from extreme environmental conditions |
| Applications | Criminal investigation, paternity testing, mass disaster victim identification, identifying decomposed/burned remains |
"Before the development of DNA fingerprinting, identification of criminals was far less scientific."
(Basic Medical Biochemistry - A Clinical Approach, 6e)
For mass disasters (e.g., aircraft crashes): The recommended sequence is:
- First attempt fingerprinting
- Then dental identification and comparative antemortem/postmortem X-rays
- If unsatisfactory - use DNA typing
(DiMaio's Forensic Pathology, 3rd ed.)
5. Comparison of Identification Methods
| Method | Reliability | Survives decomposition | Needs antemortem record | Key limitation |
|---|---|---|---|---|
| Fingerprints | Absolute (classical surest) | Yes (even from dermis) | No | Skin must be intact enough |
| DNA fingerprinting | Gold standard (modern) | Yes (from teeth, bone) | Need reference sample | Expensive; needs comparison sample |
| Dental records | Highly reliable | Yes (teeth most resistant) | Yes - essential | No universal dental database |
| Radiological comparison | As reliable as dental | Yes | Yes (antemortem X-rays) | Less commonly used |
| Visual/facial recognition | Unreliable | No | No | Subject to considerable error |
Summary for Exams
Classical/traditional answer: Fingerprints = surest sign of identification ("absolute identification is possible")Modern/current answer: DNA fingerprinting = gold standard (most discriminatory)MCQ tip: If the question says "surest" or "most reliable" in a forensic/traditional context - Fingerprints. If it says "most accurate" or "modern gold standard" - DNA profiling.
Antemortem vs postmortem blood clot
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Excellent material gathered from both forensic and pathology textbooks. Here is a comprehensive comparison:
Antemortem vs Postmortem Blood Clot
The Key Principle
An antemortem clot (thrombus) forms during life in flowing or sluggish blood as part of a pathological process. A postmortem clot forms after death due to passive settling of blood in stagnant vessels. Distinguishing them at autopsy is a critical forensic and pathological skill.
Comprehensive Comparison Table
| Feature | Antemortem Clot (Thrombus) | Postmortem Clot |
|---|---|---|
| Time of formation | During life | After death |
| Consistency | Firm, dry, tough, rubbery | Soft, gelatinous, jelly-like, friable |
| Surface | Rough, dull, transversely ridged | Smooth, shiny, glistening |
| Appearance | Variegated - pale and dark areas | Homogeneous (uniformly red or yellow) |
| Colour | Dark red to grey-red, varying from place to place | Dark red ("red currant jelly") OR pale yellow ("chicken fat") OR mixture |
| Lamination | Laminated - shows pale and dark alternating layers | Non-laminated, homogeneous |
| Lines of Zahn | Present - pale platelet/fibrin layers alternating with red cell-rich layers | Absent - no fine white lines of fibrin (striae of Zahn) |
| Adherence to vessel wall | Firmly adherent to lining endothelium | Weakly adherent or not attached at all |
| Moisture | Dry | Wet looking, moist |
| Elasticity | Firm, inelastic | Elastic (if fibrin content is high) |
| Blood coagulation status | Clotted, laminated, firmly adherent | Blood may not clot soon after death; if clot forms, it is non-laminated |
| Composition | Fibrin + RBC + platelets (especially arterial) | Mainly fibrin + RBC; platelets poor |
| Vessel cast | Does not form perfect cast | Forms a perfect cast of vessel and its branches |
| When lung sliced | Emboli project slightly above cut surface | Clot does not pour out of cut small vessels |
| Vital reaction | Present (leucocyte infiltration, inflammation) | Absent |
| Histology | Leucocyte + RBC infiltration between muscle fibres | Vessels distended with clot; no cellular infiltration outside vessel wall |
(Parikh's Textbook of Medical Jurisprudence, p. 10258-10267; Robbins & Kumar Basic Pathology, p. 2579-2593)
The Two Types of Postmortem Clots
Postmortem clots form in two patterns depending on speed of clotting after death:
1. Red Currant Jelly Clot
- Blood clots rapidly after death
- Result: soft, lumpy, uniformly dark-red, slippery, moist clot
- Red cells are uniformly distributed throughout the fibrin mesh
2. Chicken Fat Clot
- Red cells sediment by gravity before blood coagulates
- Lower (dependent) portion: dark red clot (red cells)
- Upper portion: pale or bright yellow layer of serum + fibrin = "chicken fat"
- Usually a mixture of both types is seen
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 1164-1182)
Lines of Zahn - The Pathognomonic Feature
"Lines of Zahn represent pale platelet and fibrin layers alternating with darker red cell-rich layers. Such lines are significant in that they are only found in thrombi that form in flowing blood; their presence can therefore distinguish antemortem thrombosis from the bland non-laminated clots that form in the postmortem state."
