Teach me in simple way about enteric fever (typhoid) Epidemiology Pathogenesis Lab diagnosis Widal test Drug resistance prophylaxis Vaccine Microbiology For microbiology uni exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have very comprehensive content from Harrison's (2025) and Jawetz Medical Microbiology to write a thorough, exam-ready guide. Let me compile everything now.
🦠 Enteric Fever (Typhoid) - Complete Microbiology Exam Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Jawetz Melnick & Adelberg's Medical Microbiology 28E, Park's Textbook of Preventive & Social Medicine
1. THE ORGANISM (Microbiology of Salmonella Typhi)
Classification:
- Family: Enterobacteriaceae
- Gram-negative, short rod (bacillus)
- Non-lactose fermenter
- Motile (peritrichous flagella)
- Facultative anaerobe
- Produces H₂S gas
- Does NOT form spores or capsule (except Vi antigen = virulence capsular antigen)
Key Antigens (Kauffmann-White scheme):
| Antigen | Type | Significance |
|---|---|---|
| O antigen | Somatic (cell wall LPS) | Serogroup D for S. Typhi; rises first in infection (day 6-8) |
| H antigen | Flagellar (phase 1 = d) | Species-specific; rises after O (day 10-12) |
| Vi antigen | Capsular polysaccharide | Virulence factor; used in vaccines; may block O agglutination |
Culture characteristics:
- On MacConkey / EMB agar: pale/colorless colonies (non-lactose fermenter)
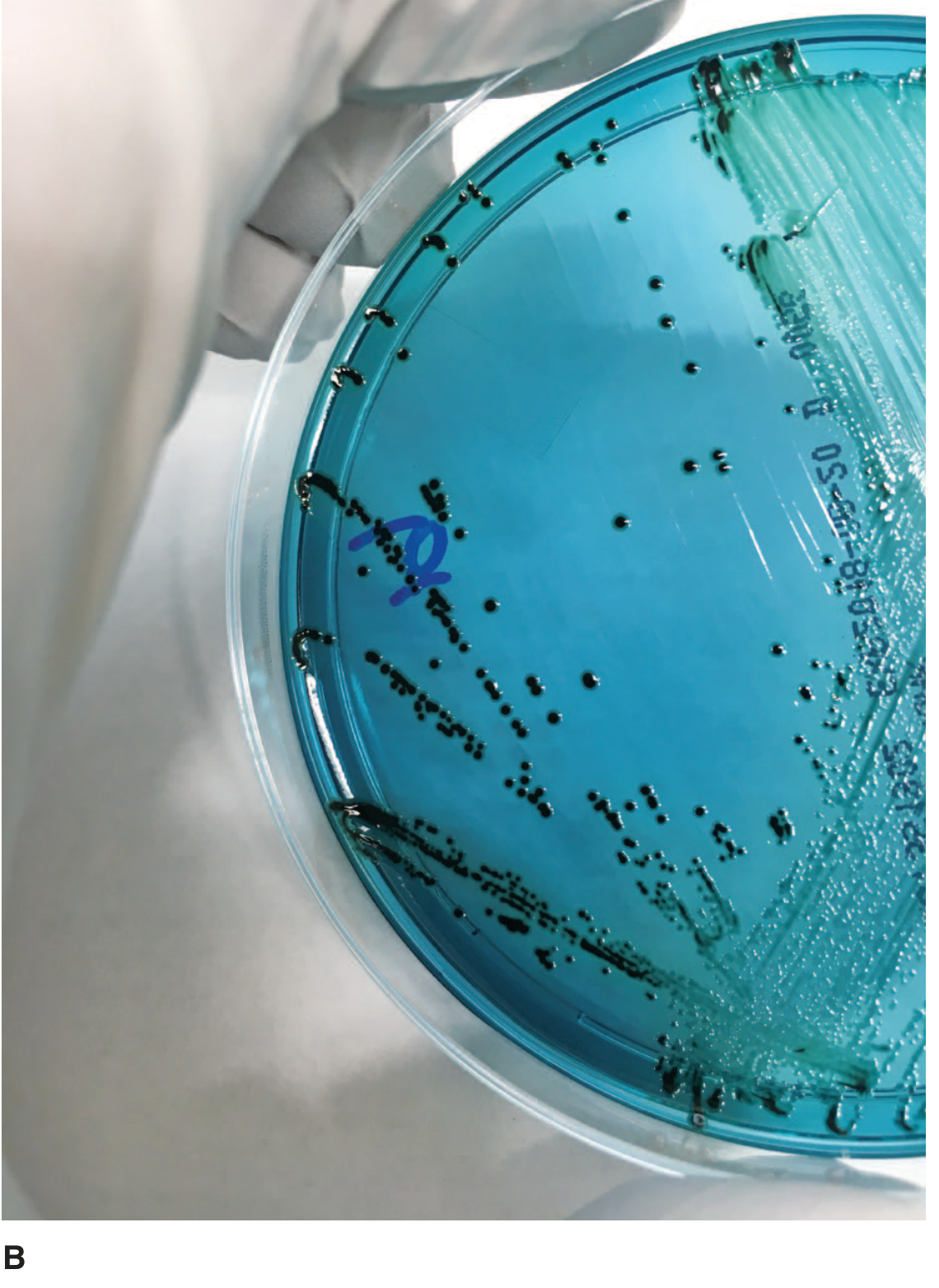
- On Bismuth sulfite agar: black colonies (H₂S production)
- On Salmonella-Shigella (SS) agar / HE agar / XLD agar: selective media
- On TSI (Triple Sugar Iron) slant: K/A, Gas, H₂S positive (ferments glucose only, not lactose or sucrose)
- Enrichment broth: Selenite F or Tetrathionate broth (inhibits normal flora, allows Salmonella to multiply)
2. EPIDEMIOLOGY
Global burden:
- ~9.2-21 million cases of typhoid fever per year worldwide
- ~5 million cases of paratyphoid fever per year
- 110,000-280,000 deaths annually
- Highest incidence: Indian subcontinent (India, Pakistan, Bangladesh, Nepal), Eastern Mediterranean, Africa - exceeding 1,000 cases per 100,000 children in some urban areas
- In developed countries (USA, Western Europe), enteric fever is rare and mostly travel-associated
Transmission:
- Fecal-oral route - the ONLY route
- S. Typhi and S. Paratyphi are strictly human pathogens (no animal reservoir - unlike non-typhoidal Salmonella)
- Sources:
- Fecally contaminated drinking water or ice (causes explosive epidemics)
- Contaminated food from chronic carriers (most important ongoing source)
- Street food, raw fruits/vegetables from sewage-fertilized fields
- Sexual transmission (male-to-male, documented)
