Hypertensive disorders in pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertensive disorders" AND pregnancy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full detailed response.
Hypertensive Disorders of Pregnancy (HDP)
Overview
Hypertensive disorders complicate approximately 5-8% of all pregnancies (up to 85 per 1000 deliveries in the United States) and represent one of the leading causes of maternal and perinatal morbidity and mortality worldwide. They encompass a spectrum ranging from mild gestational hypertension to life-threatening eclampsia and HELLP syndrome.
Classification (ACOG)
The ACOG Practice Bulletin No. 222 defines four main categories:
| Category | Definition |
|---|---|
| Gestational Hypertension | New-onset BP ≥140/90 mmHg after 20 weeks, without proteinuria or end-organ damage; resolves postpartum |
| Preeclampsia | Gestational hypertension + proteinuria (≥300 mg/24h, protein:creatinine ≥0.3, or dipstick 2+) OR new end-organ damage |
| Chronic Hypertension | HTN diagnosed before pregnancy or before 20 weeks, or persisting postpartum |
| Chronic HTN with Superimposed Preeclampsia | Preeclampsia developing in a woman with pre-existing chronic hypertension |
Note: Eclampsia = Preeclampsia + new-onset tonic-clonic, focal, or multifocal seizures in the absence of other causes.
Onset subclassification:
- Early-onset preeclampsia: <34 weeks (more severe, higher maternal/fetal risk)
- Late-onset preeclampsia: ≥34 weeks (more common)
Epidemiology and Risk Factors
- Gestational hypertension: 6-17% of nulliparous, 2-4% of parous women
- Preeclampsia: 5-8% of all pregnancies
- Eclampsia: ~1 in 2000-3000 deliveries in high-resource settings
Major risk factors (Creasy & Resnik's Maternal-Fetal Medicine, Table 45.2):
- Nulliparity (highest population-attributable fraction: 32.3%)
- Prior preeclampsia (8-fold increased risk)
- Chronic hypertension (25% risk of superimposed preeclampsia)
- Antiphospholipid syndrome
- Pregestational diabetes mellitus (20% overall; up to 70% with White's class F/R)