(Robbins & Kumar Basic Pathology, p. 2579-2582)
- Present = Antemortem thrombus (formed in flowing blood)
- Absent = Postmortem clot (formed in stagnant blood)
- Even venous thrombi (low-flow) show ill-defined laminations, distinguishing them from postmortem clots
Agonal Thrombi - A Third Category
Formed in a person dying slowly with circulatory failure:
- Firm, stringy, tough, pale yellow
- Form in cardiac cavities (usually right side - right atrium/ventricle)
- Extend into pulmonary artery and branches like a tree-like cast
- Can be mistaken for postmortem clot but are firmer and paler
Postmortem Fluidity of Blood
An important associated concept:
- Shortly after death, blood is usually fluid
- If autopsy is done a few hours after death - blood may be partly clotted, partly fluid
- Uncoagulable fluid blood in limb vessels/heart is normal in sudden death and does NOT indicate cause of death
- In asphyxial deaths - blood is classically fluid and incoagulable
- Mechanism: fibrinolysins are liberated from vascular endothelium; plasminogen activator is released through agonal-period vasoactive mediators
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 1184-1197)
Significance of Haemorrhage in Antemortem vs Postmortem Wounds
| Feature | Antemortem | Postmortem |
|---|---|---|
| Amount | Usually copious, arterial | Slight, venous only |
| Arterial spurting | Present (spurring marks) | Absent - only oozing |
| Clot in wound | Laminated, firmly adherent, rubbery, variegated | Non-laminated, homogeneous, soft, chicken fat/currant jelly |
| Tissue staining | Deep infiltration, cannot be washed away | Superficial, can be washed away |
(Parikh's Textbook of Medical Jurisprudence, Table 18.1)
Quick Summary for Exams
| Antemortem | Postmortem | |
|---|---|---|
| Consistency | Firm, dry | Soft, jelly-like |
| Lamination | Yes (Lines of Zahn) | No |
| Adherence | Firm | Weak/absent |
| Colour | Variegated (grey-red) | Uniform (red or yellow) |
| Vital reaction | Present | Absent |
| Vessel cast | No | Yes (perfect cast) |
| Platelets | Rich | Poor |
Key MCQ: Lines of Zahn are seen in - Antemortem thrombus (formed in flowing blood)Key MCQ: "Chicken fat" and "currant jelly" clots are - Postmortem clots
Give me like 6-7 main differences which i can remember
Here are the 7 key differences, easy to memorize:
| # | Feature | Antemortem Clot | Postmortem Clot |
|---|---|---|---|
| 1 | Consistency | Firm, dry, tough | Soft, jelly-like, friable |
| 2 | Colour | Variegated (grey-red, mixed) | Uniform - red ("currant jelly") or yellow ("chicken fat") |
| 3 | Lines of Zahn | Present (pale fibrin/platelet layers alternating with red) | Absent |
| 4 | Adherence | Firmly adherent to vessel wall | Weakly adherent or free |
| 5 | Lamination | Laminated (layered) | Non-laminated, homogeneous |
| 6 | Vessel cast | Does NOT form a cast | Forms a perfect cast of the vessel |
| 7 | Vital reaction | Present (leucocyte infiltration, inflammation) | Absent |
Memory Trick
"FLAVCV" - Firm, Laminated, Adherent, Variegated, Cast (no), Vital reaction present = Antemortem
Everything is the opposite for postmortem.
The single most important distinguishing feature = Lines of Zahn → Antemortem only
Locards principle
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Locard's Exchange Principle
Who Formulated It?
Dr. Edmond Locard (1877-1966) - French criminologist, Director of the first crime laboratory in Lyon, France. Also described Poroscopy (identification via fingerprint pore patterns).
The Principle (Exact Statement)
"Whenever two objects come into contact, there is an exchange of materials between them."
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 5892-5903)
Simply put: "Every contact leaves a trace."
What It Means
When a criminal comes into contact with a person, object, or crime scene:
- Traces FROM the scene are carried away on the criminal (on body, clothing, tools)
- Traces FROM the criminal are left at the scene
- This exchange is mutual and unavoidable
Types of Trace Evidence Left Behind
| Source | Examples |
|---|---|
| Criminal on scene | Fingerprints, footprints, hair, blood, semen, saliva, sweat |
| Scene on criminal | Soil/mud, fibres, glass fragments, paint, pollen, dust |
| Between persons | Skin cells under victim's fingernails, fibres transfer, blood splatter |
| Tools/weapons | Tool marks, scratches, paint transfer, blood stains |
"Wherever a criminal goes, whatever he touches, and whatever he leaves will serve as silent evidence against him."
Significance in Forensic Investigation
1. Links criminal to crime scene
Physical evidence can objectively connect a suspect to a victim, weapon, or scene - even without eyewitness testimony.
2. Why crime scene preservation matters
Every person who enters a crime scene deposits new trace material and removes existing material - contaminating evidence. This is why the scene must be sealed immediately.
3. Physical evidence is superior to eyewitness testimony
"Physical evidence cannot be wrong and completely absent. Only its interpretation can be incorrect. Only human failure to find, study, and understand it can diminish its value."
4. Three sources of physical evidence:
- Scene of crime
- The victim
- The suspect
5. Chain of evidence must be maintained
Evidence must be marked, labelled (date, time, place, by whom collected) and preserved in the exact condition found.
Locard's Other Contribution - Poroscopy
Locard also described poroscopy - the study of microscopic pores on fingerprint ridges for identification. Each mm of ridge contains 9-18 pores. Useful when only fragments of fingerprints are available with no identifiable pattern.
(Parikh's Textbook of Medical Jurisprudence, p. 6943)
Exam Summary
| Point | Detail |
|---|---|
| Principle | Every contact leaves a trace - bidirectional exchange |
| By whom | Dr. Edmond Locard (French criminologist) |
| Applied to | Crime scene investigation, linking suspect to scene/victim |
| Other contribution | Poroscopy (fingerprint pore identification) |
| Key statement | "Wherever a criminal goes, whatever he touches...silent evidence against him" |
Trace evidence
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Trace Evidence
Definition
Trace evidence refers to small (often microscopic) physical materials that are transferred between persons, objects, or crime scenes during contact. It is the practical basis of Locard's Exchange Principle - "every contact leaves a trace."