- Health care workers from infected patients/cultures
Risk factors:
- Poor sanitation, mixing of drinking water with sewage
- No handwashing, limited toilet access
- Young children and adolescents in endemic areas
- Prior H. pylori infection (reduces gastric acidity = lower barrier)
- Travel to endemic regions
Carriers:
- 3% of typhoid survivors become permanent (chronic) carriers
- Organisms persist in the gallbladder and biliary tract (especially if gallstones present)
- Convalescent carriers shed organisms in stool/urine for weeks after recovery
- Carriers working as food handlers = major source of outbreaks
3. PATHOGENESIS
Step-by-step (exam favorite):
Ingestion of S. Typhi (inoculum ~10⁵ organisms)
↓
Survive gastric acid → reach small intestine
↓
Penetrate intestinal epithelium via M-CELLS overlying Peyer's patches
(M-cells in ileum = specialized sampling cells of gut-associated lymphoid tissue)
↓
Enter intestinal lymphatics → Peyer's patches multiply → local hyperplasia
↓
PRIMARY BACTEREMIA (1st week) - spreads to liver, spleen, bone marrow
↓
Bacteria multiply intracellularly within macrophages (reticuloendothelial system)
↓
SECONDARY BACTEREMIA (2nd week) - high fever plateau, systemic illness
↓
Re-seeding of intestine via bile from gallbladder
→ Necrosis of Peyer's patches → ulceration
Key pathological lesions:
- Hyperplasia then necrosis of Peyer's patches (ileum) - hallmark
- Enlarged mesenteric lymph nodes
- Hepatitis + focal necrosis of liver
- Splenomegaly
- Inflammation of gallbladder (organisms persist here)
- Rose spots = bacterial emboli in dermal capillaries
Why bacteremia is sustained:
- S. Typhi survives inside macrophages (intracellular pathogen) - resists killing
- Vi antigen inhibits complement activation and phagocytosis
4. CLINICAL FEATURES
Incubation period: 10-14 days (range 5-21 days, depending on inoculum size)
Classic stepwise fever progression (3 weeks):
| Week | Features |
|---|---|
| Week 1 | Gradual onset fever, headache, malaise, dry cough, constipation, relative bradycardia |
| Week 2 | High plateau fever (39-40°C), rose spots appear, hepatosplenomegaly, delirium |
| Week 3 | Complications may appear - intestinal hemorrhage, perforation |
| Week 4 | Gradual defervescence if untreated (or death in severe cases) |
Classic signs:
- Relative bradycardia (Faget's sign) = pulse lower than expected for the fever temperature
- Rose spots: faint, salmon-colored, blanching maculopapular rash on trunk/chest; 2-4mm; appear in ~30% of patients; disappear in 3-4 days
- Coated tongue (51-56%)
- Splenomegaly + hepatomegaly
- Dicrotic pulse
Important labs:
- Leukopenia (WBC normal or low) - NOT elevated as in typical bacterial sepsis - classic exam point!
