Peptic ulcer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information to write a thorough response. Let me compile the full answer.
Peptic Ulcer Disease (PUD)
Definition
A peptic ulcer is an excoriated area of the stomach or intestinal mucosa caused by the digestive action of gastric acid and pepsin. Although the name implies pepsin as the culprit, acid is actually the indispensable factor - ulcers do not form in its absence, and all peptic ulcers can be healed by rendering a patient virtually achlorhydric with proton pump inhibitors (PPIs). - Bailey and Love's Short Practice of Surgery 28th Ed., p. 1178
Common Sites
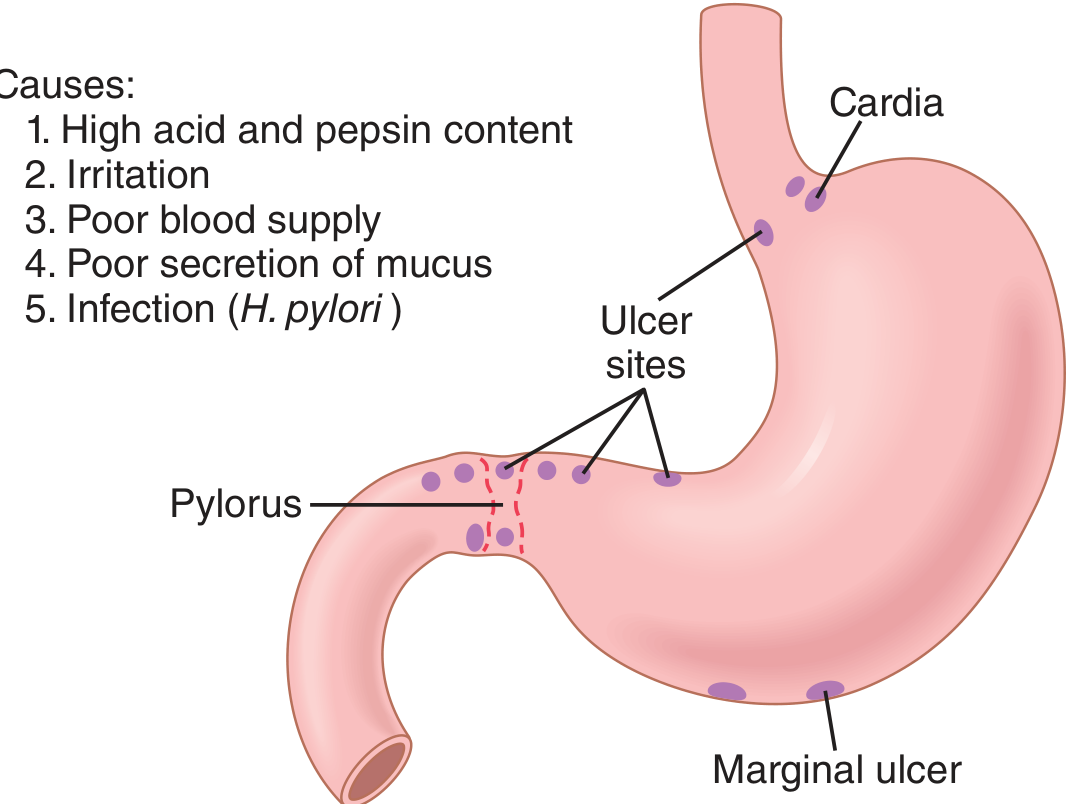
Figure: Common ulcer sites and causes - Guyton and Hall Textbook of Medical Physiology
The most frequent sites are:
- First part of the duodenum (most common overall)
- Lesser curve of the stomach (especially the incisura angularis)
- Prepyloric / pyloric channel
- Distal esophagus (acid reflux)
- Post-surgical stoma (marginal ulcer at gastrojejunostomy)
- Meckel's diverticulum (if ectopic gastric mucosa is present)
Ulcers occur at junctions between different epithelial types, where resistance to acid damage is lowest. - Guyton and Hall, p. 824
Epidemiology
- Affects >4 million individuals in the US each year
- Lifetime risk: ~10% in males, ~4% in females
- Duodenal ulcers (DU) are more common than gastric ulcers (GU)
- DU: more common in men; GU: equal gender incidence, older patients
- GU more prevalent in low socioeconomic groups and resource-poor nations
- Robbins & Kumar Basic Pathology, p. 598
Pathogenesis: The Balance Model
PUD results from an imbalance between mucosal damaging forces and protective mechanisms.
