IVF
Reading File
Asking for Preferences
Finding Sources
Searching the Web
IVF in vitro fertilization process overview steps 2024
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all I need for a thorough, well-illustrated answer.
In Vitro Fertilization (IVF) - How It Works
IVF is an assisted reproductive technology (ART) where eggs are fertilized by sperm outside the body in a laboratory, and the resulting embryo is transferred into the uterus. It was pioneered in 1978 by Robert G. Edwards and Patrick Steptoe, leading to the birth of Louise Brown, the world's first "test tube baby." Since then, several million children worldwide have been born via IVF.
Step-by-Step Process
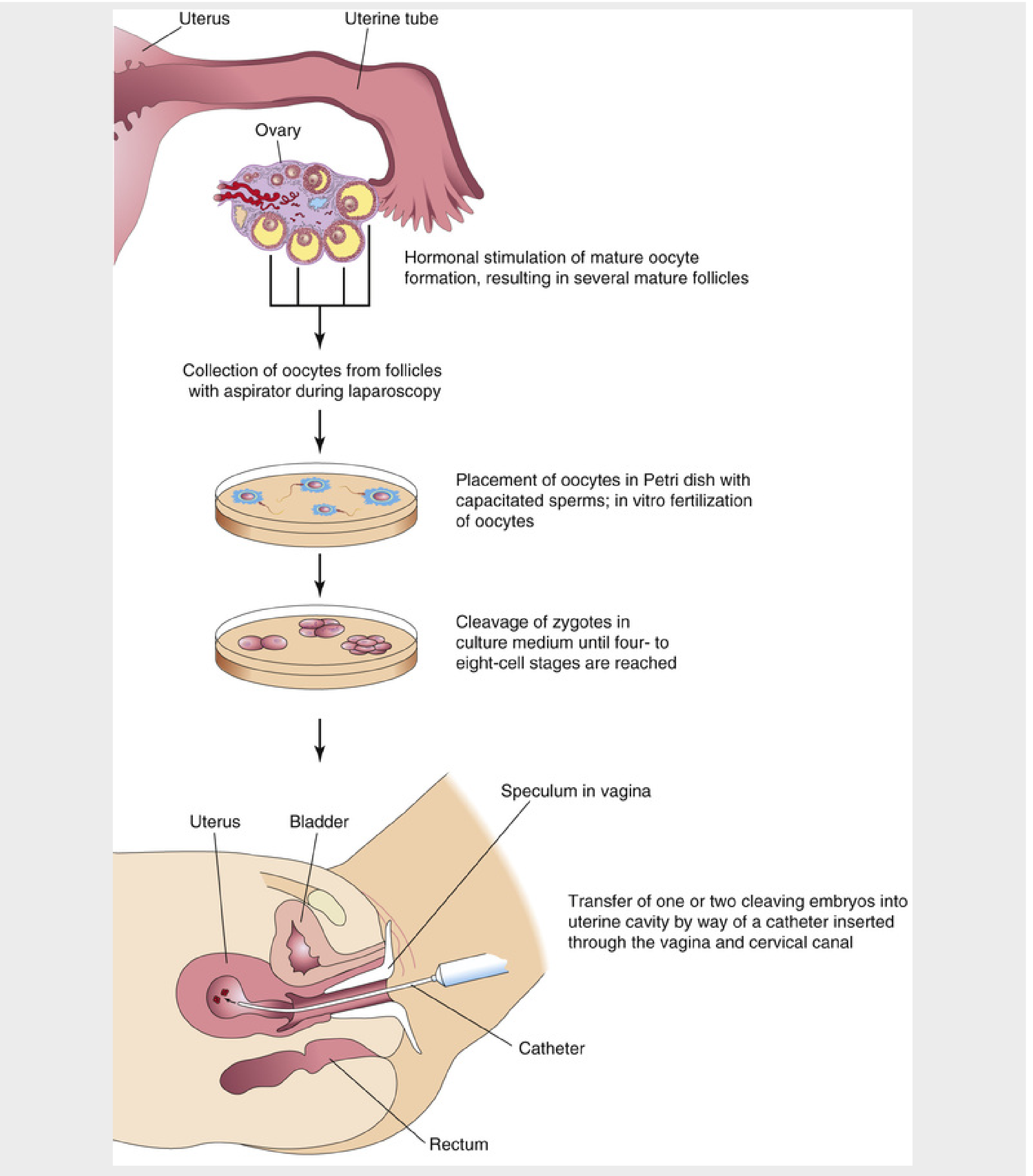
1. Ovarian Stimulation (Superovulation)
The woman receives fertility medications - typically clomiphene citrate or gonadotropins - to stimulate the ovaries to produce multiple mature follicles simultaneously (rather than the single egg that naturally matures each cycle). This is sometimes preceded by a "priming" phase using oral contraceptives or estrogen to synchronize follicular development and maximize the number of retrievable eggs.