- Renal disease
- Connective tissue disorders (SLE)
- Multifetal gestation
- IVF conception
- Extremes of maternal age
- Non-Hispanic Black race (related more to severity than incidence)
- Obesity, family history of preeclampsia
Pathophysiology
The central mechanism is a two-stage model:
Stage 1 - Defective Placentation
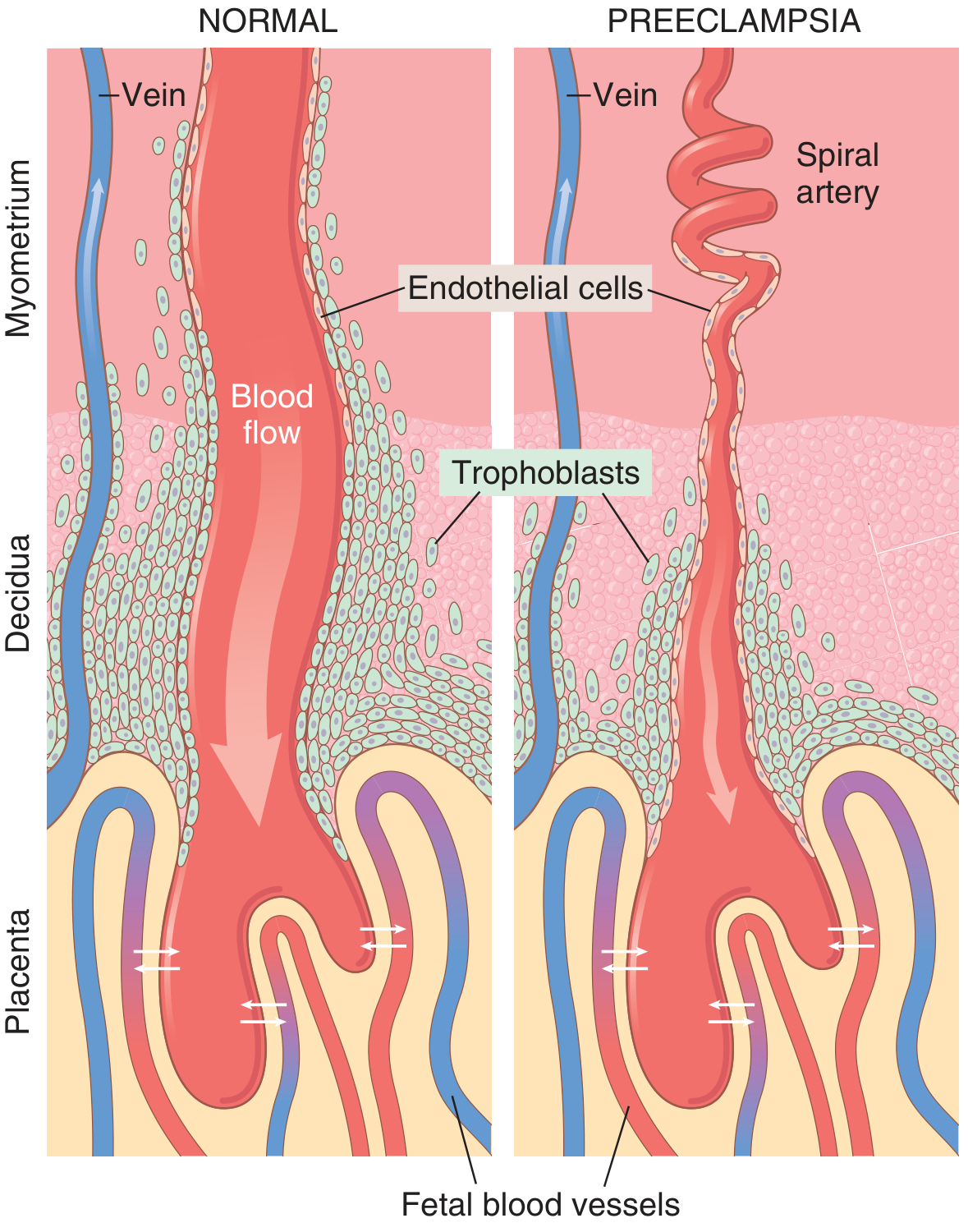
In normal pregnancy, trophoblasts invade the spiral arteries of the uterine endometrium, remodeling them into wide, low-resistance vascular sinusoids. In preeclampsia, this process is impaired - the muscloelastic walls are retained, channels remain narrow, and uteroplacental blood flow is reduced, leading to placental hypoxia.
Stage 2 - Endothelial Dysfunction
Placental ischemia triggers release of circulating factors into the maternal bloodstream:
- sFlt-1 (soluble fms-like tyrosine kinase-1) - antagonizes VEGF
- Soluble endoglin (sEng) - antagonizes TGF-β
- Inflammatory cytokines (TNF-α, IL-6)
These antiangiogenic factors cause systemic maternal endothelial dysfunction, leading to:
| Consequence | Mechanism |
|---|---|
| Hypertension | Reduced endothelial PGI₂/PGE₂ (vasodilators) + increased TXA₂ (vasoconstrictor); increased SVR |
| Proteinuria / renal injury | Glomerular endotheliosis; decreased GFR, decreased renal blood flow |
| Coagulopathy/HELLP | Endothelial activation → platelet consumption, microangiopathic hemolysis |
| Fetal growth restriction | Chronic uteroplacental hypoperfusion |
| Seizures (eclampsia) | Cerebral vasospasm, blood-brain barrier disruption, PRES (posterior reversible encephalopathy syndrome) |
| Hepatic injury | Periportal fibrin deposition; elevated AST/ALT; risk of subcapsular hematoma/rupture |
| Pulmonary edema | Increased afterload, decreased oncotic pressure, endothelial permeability |
Vascular reactivity: Preeclamptic women show exaggerated sensitivity to all endogenous pressors - angiotensin II, norepinephrine, epinephrine, and vasopressin - a finding detectable weeks before clinical hypertension develops.
