Development of uterus diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the key diagrams and text needed for a comprehensive answer. Here is the full educational breakdown:
Development of the Uterus
1. Embryological Origin
The uterus develops from the paramesonephric (Müllerian) ducts - a pair of longitudinal tubes arising from the coelomic epithelium lateral to the mesonephros, appearing around weeks 5-6 of embryonic development.
In the female embryo, the absence of anti-Müllerian hormone (AMH/MIS) - which would otherwise cause Müllerian duct regression - allows the paramesonephric ducts to persist and develop. This occurs in the presence of estrogen and the absence of testosterone.
2. Three-Part Structure of Each Paramesonephric Duct
Each paramesonephric duct has three recognizable segments:
- Cranial vertical portion - opens into the abdominal cavity → becomes the uterine (fallopian) tube
- Horizontal part - crosses the mesonephric duct
- Caudal vertical part - fuses with its partner from the opposite side → forms the uterine canal
3. Diagram A: Early Development - Müllerian and Mesonephric Ducts
This diagram shows the early fetal female reproductive system, with the Müllerian duct (pink/red) running alongside the mesonephros (blue), both converging at the urogenital sinus to form the Müllerian tubercle (the precursor to the uterovaginal canal).
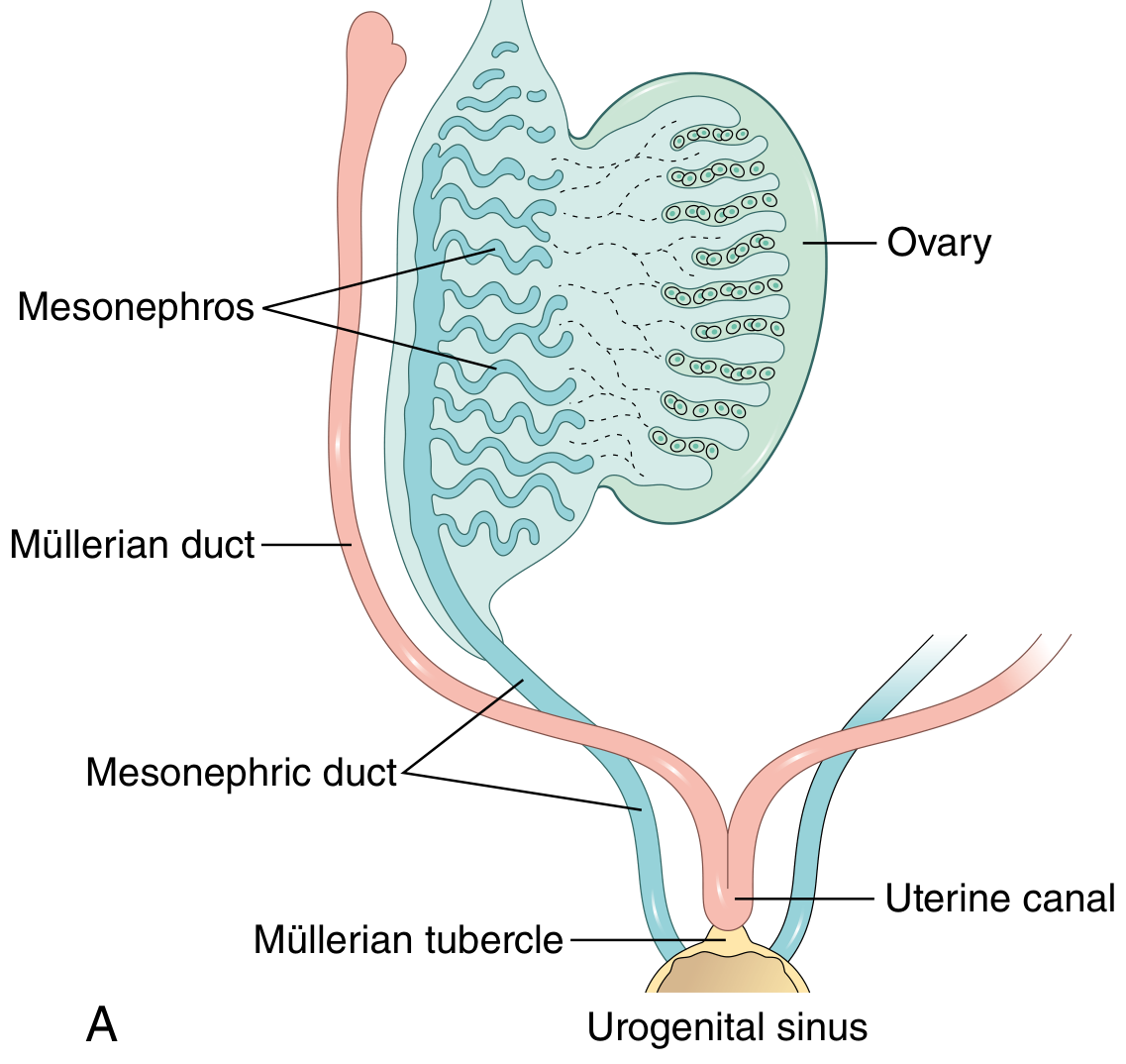
Fig. 22.1A - Robbins & Kumar Pathologic Basis of Disease: Early development showing mesonephric (blue) and Müllerian (red) ducts merging at the urogenital sinus.