"Wherever a criminal goes, whatever he touches, and whatever he leaves will serve as silent evidence against him."
Role in Forensic Investigation
Trace evidence serves to:
- Link a suspect to a crime scene or victim
- Link a victim to a suspect
- Link a weapon to a crime
- Reconstruct the sequence of events
- Corroborate or contradict eyewitness testimony
Physical evidence cannot be wrong - only its interpretation can be incorrect. Eyewitness evidence may fail due to partisanship, faulty memory, or defective observation.
Types of Trace Evidence and Their Forensic Significance
1. Blood
- Found at scene, on accused's clothing, or on weapon
- Distribution and pattern of bloodstains helps reconstruct the crime
- Blood grouping useful in disputed paternity
- Criminal may also bleed (from struggle, accidental injury during crime)
2. Semen
- Found on clothes of victim/accused, pubic hair, bedding, floor
- UV light (fluorescence) useful to detect semen stains on garments
- Critical in sexual offence cases
3. Fingerprints
- Latent prints left on weapons, surfaces, door handles
- Can identify the criminal even without other evidence
- Also used to identify dead bodies, amnesia victims, persons using aliases
4. Hair
- Retains traces of dietary elements, drugs, and environmental toxins (measurable by neutron activation analysis)
- Hair pulled from criminal by objects at scene, or victim's hair on criminal's clothing/weapon
- In sexual offences - victim's hair found on genitals of accused and vice versa
- Animal hair useful in cases of bestiality or cattle theft
- Hair stuck to a vehicle useful in hit-and-run cases
5. Fibres
- May be animal, vegetable, mineral, or synthetic origin
- Transfer between criminal's clothes and victim/scene during assault, burglary, theft
- Clothing constantly carries loose fibres
- If a fibre from one source exactly matches another source → definite probability of contact
6. Glass
- In hit-and-run - fragments from broken lamp found on vehicle bumper
- Burglars may carry window glass fragments in clothes
- Identified by: refractive index, specific gravity, UV fluorescence, spectroscopic/chemical analysis
7. Paint
- In road accidents - paint flakes from vehicle found on victim/ground; traces from object found on vehicle
- In burglaries - paint from walls/doors/safe found on criminal's clothing or tools
8. Wood
- Splinters from tool handles found at scene matched to tool seized from suspect
- Identified by: microscopy of cell structure, paint analysis, fracture matching
9. Metals
- Metal fragments from tool used at crime may be recovered from criminal's clothing
- Identified by: chemical analysis or spectroscopy
10. Tool Marks
- Every tool leaves characteristic compression, scraping, or cutting marks
- Wear creates individuality transmitted to the object worked upon
- Two types: compression marks and scrape marks
- Identified by: density, pigment distribution, spectrographic analysis, microscopy
11. Poisons
- Identified from body fluids, viscera, stains at scene
- Presence of visible injuries or disease does not rule out co-existing poisoning
12. Firearms Evidence
- Bullet recovered from body identifies type of gun and ammunition
- Markings on bullet can identify the specific firearm that discharged it
13. Soil/Vegetation
- Unique soil composition from crime scene found on suspect's shoes/clothing
- Sample of soil/vegetation taken from scene compared with control sample
Collection of Trace Evidence - Key Rules
| Rule | Detail |
|---|---|
| Crime scene preservation | Nothing should be changed, added, removed, or destroyed |
| Paper bags on hands | Before transporting body - to preserve trace evidence under fingernails/in hands (NOT plastic - plastic causes condensation and loss) |
| Victim's clothing | Never discarded on floor - victim should undress standing on a clean sheet of paper to catch dislodged evidence |
| Clothing instructions | Air dry, hold as evidence, maintain chain of custody |
| Doctor at scene | Must NOT smoke, throw cigarette stubs/matches - these add false trace evidence |
| Control sample | Always collect unstained samples alongside stained ones to rule out false positives |
| Chain of evidence | Must be intact - label with date, time, place, by whom collected, from whom taken |
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 5892-6068; Parikh's Textbook of Medical Jurisprudence, p. 5162-5208)
Quick Summary for Exams
| Type | Crime | Key Test/Feature |
|---|---|---|
| Blood | Murder, assault, rape | Blood group, DNA, spatter pattern |
| Semen | Sexual offences | UV fluorescence |
| Hair | Sexual offences, hit-and-run | Neutron activation analysis |
| Fibres | Assault, burglary | Fibre matching |
| Glass | Hit-and-run, burglary | Refractive index, spectroscopy |
| Paint | Road accidents, burglary | Spectrographic analysis |
| Fingerprints | Any crime | Latent print development |
| Tool marks | Burglary | Compression/scrape mark comparison |
MCQ: Role of trace evidence = Links a suspect to a crime scene or object
Ommition and commition in infanticide
Finding Sources
Finding Sources
Reading File
Reading File
Acts of Commission vs Omission in Infanticide
Definition
Infanticide = the killing of a newborn child (usually within the first year of life) by the mother or others. The criminal causes of infant death are classified into:
(1) Acts of Commission - active violence or poisoning (2) Acts of Omission - criminal neglect; failure to perform a duty
Acts of COMMISSION
(Actively doing something to kill the infant)
These involve mechanical violence or poisoning. Death can occur in the same ways as in adults but certain methods are more common:
1. Suffocation
- Pressing the face on a pillow, or closing the nose and mouth by cloth/hands
- May leave no external marks if minimal force used
- More force than necessary → bruising of inner aspects of lips
- Sometimes mucus and squamous respiratory epithelium from the infant found in the smothering material
- Infants also suffocated by pressure on the chest
- Foreign bodies (rag, cotton wool) in mouth/air passages + internal signs of asphyxia = homicidal suffocation
2. Strangulation
- By hand (manual) or by ligature
- Manual strangulation → bruises from finger pressure, scratches from nails, injury to deeper tissues
- Ligature strangulation → ligature frequently left in situ (preserve as evidence)
- Important: Natural skin folds on neck of fat infants can resemble ligature marks - close dissection needed to differentiate
- Umbilical cord sometimes used as a ligature to simulate accident; displaced Wharton's jelly indicates rough handling
3. Drowning
- Infant thrown into water, bucket, toilet, etc.