Diagnosis
Preeclampsia Without Severe Features
- BP ≥140/90 mmHg on two occasions ≥4 hours apart, at or after 20 weeks
- PLUS: proteinuria ≥300 mg/24h (or protein:creatinine ≥0.3, or dipstick 2+)
- OR: any of the following end-organ manifestations even without proteinuria:
- Thrombocytopenia (<100,000/μL)
- Renal insufficiency (creatinine >1.1 mg/dL or doubling of baseline)
- Impaired liver function (AST/ALT ≥2× upper limit of normal)
- Pulmonary edema
- New-onset headache unresponsive to analgesics
- Visual disturbances
Severe Features (Any One Qualifies)
Per ACOG (also from Goldman-Cecil Medicine, Table 221-7):
| Severe Feature | Threshold |
|---|---|
| Severe hypertension | SBP ≥160 or DBP ≥110 mmHg on 2 occasions ≥4 h apart |
| Thrombocytopenia | Platelets <100,000/μL |
| Elevated liver enzymes | ≥2× upper limit of normal |
| Severe RUQ/epigastric pain | Unresponsive to medications |
| Renal insufficiency | Creatinine >1.1 mg/dL or doubling of baseline |
| Pulmonary edema | - |
| New-onset headache | Not relieved by analgesics |
| Visual disturbances | - |
HELLP Syndrome
A severe variant of preeclampsia occurring in ~10% of severe cases:
- H - Hemolysis (microangiopathic hemolytic anemia)
- EL - Elevated Liver enzymes
- LP - Low Platelets
Morphological / Histological Findings (Robbins & Kumar Basic Pathology)
Placenta:
- Multiple infarcts (far more numerous than in normal pregnancy)
- Retroplacental hemorrhage
- Ischemic changes: increased syncytial knot formation
- Acute atherosis: fibrinoid necrosis of decidual vessels + lipid-laden macrophages
Kidney:
- Glomerular endotheliosis - the classic lesion: swelling of glomerular endothelial cells, luminal obliteration, subendothelial protein deposits
- Decreased GFR, decreased renal blood flow
Brain (Eclampsia):
- Posterior reversible encephalopathy (PRES) - T2-weighted MRI shows bilateral signal intensity in subcortical white matter of occipital/parietal regions
- Hemorrhage, ring hemorrhages, petechiae
Management
Antihypertensive Treatment Algorithm
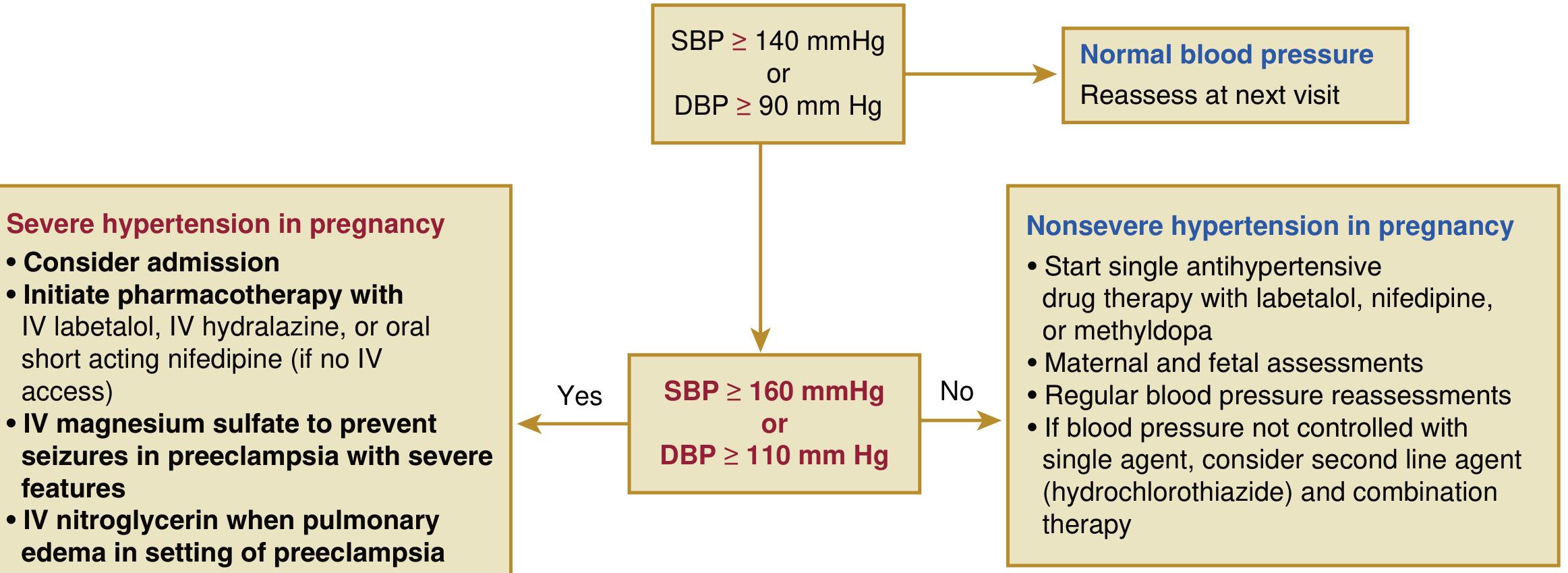
Urgent Management of Severe Hypertension (BP ≥160/110 mmHg)
Per Goldman-Cecil Medicine (Table 221-6):
| Route | Drug | Dose |
|---|---|---|
| Oral | Nifedipine IR | 10-20 mg initially; repeat in 20 min; then 10-20 mg q2-6h (max 180 mg/day) |
| IV | Labetalol (preferred) | 10-20 mg IV bolus, then 1-2 mg/min infusion (or 20-80 mg q10-30 min) to max 300 mg |
| IV | Hydralazine | 5 mg initially, then 0.5-10 mg/hr (or 5-10 mg q20-40 min) to max 20 mg |
For pulmonary edema in the setting of preeclampsia: IV nitroglycerin.