4. Diagram B: Transverse Sections Showing Duct Fusion
Three cross-sectional stages show how the paramesonephric ducts approach each other from the lateral urogenital ridges, fuse in the midline, and form the broad ligament of the uterus as a transverse pelvic fold. The gonads (ovaries) come to rest at the posterior surface of this fold.
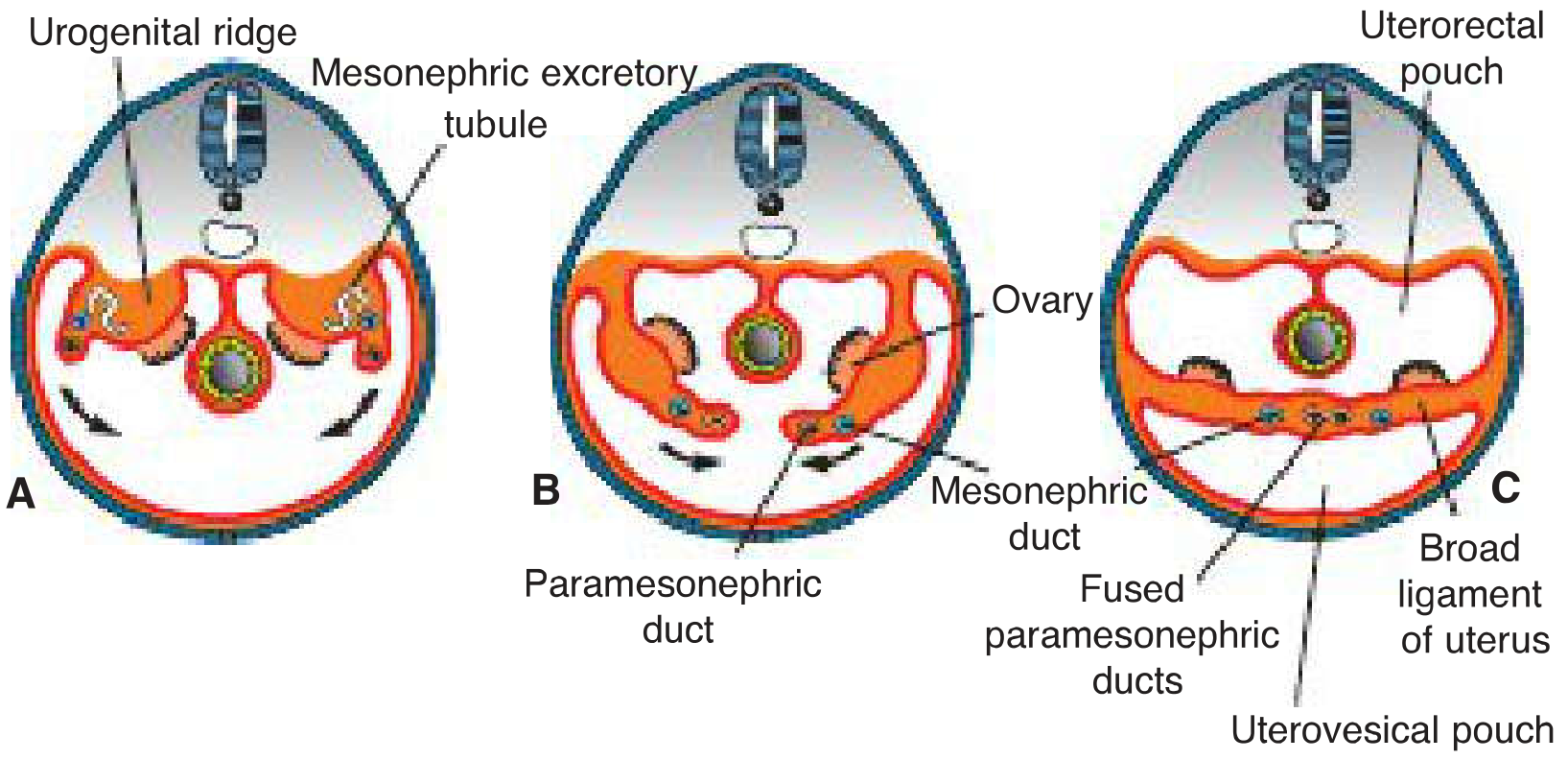
Fig. 16.27 - Langman's Medical Embryology: (A) Urogenital ridges separate; (B) Paramesonephric ducts approach midline with ovary visible; (C) Fused paramesonephric ducts form the uterus, with broad ligament, uterovesical pouch, and uterorectal pouch established.
5. Diagram C: Vagina and Uterus Formation from Sinovaginal Bulbs
This diagram shows the sequential canalization of the fused paramesonephric ducts and the contribution of the sinovaginal bulbs (from the urogenital sinus) to vaginal formation.