4. Fracture of the Skull
- Blunt force to head; must be distinguished from birth injuries (especially in unattended deliveries)
5. Fracture and Dislocation of Cervical Vertebrae
- May occur from forcible rotation of neck during attempted delivery correction (can mimic birth injury)
6. Other Injuries (Rare)
- Stab wounds by needles, pins, or scissors penetrating heart, brain, or medulla
- Concealed punctures to check for: fontanelles, inner canthus of eye, nostrils, throat, nape of neck, up the rectum - these are easily missed at autopsy
7. Poisoning
| Region | Agents Used |
|---|---|
| India/some countries | Opium, calotropis juice, madar, tobacco, dhatura |
| Other countries | Insulin, antihistamines, tranquillisers, hypnotics |
In suspicious cases - stomach and other viscera must be preserved for chemical analysis
Acts of OMISSION
(Failing to do something necessary for survival)
"The law presumes that a woman who is about to deliver should take ordinary precautions to save her child after it is born. She is guilty of criminal negligence if she fails to do so."
Deaths from omission at birth relate to failure to perform 5 key duties:
| # | Omission | What Should Have Been Done |
|---|---|---|
| 1 | No preparation for birth | Arrange medical aid as soon as labour pains begin |
| 2 | Failure to tie the umbilical cord after dividing it | Tie cord to prevent fatal haemorrhage |
| 3 | Failure to remove the child from mother's discharges | Remove amniotic fluid/blood from airways to prevent aspiration |
| 4 | Failure to protect child from cold/heat | Provide warmth and shelter |
| 5 | Failure to supply food | Breastfeed or provide nutrition |
Legal Position on Omission
- Evidence that no provision of any kind was made for the birth suggests intent to kill the child
- Exception: if the woman was unaware of her pregnancy until delivery, or if she fainted due to sudden violent labour pains
Abandoning of Children (Related Offence)
Under Section 317 IPC - whoever, being a parent or having care of a child under 12 years, exposes or leaves the child with intention of wholly abandoning it is punishable.
- If the child dies as a result → may be tried for murder or culpable homicide
(Parikh's Textbook of Medical Jurisprudence, p. 12314-12505)
Quick Summary Table
| Commission | Omission | |
|---|---|---|
| Nature | Active killing | Passive neglect |
| Methods | Suffocation, strangulation, drowning, skull fracture, cervical injury, stab, poison | Failure to prepare, tie cord, clear airway, protect from cold, feed |
| Evidence | Marks of violence, asphyxia signs, foreign bodies, poison in viscera | No provisions made, umbilical cord untied, hypothermia |
| Legal principle | Direct homicide | Criminal negligence |
Acts in infanticide
Finding Sources
Reading File
Reading File
Reading File
Reading File
Acts/Laws Related to Infanticide
In INDIA
1. Indian Penal Code (IPC) - Section 302
- Infanticide = unlawful destruction of a newly born child
- Regarded as murder in Indian law
- Punishable by: death or transportation for life + fine
- Key requirement: prosecution must prove the child was born alive
- Legal presumption = child is born dead (burden of proof on prosecution)
2. Definition of "Born Alive" - Indian Law
"Any part of a living child brought forth external to the mother - even if the child has not breathed or is not completely born - constitutes live birth and therefore homicide."