Preventing premature LH surge: GnRH agonists or antagonists are used during stimulation to prevent the egg from being released too early. Fixed vs. flexible GnRH antagonist protocols are the two main options.
Trigger shot: When follicles reach adequate size, an hCG or GnRH agonist injection is given to trigger final egg maturation, timed precisely ~36 hours before retrieval.
2. Egg Retrieval (Oocyte Aspiration)
Mature oocytes are aspirated from the follicles either:
- By laparoscopy (older technique), or
- More commonly today, by a transvaginal ultrasound-guided needle passed through the vaginal wall into the follicles.
This is done under light sedation or anesthesia.
3. Fertilization in the Lab
Collected oocytes are placed in a Petri dish with capacitated sperm in a special culture medium. Two approaches:
- Conventional IVF - sperm and eggs are incubated together and fertilization occurs naturally in the dish.
- ICSI (Intracytoplasmic Sperm Injection) - a single sperm is injected directly into the cytoplasm of the oocyte. Used when sperm count/motility is very low, or when conventional IVF has failed.
4. Embryo Culture and Monitoring
Fertilized eggs (zygotes) are monitored microscopically as they undergo cleavage. Embryos are cultured for 3 to 5 days - reaching the 4-8 cell stage or the blastocyst stage (day 5), which is generally preferred for transfer as it improves selection of viable embryos.
5. Embryo Transfer
One to three embryos (depending on the mother's age and clinical factors) are loaded into a thin flexible catheter, which is passed through the vagina and cervical canal into the uterine cavity. The embryo(s) are gently deposited. The patient rests supine for several hours afterward.
- The current trend is toward single embryo transfer (SET) to reduce the risk of multiple gestation.
- Surplus embryos can be cryopreserved (frozen in liquid nitrogen with a cryoprotectant like glycerol or DMSO) for future use.
6. Luteal Phase Support & Pregnancy Test
Progesterone supplementation supports the uterine lining. A blood pregnancy test (beta-hCG) is done about 10-14 days after transfer.
Related ART Techniques
| Technique | Description |
|---|---|
| ICSI | Single sperm injected directly into egg; used for severe male factor infertility |
| GIFT | Gametes transferred directly into the fallopian tube (largely obsolete now) |
| ZIFT | Zygote transferred into the fallopian tube (largely obsolete) |
| PGT (Preimplantation Genetic Testing) | Genetic screening of embryos before transfer; includes PGD (diagnosis) and PGS (screening) |
| Oocyte cryopreservation | Egg freezing for fertility preservation (e.g., before cancer treatment) |
| Gestational carrier | Embryo transferred into a surrogate's uterus |
Key Risks and Considerations
- Multiple gestation - a serious complication when more than one embryo is transferred; carries risks of preterm birth and low birth weight.
- Ovarian Hyperstimulation Syndrome (OHSS) - ovaries over-respond to stimulation medications; can range from mild (bloating) to severe (fluid shifts, thrombosis). Improved protocols have significantly reduced this.
- Increased preterm birth and low birth weight - reported across multiple studies for ART-conceived children.
- Birth defects - slightly elevated absolute risk, though still low overall.
- Ectopic pregnancy - possible if embryo implants in the tube rather than the uterus.
- Emotional stress - the most common reason patients discontinue therapy.
- Cancer risk - current evidence does not show a significantly increased risk of breast, uterine, or ovarian cancer from superovulation medications.
Success Rates
Live birth rates per cycle vary primarily with maternal age - generally 40-50% per cycle for women under 35, declining progressively with age. Prediction models now allow personalized estimates. The CDC's National ART Surveillance System and the Society for Assisted Reproductive Technology (SART) publish annual outcome data.
Sources: The Developing Human: Clinically Oriented Embryology, Ch. 2 | Berek & Novak's Gynecology, Ch. on Infertility & ART
This is a shared conversation. Sign in to Orris to start your own chat.