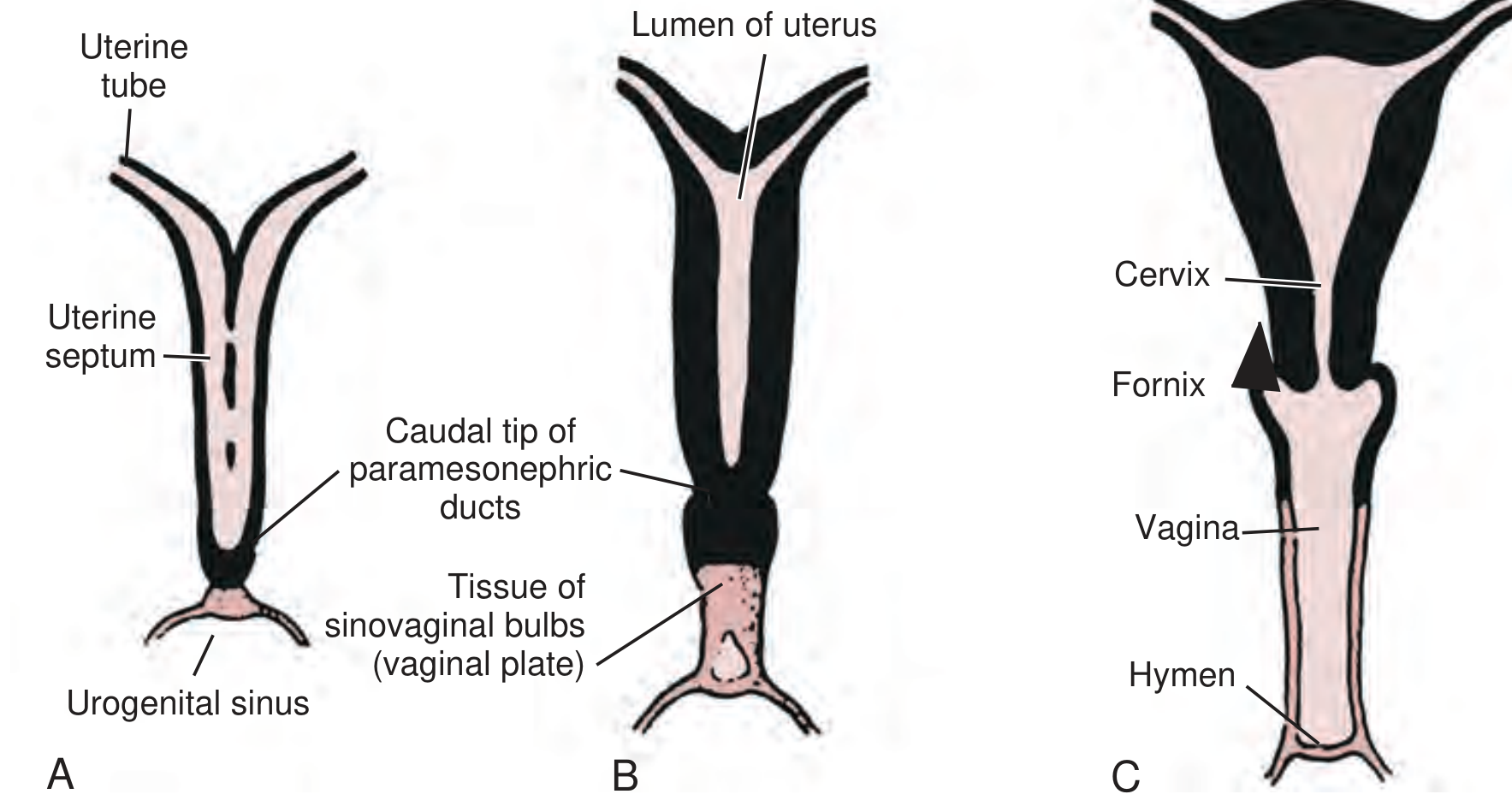
Fig. 47.1 - Campbell Walsh Wein Urology: (A) Uterine septum still present, sinovaginal bulb tissue (vaginal plate) below; (B) Canalization progressing, uterine lumen opening; (C) Fully formed uterus with cervix, fornix, vagina, and hymen.
6. Diagram D: Male vs. Female Gonad and Genital Development (Comparative)
This side-by-side comparison shows how identical indifferent structures differentiate under hormonal control:
- In males: SRY protein → Sertoli cells → AMH causes Müllerian regression; mesonephric ducts persist
- In females: No SRY/AMH → paramesonephric ducts develop into fallopian tubes, uterus, and upper vagina; mesonephric ducts degenerate (leaving only Gartner duct cysts as remnants)