- Elevated liver enzymes
Complications:
- Intestinal hemorrhage (sudden temperature drop + shock + blood in stool)
- Intestinal perforation (3rd week - most dangerous)
- Pneumonia, myocarditis, cholecystitis, nephritis, osteomyelitis, typhoid psychosis
Mortality: 1-4% with treatment; up to 10-30% if untreated
5. LABORATORY DIAGNOSIS
Summary Table
| Test | Best Timing | Sensitivity | Notes |
|---|---|---|---|
| Blood culture | Week 1-2 | 60-80% | Gold standard; positive in first 1-2 weeks |
| Bone marrow culture | Any time | >90% | Most sensitive; remains positive even after antibiotics |
| Stool culture | Week 2-3 | ~50% | Positive from 2nd week onward |
| Urine culture | Week 3 | Low | Less reliable |
| Widal test | Week 2+ | Moderate | Serological test; see below |
Blood culture = MAINSTAY of diagnosis (most important clinically)
Bone marrow culture = GOLD STANDARD (highest sensitivity ~90%, not affected by prior antibiotics)
Steps in bacteriological culture:
- Sample (blood, stool, urine, bone marrow)
- Inoculate into enrichment broth (selenite F / tetrathionate) for stool
- Subculture on differential media (MacConkey, EMB, bismuth sulfite)
- Subculture on selective media (SS agar, HE agar, XLD agar)
- Identify suspect colonies by biochemical reactions (TSI, urease, oxidase)
- Confirm by slide agglutination with specific antisera
6. WIDAL TEST (Tube Dilution Agglutination Test)
What it is:
A serological test that detects agglutinating antibodies (IgM and IgG) against the O and H antigens of S. Typhi in the patient's serum.
Principle:
Patient serum + known S. Typhi O and H antigens → look for agglutination
Antibody appearance timing:
- O antibodies: appear day 6-8 after onset
- H antibodies: appear day 10-12 after onset
- Serum agglutinins rise sharply during weeks 2-3 of infection
Interpretation:
- Need 2 serum samples at 7-10 day intervals to show a rising titer (4-fold rise is significant)
- Single significant titers (used in endemic areas):
- O agglutinin ≥ 1:160 = significant
- H agglutinin ≥ 1:160 = significant
- A rising titer is more meaningful than a single titer
Limitations (very high-yield exam content):
- False positives caused by:
- Cross-reaction with other Salmonella serotypes sharing O/H antigens
- Cross-reacting epitopes with other Enterobacteriaceae
- Malaria, typhus, bacteremia, liver cirrhosis, immunological conditions
- Previous vaccination
- False negatives caused by:
- Prior antibiotic therapy (blunts antibody response)
- Early disease (too early for antibody rise)
- Immunocompromised patients
- Up to 30% of culture-proven typhoid cases can be Widal-negative!