- More liberal (protective) than English law
- Applies to both mother AND father (unlike English Acts which apply only to the mother)
- Killing before any part of the child is born = not homicide (foeticide instead)
3. Section 317 IPC - Exposure and Abandonment
- Abandoning a child under 12 years with intent to wholly abandon
- If the child dies = tried for murder or culpable homicide
4. Section 318 IPC - Concealment of Birth
- Secretly burying or disposing of the dead body of a child to conceal birth
- Live birth need NOT be proved - sufficient that birth occurred and child was dead at time of concealment
- A foetus is considered a child if it has attained maturity capable of separate existence
- When infanticide cannot be proved, the mother is usually charged with this lesser offence
In ENGLAND (For Comparison/Exam)
1. Infanticide Act 1922 (England only)
- First law recognising that effects of delivery can disturb the mother's mind
- Made provision for reduced charge if mother's mental balance was disturbed at the time
- Applicable only to England (not Ireland or Scotland)
- No age limit defined; did not account for lactation
2. Infanticide Act 1926
- Re-enacted the 1922 Act
- Defined age limit = child under 12 months
3. Infanticide Act 1938 (Most Important)
"Where a woman by any willful act or omission causes the death of her child being a child under the age of 12 months, but at the time of the act or omission the balance of her mind was disturbed by reason of her not having fully recovered from the effect of giving birth to the child OR by reason of the effect of lactation consequent upon the birth of the child..."She is guilty of infanticide and punished as if she had committed manslaughter (not murder)
Key features:
| Point | Detail |
|---|---|
| Who | Only the mother (husband or others = murder/manslaughter) |
| Child's age | Under 12 months |
| Mental state | Balance of mind disturbed at time of act |
| Causes | Effects of delivery OR lactation (broader than 1922 Act) |
| Punishment | As for manslaughter (not murder) |
| Proof | Doctor + psychiatrist must prove disturbed mental balance |
Requirements for this Act to apply:
- Only the mother can be charged
- Child must be born alive (and viable)
- Child must have been killed
- Mother must show evidence of disturbed mental balance
4. Infant Life (Preservation) Act 1929
- Deals with destruction of children at or before labour (before complete birth)
- Crime = child destruction
- Criteria: pregnancy of 28 weeks or more; child capable of being born alive
- Punishment: imprisonment for life
- If not guilty of murder/manslaughter/infanticide → can be charged with child destruction
5. Criminal Law of England
- Child "born alive" only when completely born external to mother (irrespective of cord)
- Destruction before complete birth = not homicide (Indian law is considered more correct here)
Summary Comparison Table
| Law | Country | Key Feature |
|---|---|---|
| IPC S.302 | India | Infanticide = murder; both parents liable |
| IPC S.317 | India | Abandonment of child <12 years |
| IPC S.318 | India | Concealment of birth |
| Infanticide Act 1922 | England | First recognition of disturbed mind defence |
| Infanticide Act 1938 | England | Mother only; <12 months; lactation included; manslaughter punishment |
| Infant Life Preservation Act 1929 | England | Child destruction; ≥28 weeks gestation; life imprisonment |
Key Exam Points
- India = infanticide is murder (S.302 IPC); no special leniency for mother
- England = infanticide Act 1938 reduces charge to manslaughter if mental balance disturbed
- Legal presumption in India = child is born dead (prosecution must prove live birth)
- If infanticide not proved → charged with concealment of birth (S.318 IPC)
- Foeticide = destruction before birth; Neonaticide = destruction in first month
(PC Dikshit Textbook of Forensic Medicine, p. 669-784; Parikh's Textbook of Medical Jurisprudence, p. 11299-11314)
Give in BNS Acts regarding infant deaths
Searching the Web
BNS 2023 Bharatiya Nyaya Sanhita sections infanticide concealment of birth abandonment child equivalent IPC 302 317 318
Finding Sources
Reading File
Here are the relevant BNS (Bharatiya Nyaya Sanhita), 2023 sections on infant deaths, along with their old IPC equivalents:
BNS 2023 - Acts Regarding Infant Deaths
(BNS came into force on 1st July 2024, replacing the IPC 1860)
Complete Section Map
| BNS Section | IPC Equivalent | Offence | Punishment |
|---|---|---|---|
| S. 86 | S. 312 | Causing miscarriage | Up to 3 yrs / 7 yrs if woman quick with child |
| S. 87 | S. 313 | Causing miscarriage without woman's consent | Life imprisonment or up to 10 yrs + fine |
| S. 88 | S. 314 | Death caused by act done with intent to cause miscarriage | Up to 10 yrs + fine; if woman dies - life imprisonment |
| S. 89 | S. 315 | Act done with intent to prevent child being born alive or to cause it to die after birth | Up to 10 yrs + fine |
| S. 90 | S. 316 | Causing death of quick unborn child by act amounting to culpable homicide | Up to 10 yrs + fine |
| S. 91 | S. 317 | Exposure and abandonment of child under 12 years | Up to 7 yrs + fine; if child dies = murder/culpable homicide |
| S. 92 | S. 318 | Concealment of birth by secret disposal of dead body | Up to 2 yrs + fine, or both |
| S. 103 | S. 302 | Murder (includes infanticide - killing newborn = murder) | Death or life imprisonment + fine |
Key Sections Explained
BNS S. 103 (= IPC S. 302) - Murder / Infanticide
- Infanticide in India = murder
- Same punishment: death or life imprisonment + fine
- Applies to both parents and any person
- Must prove child was born alive
- Legal presumption = child born dead (prosecution bears burden of proof)
BNS S. 89 (= IPC S. 315) - Preventing Live Birth
- Intentional act to prevent a child being born alive OR to cause it to die after birth
- Applies when child could have survived
- Up to 10 years + fine
BNS S. 91 (= IPC S. 317) - Exposure & Abandonment
"Whoever, being the father or mother of a child under the age of twelve years, or having the care of such child, shall expose or leave such child in any place with the intention of wholly abandoning such child..."
- Punishment: Up to 7 years + fine
- If child dies as consequence → tried for murder or culpable homicide
BNS S. 92 (= IPC S. 318) - Concealment of Birth
"Whoever by secretly burying or otherwise disposing of the dead body of a child whether such child die before, after, or during its birth, intentionally conceals or endeavours to conceal the birth..."
- Live birth need NOT be proved
- Sufficient that birth occurred + child was dead at time of concealment
- Punishment: Up to 2 years + fine, or both
- Charged when infanticide cannot be proved (lesser offence fallback)
Quick Reference Card
Infanticide (killing newborn) → BNS S. 103 (IPC 302) → Death / Life imprisonment
Prevent live birth → BNS S. 89 (IPC 315) → 10 yrs + fine
Abandoning child (<12 yrs) → BNS S. 91 (IPC 317) → 7 yrs + fine
Concealment of birth → BNS S. 92 (IPC 318) → 2 yrs + fine
Quick unborn child death → BNS S. 90 (IPC 316) → 10 yrs + fine
Exam tip: The BNS renumbered sections but the substance of law is unchanged. For forensic medicine MCQs post-July 2024, quote BNS section numbers. The most tested: S. 91 (abandonment), S. 92 (concealment), S. 103 (murder/infanticide).