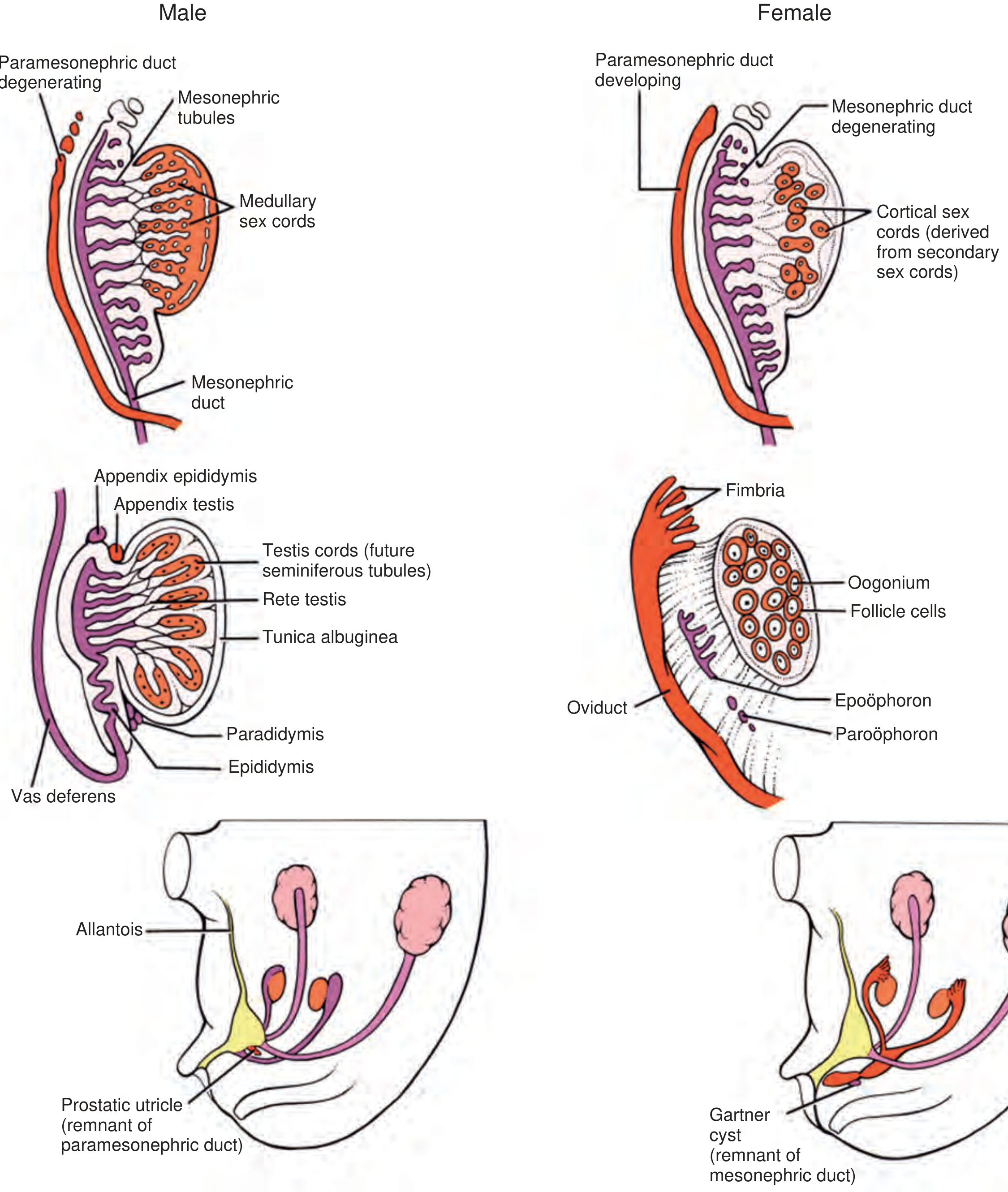
Fig. 20.24 - Campbell Walsh Wein Urology: Male (left) vs. female (right) development from indifferent gonads through differentiated genital structures.
7. Diagram E: Mature Female Genital Tract (At Birth)
By birth, the Müllerian ducts have fused to form the fallopian tubes, uterus, and endocervix. Mesonephric duct remnants may persist as Gartner duct cysts in the anterolateral vaginal wall and as epoophoron/paroophoron in the adnexa.
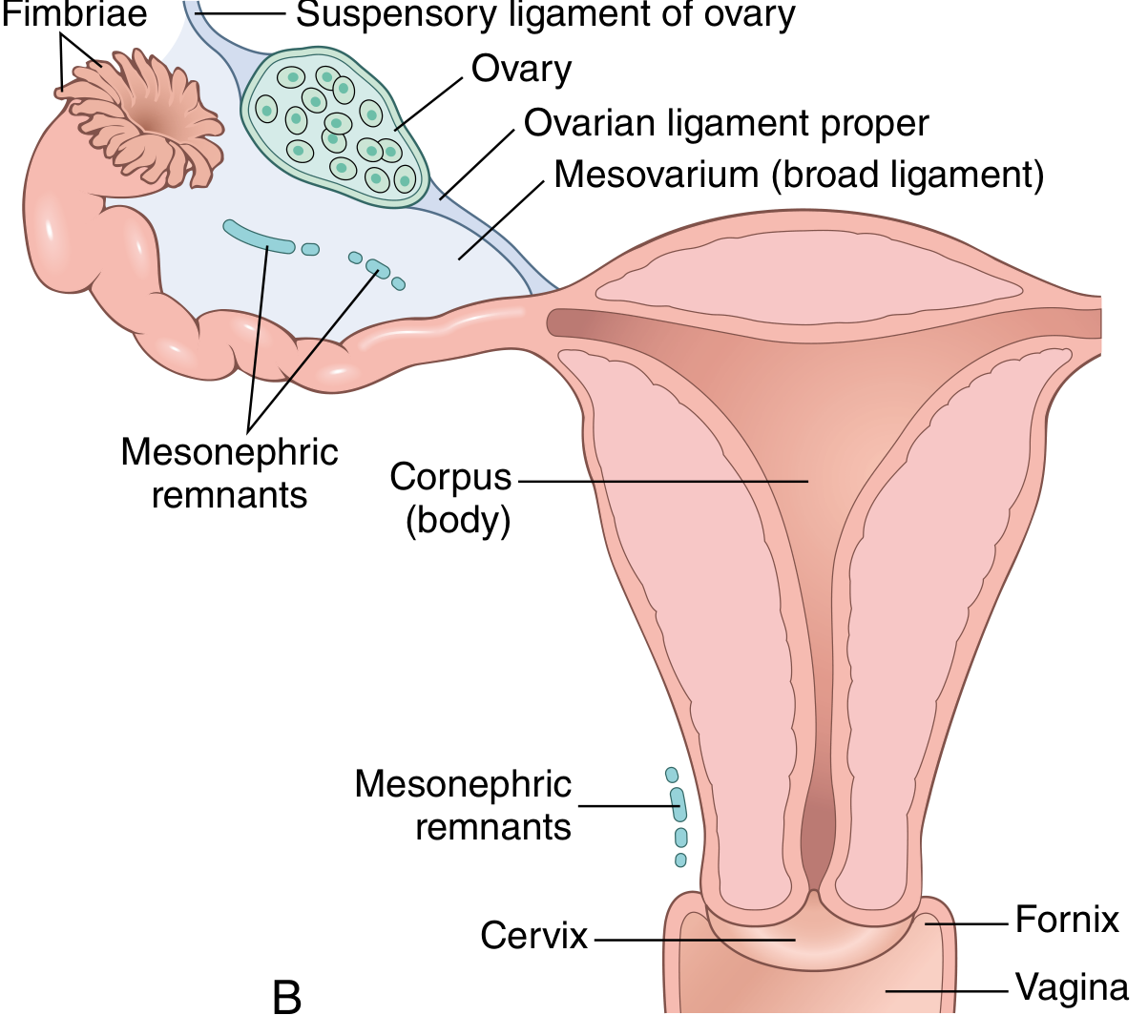
Fig. 22.1B - Robbins & Kumar Pathologic Basis of Disease: Final anatomy of the female genital tract with labelled structures including corpus, cervix, fimbriae, ovarian ligament, mesovarium (broad ligament), mesonephric remnants, fornix, and vagina.