Protective Mechanisms
- Mucus layer and bicarbonate secretion (surface mucous cells, Brunner glands)
- Mucosal blood flow
- Epithelial tight junctions and rapid cell turnover
- Duodenal alkalinization by pancreatic bicarbonate and bile
- Feedback inhibition of gastric emptying when acid enters the duodenum (secretin release → more pancreatic HCO₃⁻)
Damaging Factors
- H. pylori infection
- NSAIDs / aspirin
- Excess gastric acid secretion
- Cigarette smoking (reduces mucosal blood flow, impairs healing)
- High-dose corticosteroids (suppress prostaglandin synthesis)
- Guyton and Hall, p. 825; Robbins & Kumar, p. 598
Etiology
1. Helicobacter pylori
-
70% of all PUD is associated with H. pylori
- Only 5-10% of infected individuals develop ulcers - host factors and bacterial strain virulence matter
- H. pylori breaks down the mucosal barrier and stimulates acid secretion
- Testing and eradication are mandatory in all confirmed PUD cases
- Robbins & Kumar, p. 598
2. NSAIDs / Aspirin
- Increasingly the most common cause of gastric ulcers in developed countries (as H. pylori rates fall)
- Mechanism: inhibit COX-1 → reduce prostaglandin E₂ → reduced mucus and bicarbonate secretion
- Low-dose aspirin use in the aging population is driving this trend
3. Zollinger-Ellison Syndrome (ZES)
- Gastrin-secreting tumors (gastrinomas) cause massive acid hypersecretion
- Multiple ulcers in stomach, duodenum, and even jejunum
- Should be suspected in H. pylori-negative, non-NSAID PUD
- Robbins & Kumar, p. 599
4. Other Risk Factors
- Alcohol-related cirrhosis
- Chronic renal failure (hypercalcemia → gastrin ↑)
- Hyperparathyroidism (hypercalcemia → gastrin ↑)
- Chronic obstructive pulmonary disease
Morphology / Pathology
Macroscopic
- Duodenal ulcers: usually in the first part of the duodenum; often solitary but "kissing ulcers" (anterior + posterior) occur
- Gastric ulcers: tend to be larger; lesser curve, especially at the incisura angularis
- Chronic ulcers penetrate the mucosa into the muscle coat → fibrosis and scarring
- Fibrosis can cause pyloric stenosis or hourglass deformity of the stomach
- Posterior gastric ulcers may erode into the pancreas or splenic artery
Endoscopic Appearance
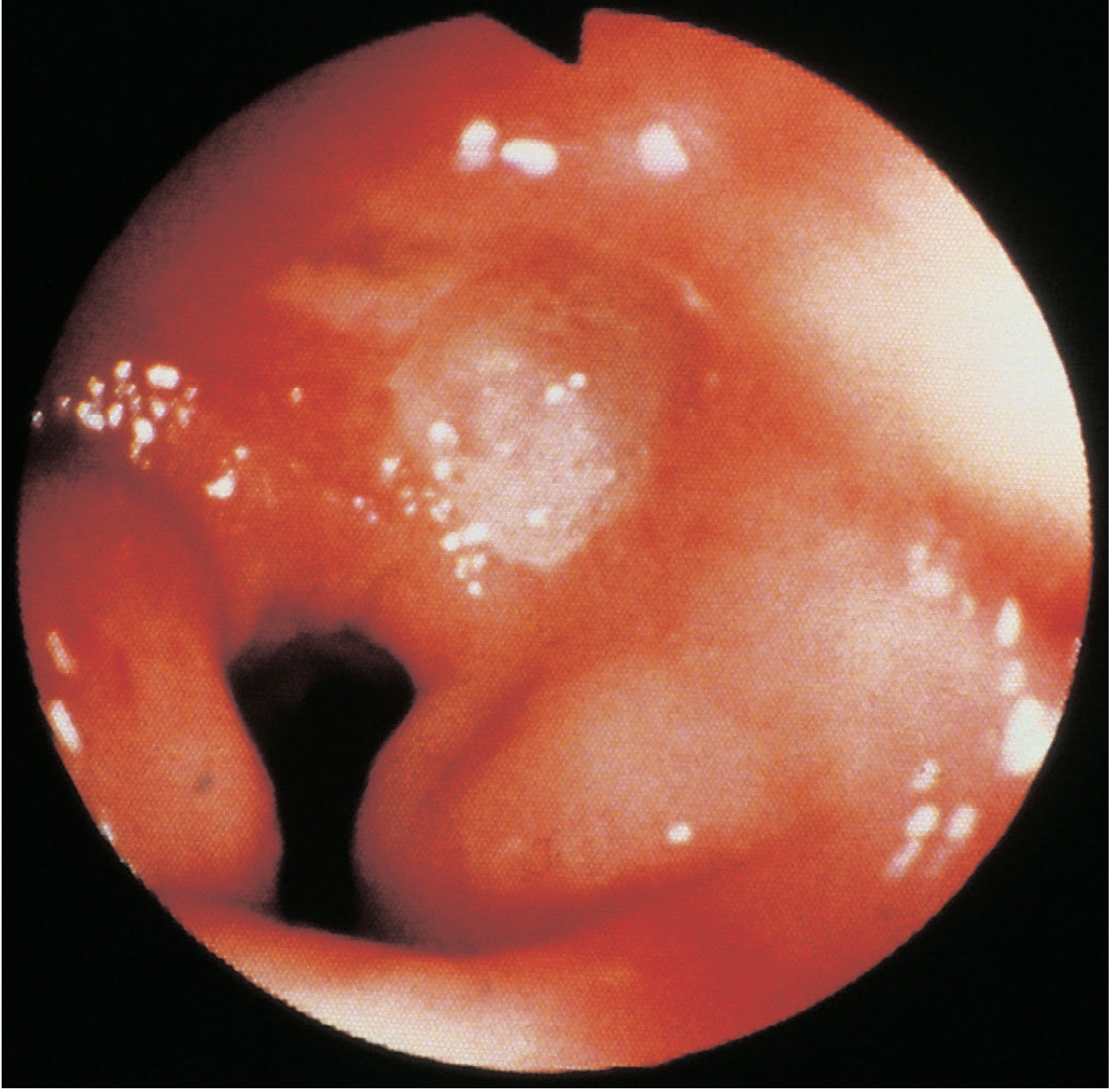
Figure: Endoscopic view of a duodenal ulcer - Bailey and Love's Surgery
Microscopic
- Base covered with granulation tissue
- Evidence of endarteritis obliterans in chronic cases
- Epithelial downgrowth during healing can mimic invasion (important not to misinterpret as carcinoma)
- Bailey and Love, p. 1179
Malignancy Risk
- Duodenal ulcers: virtually never malignant
- Gastric ulcers: may be malignant or may coexist with cancer - all gastric ulcers require multiple biopsies
- Bailey and Love, p. 1180
Clinical Features
| Feature | Detail |
|---|---|
| Epigastric pain | Gnawing, burning, may radiate to back |
| Pain-food relationship | DU: relieved by food; GU: may worsen with food |
| Periodicity | Weeks of symptoms followed by remission |
| Vomiting | Not a prominent feature unless stenosis present |
| Weight changes | Loss in GU; occasional gain in DU |
| Bleeding | Chronic (microcytic anaemia) or acute (haematemesis/melaena) |