Beveled wound
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Beveled Wound
Definition
A beveled wound is a sloping/angled defect in a flat bone (classically the skull) produced by a bullet passing through it. The wound is funnel-shaped (cone-shaped), with the funnel opening up in the direction the bullet is travelling - both at entry and exit.
It is the single most important feature for determining the direction of fire in gunshot injuries to the skull.
Mechanism of Beveling
"Beveling is produced when the unsupported diploe everts and fragments on the side where the bullet leaves, in contrast to the approach side where the rim of the defect is supported by the underlying bone."
The skull has three layers:
- Outer table (compact bone)
- Diploe (spongy middle layer)
- Inner table (compact bone)
When a bullet passes through, it punches a clean hole on the side it enters and shatters and bevels the bone on the side it exits - because the diploe is unsupported on the exit side.
Entrance Wound in Skull
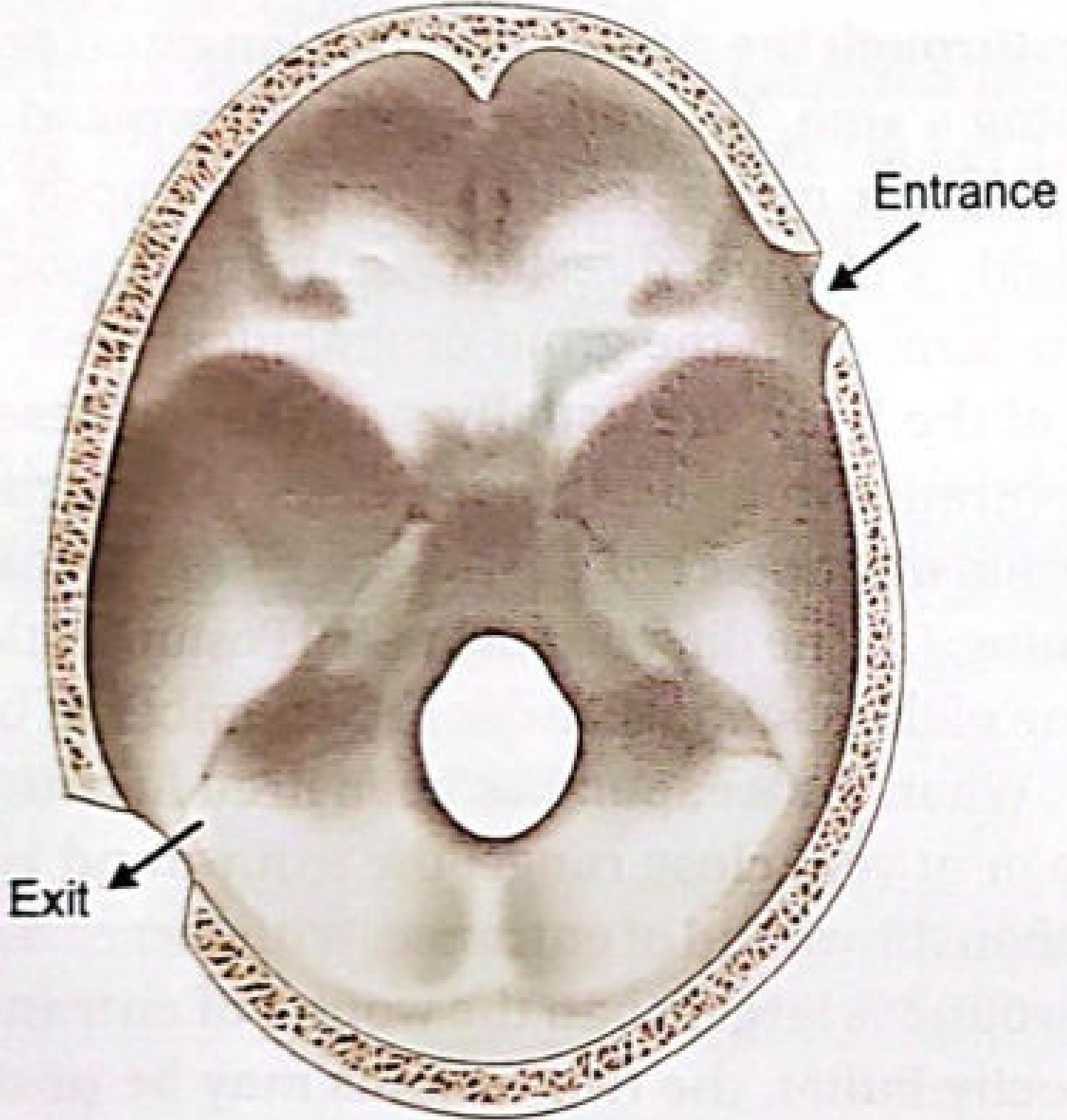
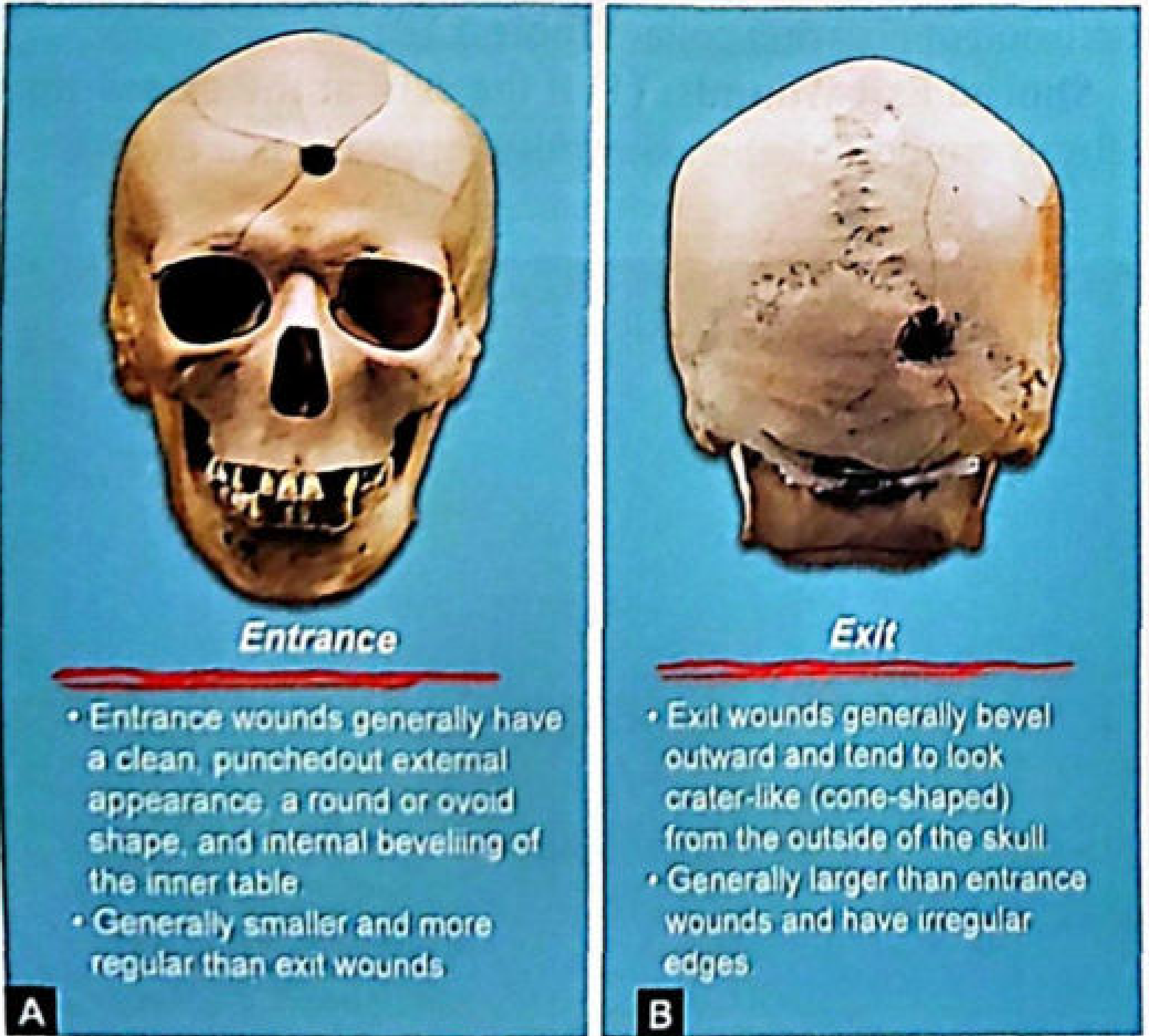
| Feature | Entrance Wound | Exit Wound |
|---|---|---|
| Outer table | Small, clean, punched-out hole | Beveled (sloped/cratered) outward |
| Inner table | Beveled inward (inward beveling) | Small, punched-out |
| Shape | Round/ovoid, clean-cut margins | Larger, irregular, crater-like |
| Size | Smaller | Larger (due to bullet deformity + tumbling) |
| Bevel direction | Inner table beveled = internal beveling | Outer table beveled = external beveling |
| Direction of cone | Cone opens inward (toward brain) | Cone opens outward (toward skin) |
Key rule:
- Entry = INner table beveled = INward beveling
- Exit = OUTer table beveled = OUTward beveling