Nonsevere Hypertension (140-159/90-109 mmHg)
- First-line oral agents: labetalol, nifedipine (extended release), or methyldopa
- If uncontrolled on monotherapy: add hydrochlorothiazide
- Regular maternal and fetal monitoring
Drugs to AVOID in pregnancy:
- ACE inhibitors and ARBs (fetotoxic - renal dysgenesis, oligohydramnios, fetal demise)
Seizure Prophylaxis / Eclampsia Management
Magnesium sulfate is the drug of choice:
- Loading dose: 4-6 g IV over 15-20 minutes
- Maintenance: 2 g/hour infusion
- Mechanism: cerebrovascular vasodilation, membrane stabilization, NMDA receptor antagonism
- Monitoring: urine output, respiratory rate, reflexes; antidote is calcium gluconate (1 g IV)
- Cleared renally - use caution in renal impairment
If seizures persist despite MgSO₄: give additional 2-g loading dose. Avoid respiratory depressants.
Delivery - The Only Cure
- Definitive treatment is delivery of the fetus and placenta
- Preeclampsia without severe features: delivery at 37 weeks
- Preeclampsia with severe features: delivery at 34 weeks (or sooner if deterioration)
- Emergent cesarean is NOT recommended solely for an eclamptic seizure - fetal compromise often resolves with maternal supportive care post-seizure
Postpartum Management
- Preeclampsia/eclampsia can present up to 6 weeks postpartum
- Continue seizure prophylaxis and antihypertensive therapy postpartum
- Most women develop pulmonary edema after delivery - careful fluid management is key
- Volume expansion (e.g., albumin) not routinely recommended
- Furosemide 20 mg IV for postpartum pulmonary edema
Prevention
Evidence-based interventions for high-risk women:
- Low-dose aspirin (81-150 mg/day, starting before 16 weeks): reduces risk of preeclampsia by ~20-30% in high-risk women (USPSTF recommendation)
- Calcium supplementation (1.5-2 g/day): beneficial in populations with low dietary calcium intake
- Optimization of pre-existing conditions before conception (HTN, diabetes, lupus, renal disease)
Fetal and Perinatal Complications
- Fetal growth restriction (FGR) / small-for-gestational-age
- Placental abruption
- Preterm birth (iatrogenic or spontaneous)
- Oligohydramnios
- Perinatal asphyxia
- Perinatal death
Long-Term Maternal Consequences
Pregnancy is described as a "stress test" that reveals subclinical vascular risk (Creasy & Resnik, Fig. 72.1). Women with a history of preeclampsia face substantially elevated lifetime cardiovascular risk:
| Outcome | Relative Risk |
|---|---|
| Hypertension (2-7 yrs postpartum) | 36.5% affected vs. 17% controls |
| Chronic HTN after early-onset preeclampsia | Up to 50% |
| CVD (CAD, stroke, heart failure) within 5 years | ~2× increased |
| Risk with early-onset preeclampsia (<34 wks) | Up to 8× |
The AHA officially recognizes a history of hypertension in pregnancy as an established risk factor for cardiovascular disease. Long-term screening for hypertension, renal function, and cardiovascular risk factors is recommended for all women with prior HDP.
A 2026 systematic review in AJOG (PMID 41421750) addresses postpartum management strategies, and a 2025 network meta-analysis in AJOG (PMID 40216176) evaluated relative efficacy of oral antihypertensives during pregnancy.
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapter 45
- Goldman-Cecil Medicine, Chapter 221, Table 221-6/7
- Robbins & Kumar Basic Pathology, Chapter 7
- Braunwald's Heart Disease, 12e, Chapter 92
- Guyton & Hall Textbook of Medical Physiology, Chapter 83
- ACOG Practice Bulletin No. 222 (2020): Gestational Hypertension and Preeclampsia
This is a shared conversation. Sign in to Orris to start your own chat.