8. Key Developmental Summary Table
| Structure | Embryological Origin |
|---|---|
| Fallopian tubes | Cranial + horizontal parts of paramesonephric duct |
| Uterus (corpus + cervix) | Fused caudal parts of paramesonephric ducts |
| Upper vagina (~upper 4/5) | Fused paramesonephric ducts + sinovaginal bulbs |
| Lower vagina (~lower 1/5) | Urogenital sinus (sinovaginal bulbs → vaginal plate) |
| Ovary | Cortical sex cords of indifferent gonad |
| Gartner duct cysts | Remnant of mesonephric (Wolffian) duct |
| Appendix vesiculosa | Remnant of cranial mesonephric tubules |
9. Congenital Anomalies from Developmental Failure
Errors in paramesonephric duct development (around week 8) produce a spectrum of uterine anomalies:
| Anomaly | Cause |
|---|---|
| Uterus didelphys (double uterus) | Failure of fusion of caudal paramesonephric ducts |
| Bicornuate uterus | Incomplete fusion - only superior body duplicated |
| Unicornuate uterus | One paramesonephric duct fails to develop |
| Septate uterus | Incomplete resorption of the uterine septum after fusion |
| Vaginal atresia / absence | Failure of sinovaginal bulbs to develop or canalize |
| Imperforate hymen | Failure of inferior vaginal plate to perforate |
Sources:
- Robbins & Kumar Pathologic Basis of Disease, Fig. 22.1
- Langman's Medical Embryology, Fig. 16.27 - paramesonephric duct fusion
- Campbell Walsh Wein Urology, Fig. 20.24 - male vs. female genital development
- The Developing Human: Clinically Oriented Embryology - uterine anatomy and menstrual cycle
This is a shared conversation. Sign in to Orris to start your own chat.