- The tip of the cone always points toward the gun
Additional Features of Skull Gunshot Wounds
- Fissured/comminuted fractures radiate from the central hole (more with exit wound)
- Bone fragments from entry wound driven into cranial cavity → establish bullet track
- Exit wound larger due to deformity and tumbling of bullet after entering skull
- Asymmetry of beveling is useful in assessing the angle of fire
- Same beveling appearance seen in: sternum, pelvis, ribs, dentures, thumbnails
Determining Angle of Fire from Beveling
- Bullet at right angle → abrasion collar is circular and uniform
- Bullet at an angle → wound is round but marginal abrasion is oval/elliptical; wider on the side from which bullet approaches
- Direction of bullet = from wide to narrow side of abrasion
- Asymmetric beveling in skull = indicates oblique angle of fire
Puppe's Rule (Related)
When multiple bullets strike the skull:
- Fracture lines do not cross pre-existing fractures
- Cracks from a later shot are arrested by fractures already present from the first shot
- This determines the sequence of shots at autopsy
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 1741-1785; Brogdon's Forensic Radiology, p. 6041-6063)
Summary for Exams
| Entry | Exit | |
|---|---|---|
| Outer table | Clean hole (small) | Beveled OUT |
| Inner table | Beveled IN | Clean hole |
| Size | Smaller | Larger |
| Edges | Regular | Irregular |
| Cone tip points toward | Gun (outside) | Gun (inside) |
MCQ key: Internal/inward beveling = Entry wound; External/outward beveling = Exit woundMemory: "Entry wounds = INner table bevel = INward"
Medical negligence vs medical malpraxis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Medical Negligence vs Medical Malpraxis (Malpractice)
Are They the Same?