- Difficult to interpret in endemic areas (background titers are high)
- CDC does NOT recommend Widal test for diagnosis of acute typhoid
Newer alternatives to Widal:
- IDL Tubex® test: detects IgM antibodies against O9 antigen; results in minutes
- Typhidot®: detects IgM + IgG against 50kD antigen of S. Typhi; takes 3 hours
- Typhidot-M®: detects IgM only (more specific for acute infection)
- Dipstick test: detects S. Typhi-specific IgM antibodies against LPS antigen
- PCR/NAAT: direct detection; still being evaluated for routine use
7. DRUG RESISTANCE
History of resistance:
| Era | Drugs | Status |
|---|---|---|
| Pre-1990s | Chloramphenicol, Ampicillin, TMP-SMX | First-line drugs |
| 1980s-90s | All three above | MDR S. Typhi emerged (plasmid-encoded resistance) - emerged in China, SE Asia |
| 1990s-2000s | Fluoroquinolones (ciprofloxacin) | Widely used for MDR typhoid |
| 2000s-present | Fluoroquinolones | DSC (decreased susceptibility to ciprofloxacin) and full resistance emerged on Indian subcontinent |
| 2016-present | Ceftriaxone + fluoroquinolones | XDR S. Typhi (extensively drug-resistant) - Pakistan; resistant to all 1st line + fluoroquinolones + 3rd-gen cephalosporins |
MDR S. Typhi = resistant to chloramphenicol + ampicillin + trimethoprim (plasmid-mediated)
DSC = MIC ≥ 0.125 μg/mL for ciprofloxacin (not reliably detected by standard disk diffusion - use nalidixic acid as surrogate or Etest)
XDR S. Typhi = additionally resistant to fluoroquinolones AND 3rd-generation cephalosporins
Key point for exam: In 2015, 66% of S. Typhi in the USA were DSC (decreased susceptibility to ciprofloxacin). Because of this, fluoroquinolones should no longer be used empirically on the Indian subcontinent.
8. TREATMENT
Antibiotic Therapy (Harrison's 2025 Table):
| Situation | Drug of Choice | Dose | Duration |
|---|---|---|---|
| Empirical | Ceftriaxone (IV) | 2g/day | 10-14 days |
| OR Azithromycin (PO) | 1g/day | 10 days | |
| OR Ciprofloxacin (if no DSC) | 500mg BD | 5-7 days | |
| Fully susceptible | Ciprofloxacin or Ceftriaxone | As above | 5-14 days |
| Alternatives | Chloramphenicol, Amoxicillin, TMP-SMX | Various | 14-21 days |
| MDR typhoid | Ceftriaxone or Azithromycin | As above | 10-14 days |
| XDR typhoid | Azithromycin (oral mild cases) | 1g then 500mg daily | 7 days |
| Uncomplicated (outpatient) | Oral Azithromycin | 1g then 500mg daily | 7 days |
| Complicated (hospitalized) | Parenteral 3rd-gen cephalosporin | Ceftriaxone 2g/day IV | 10-14 days |
Key treatment points:
- Mortality drops from 10-30% (untreated) to <1% with prompt treatment
- Fluoroquinolones now unreliable for Indian subcontinent strains
- Azithromycin is now a preferred oral option
- Chronic carriers: Ampicillin + cholecystectomy (if gallstones present)
9. PROPHYLAXIS (Prevention)
Non-pharmacological (environmental):
- Safe drinking water supply and proper sewage treatment
- Food safety - thorough cooking of poultry/eggs/meat
- Hand hygiene (handwashing with soap)
- Avoid raw fruits/vegetables from sewage-fertilized fields
- Exclude carriers from food handling jobs
- Identify and treat chronic carriers
Pharmacological (chemoprophylaxis):
- Not routinely recommended
- Pre-travel vaccination is the primary strategy
10. VACCINES
Currently available vaccines:
| Vaccine | Type | Route | Age | Efficacy | Duration | Boosters |