Symptoms between DU and GU are clinically indistinguishable. - Bailey and Love, p. 1179
Investigation
- Upper GI Endoscopy - gold standard; allows biopsy (mandatory for all gastric ulcers)
- H. pylori testing - CLO (rapid urease) test on antral biopsy, urea breath test, stool antigen test
- Barium meal - less common now; shows ulcer crater
- Serum gastrin - if ZES suspected (H. pylori-negative, non-NSAID, multiple/atypical ulcers)
Treatment
Medical (First-Line)
The vast majority of uncomplicated peptic ulcers are treated medically.
1. Proton Pump Inhibitors (PPIs)
- Standard-dose PPI (e.g., omeprazole 20 mg BD, lansoprazole 30 mg BD)
- Reduces acid secretion by blocking H⁺/K⁺-ATPase
- Continue for 4-8 weeks (DU) or 8-12 weeks (GU)
2. H. pylori Eradication
- Mandatory in all H. pylori-positive patients, regardless of whether this is first episode or recurrence
- First-line: 14-day triple therapy = PPI + clarithromycin + amoxicillin (or metronidazole)
- Eradication rates: 70-85% with triple therapy
- Eradication reduces recurrence dramatically: from 59-67% → <10-20%
- If triple therapy fails (usually due to clarithromycin resistance), use bismuth quadruple therapy or levofloxacin triple therapy
- Harrison's Principles of Internal Medicine 22E, p. 2570; Textbook of Family Medicine 9e
3. NSAID Management
- Stop NSAIDs if possible
- If NSAIDs must continue: use PPI co-prescription; test and eradicate H. pylori
- Misoprostol (prostaglandin analogue, 200 µg QID) is an alternative mucosal protectant but causes diarrhea in 10-30% and is contraindicated in pregnancy
Surgical Treatment
- Elective surgery for uncomplicated PUD is now very rarely performed - reserved for emergencies
- Historical procedures: Billroth I (gastroduodenostomy), Billroth II/Polya (gastrojejunostomy), vagotomy
- Now only performed for complications
Complications ("PBS")
| Complication | Key Points |
|---|---|
| Perforation | Anterior DU perforates more commonly; presents with sudden severe epigastric pain, board-like rigidity; erect CXR shows free air under diaphragm; treated by laparoscopic or open repair (Graham patch) |
| Bleeding | Posterior DU erodes gastroduodenal artery; most common cause of upper GI bleeding; managed by endoscopic haemostasis (adrenaline injection, clips, thermocoagulation) ± interventional radiology ± surgery |
| Stenosis / Gastric outlet obstruction | Chronic fibrosis → pyloric stenosis; presents with projectile vomiting, succussion splash, hypochloraemic hypokalaemic metabolic alkalosis; treated by balloon dilatation or surgery |
- Bailey and Love, p. 1178
Rockall Score for Upper GI Bleeding Risk Stratification
| Score | Rebleeding Rate | Mortality |
|---|---|---|
| 0-1 | <5% | 0% |
| 3 | 11% | 2.9% |
| 5 | 24% | 10.8% |
| ≥8 | ~42% | 41% |
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Refractory / Non-Healing Ulcers
A small minority fail to heal despite appropriate therapy. Approach:
- Confirm with repeat endoscopy (mandatory for all gastric ulcers)
- Check for persistent H. pylori infection (biopsies - breath test may be false-negative soon after treatment)
- Assess adherence and bacterial culture for resistance
- Exclude continued NSAID use