"Professional negligence, malpraxis or malpractice is defined as lack of reasonable care and skill or wilful negligence on the part of a medical practitioner in the treatment of a patient whereby the health or life of a patient is endangered."
(Parikh's Textbook of Medical Jurisprudence, p. 3698-3706)
In Indian forensic medicine textbooks, "medical negligence," "malpraxis," and "malpractice" are used synonymously - they are treated as the same concept under professional negligence. The textbook heading itself reads: "Professional (Medical) Negligence (Malpraxis)".
However, they carry subtle technical distinctions worth knowing:
Definitions
| Term | Definition |
|---|---|
| Medical Negligence | Omission to do something a reasonable person would do, OR doing something a reasonable person would not do - in a medical context |
| Medical Malpraxis / Malpractice | Lack of reasonable care and skill, OR wilful negligence by a medical practitioner in treatment of a patient, endangering health or life |
- Negligence is part of the law of torts (civil wrongs for which compensation is sought)
- "It is not mere neglect or carelessness - it is neglect or carelessness where there is a legal duty to take care and failure in that duty causes damage/injury"
The 4 Essential Elements (The "4 Ds")
For any negligence/malpractice claim to succeed, all four must be proved:
| # | Element | Meaning |
|---|---|---|
| 1 | Duty | Doctor owed a duty of care to the patient |
| 2 | Dereliction | Doctor breached/failed that standard of care |
| 3 | Direct causation | The breach directly and proximately caused the damage (no intervening cause) |
| 4 | Damage | Patient suffered actual, foreseeable harm |
Key rule: Even if the doctor is negligent, the patient cannot sue if no damage has occurred.
Types of Medical Negligence
1. Civil Negligence
- Patient sues doctor in Civil Court for compensation/damages
- Standard: simple absence of care and skill
- Burden of proof: patient proves by preponderance of evidence (more likely than not)
- Punishment: monetary damages only
What damages are assessed:
- Loss of present and future earning power
- Medical/surgical care costs
- Reduction in quality of life (loss of limb function, sensory loss)
- Pain and suffering (physical and mental)
- Loss of potency
- Aggravation of pre-existing condition
- Death
2. Criminal Negligence
- State prosecutes doctor in Criminal Court
- Standard: gross negligence - an extreme departure from the ordinary standard of care
- Burden of proof: guilt beyond reasonable doubt
- Punishment: imprisonment + fine (BNS S. 106 / IPC S. 304A)
Criminal negligence arises when:
- Doctor shows gross absence of skill or care resulting in serious injury/death
- Doctor performs an illegal act
- Gross lack of competence, gross inattention, gross recklessness, or wanton indifference to patient safety
- Gross negligence in selection and application of remedies
Conditions to satisfy:
- Indifference to an obvious risk of injury to health
- Actual foresight of risk but continuing same treatment
- Appreciation of risk but showing high degree of negligence in attempted avoidance
- Inattention to a serious risk beyond mere inadvertence
3. Contributory Negligence
- The patient's own conduct contributed to the harm
- If patient contributed to their injury → damages may be reduced or denied
4. Corporate Negligence
- Hospital/institution is held liable for negligent acts of its employees under the doctrine of Respondeat Superior (vicarious liability)
Civil vs Criminal Negligence - Comparison Table
| Trait | Civil Negligence | Criminal Negligence |
|---|---|---|
| Degree | Simple absence of care/skill | Gross negligence, recklessness |
| Litigation | Between two parties (patient vs doctor) | Between State and doctor |
| Court | Civil Court | Criminal Court |
| Evidence standard | Preponderance of evidence | Beyond reasonable doubt |
| Consent as defense | Yes - good defense | No - NOT a defense |
| Punishment | Pay damages (monetary) | Imprisonment + fine |
| Violation of law | No specific law need be violated | Must have violated a specific criminal law |
| Conduct compared to | Standard professional conduct | No single test |
Special Doctrines
Res Ipsa Loquitur ("The Thing Speaks for Itself")
Applied when the error is so self-evident that the doctor must prove innocence rather than the patient proving guilt. Three conditions required:
- Nature of injury suggests negligence by common knowledge
- Patient did not contribute to the injury
- Doctor was in exclusive control of the instrumentalities
Classic examples: foreign body left inside patient after surgery, burns from heating pads, wrong-side operation.
(Parikh's Textbook of Medical Jurisprudence, p. 3767-3802)
Bolam Test (Standard of Care)
"The degree of skill that a practitioner should bring to treatment is the average degree of skill possessed by his professional colleagues of the same standing."
- Error in diagnosis or treatment is NOT negligence if proper care and skill was exercised
- A specialist is held to a higher standard than a general practitioner
- An error of judgment ≠ negligence (as long as reasonable care was taken)
Defenses Against Negligence Claims
- Error of judgment (not the same as negligence)
- Therapeutic misadventure (unforeseeable complication)
- Unforeseeable complication
- Contributory negligence by the patient
- Consent (valid defense in civil; NOT in criminal)
- Good Samaritan protection
- Res judicata (matter already decided)
Note for exams: Contributory negligence is a defense against civil negligence claims but not for criminal negligence.
(The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 4137-4776)
This is a shared conversation. Sign in to Orris to start your own chat.