|---|---|---|---|---|---|---|
| Ty21a (Vivotif) | Live attenuated oral vaccine (S. Typhi Ty21a strain) | Oral (capsules) | ≥6 years | 50-80% | ~5 years | Every 5 years |
| Vi CPS (Typhim Vi) | Purified Vi capsular polysaccharide | IM injection | ≥2 years | 50-80% | 2-3 years | Every 2-3 years |
| Typhoid Conjugate Vaccine (TCV) | Vi polysaccharide conjugated to tetanus toxoid carrier protein | IM injection | ≥6 months | ~80-90% | Longer (conjugation = better immunogenicity) | Being introduced in endemic countries |
Key vaccine facts for exam:
- Both Ty21a and Vi CPS have 50-80% efficacy
- Ty21a contraindicated in: immunocompromised patients, pregnancy, <6 years, during antibiotic use
- Vi antigen is the basis of the injectable vaccine - it is the capsular polysaccharide that confers immunity
- TCV is WHO-recommended for routine immunization in children in high-burden countries
- Vaccination recommended for travelers to endemic regions, especially rural areas
- Only 3% of US typhoid cases had received vaccine in the prior 5 years!
Mechanism of immunity:
- O and Vi antibodies = resistance to infection (circulating antibodies)
- Secretory IgA = prevents attachment to intestinal epithelium
- Reinfection possible but usually milder
- Relapses occur in 2-3% despite antibodies (organisms sequestered intracellularly)
11. QUICK EXAM SUMMARY TABLE
| Feature | Key Fact |
|---|---|
| Causative organism | Salmonella enterica serovar Typhi (also Paratyphi A, B, C) |
| Gram stain | Gram-negative rod |
| Reservoir | Humans ONLY (no animal reservoir) |
| Transmission | Fecal-oral (contaminated water/food) |
| Incubation | 10-14 days |
| Pathogenesis key step | M-cells → Peyer's patches → bacteremia |
| Gold standard diagnosis | Blood culture (week 1-2); Bone marrow culture (any time) |
| Best single specimen | Bone marrow culture (>90% sensitivity) |
| WBC in typhoid | Normal or LOW (leukopenia) |
| Widal test principle | Agglutination of O and H antigens |
| Widal significant titer | ≥1:160 for both O and H |
| O antibody timing | Day 6-8 |
| H antibody timing | Day 10-12 |
| Drug of choice now | Ceftriaxone or Azithromycin (due to fluoroquinolone resistance) |
| MDR definition | Resistant to Chloramphenicol + Ampicillin + TMP-SMX |
| Vaccine (oral) | Ty21a (live attenuated) |
| Vaccine (injectable) | Vi CPS or TCV (conjugate) |
| Chronic carrier site | Gallbladder |
| Classic rash | Rose spots (salmon-colored, blanching, maculopapular, trunk) |
| Most feared complication | Intestinal perforation (3rd week) |
12. HIGH-YIELD MNEMONICS
"5 Ps" of Typhoid pathogenesis:
Peyer's patches → Primary bacteremia → Proliferation in macrophages → Peyer's patch necrosis → Perforation risk
Widal limitations - "CAVE":
Cross-reactions, Antibiotics cause false negatives, Vaccination causes false positives, Endemic areas have background titers
Stages of fever - "1-2-3 Rule":
- Week 1: rising fever + blood culture positive
- Week 2: plateau fever + rose spots + Widal turns positive
- Week 3: complications (perforation/hemorrhage) + stool culture positive
Sources: Harrison's Principles of Internal Medicine 22E (2025) - Chapter on Enteric Fever; Jawetz Melnick & Adelberg's Medical Microbiology 28E - Chapter 15; Park's Textbook of Preventive & Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.