- Measure serum gastrin to rule out ZES
- Consider rare IgG4-related ulceration
- Bailey and Love, p. 1182
Key Summary Points
- PUD = imbalance between acid/pepsin aggression and mucosal defense
- Two dominant causes: H. pylori (>70%) and NSAIDs
- Diagnosis: upper GI endoscopy + H. pylori testing (all gastric ulcers must be biopsied)
- Treatment: PPI + H. pylori eradication (14-day triple therapy)
- Eradication dramatically reduces recurrence and bleeding
- Complications: perforation, bleeding, stenosis - now mainly managed endoscopically/radiologically; surgical intervention reserved for failures
- Elective surgery for PUD is now obsolete
Sources:
- Guyton and Hall Textbook of Medical Physiology, Ch. 67
- Robbins & Kumar Basic Pathology
- Bailey and Love's Short Practice of Surgery 28th Ed., Ch. 67
- Harrison's Principles of Internal Medicine 22E (2025), Ch. on PUD
- Textbook of Family Medicine 9e
Malabsorption syndrome
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed to write a thorough, well-illustrated answer on malabsorption syndrome. Here it is:
Malabsorption Syndrome
Definition
Malabsorption syndrome is a clinical state in which there is impaired absorption of one or more nutrients (fats, carbohydrates, proteins, vitamins, minerals, water) from the gastrointestinal tract, leading to nutritional deficiencies and their consequences. The hallmark sign is steatorrhea - bulky, frothy, greasy, yellow or clay-colored stools with excessive fecal fat. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis: The Four Phases of Absorption
Malabsorption results from a disturbance in at least one of four phases:
| Phase | Process | Examples of Disorders |
|---|---|---|
| 1. Intraluminal digestion | Proteins, carbs, fats broken into absorbable forms | Pancreatic insufficiency, bile acid deficiency, bacterial overgrowth |
| 2. Terminal digestion | Brush-border hydrolysis by disaccharidases/peptidases | Celiac disease, lactase deficiency, viral enteritis |
| 3. Transepithelial transport | Absorption and processing across intestinal epithelium | Celiac disease, Whipple's disease, abetalipoproteinemia |
| 4. Lymphatic transport | Chylomicron transport via lacteals | Intestinal lymphangiectasia, Whipple's disease |
In most disorders, more than one phase is disturbed simultaneously. - Robbins Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
Causes Classified by Mechanism
A. Intraluminal Maldigestion
1. Pancreatic Exocrine Insufficiency
- Occurs when >90% of pancreatic secretory function is lost
- Causes: chronic pancreatitis (most often from alcohol), cystic fibrosis, pancreatic duct obstruction, somatostatinoma
- Results in fat, protein, and carbohydrate maldigestion
- Treatment: oral pancreatic enzyme supplementation
2. Bile Acid Deficiency
- Biliary obstruction or cirrhosis → reduced intraluminal bile acids → impaired micelle formation → fat maldigestion
- Primary bile acid malabsorption (terminal ileal disease/resection, Crohn's ileitis)
3. Small Intestinal Bacterial Overgrowth (SIBO)
- Bacteria deconjugate bile acids → impaired micelle formation
- Occurs in blind loops, multiple small bowel diverticula, motility disorders
- Detected by lactulose or glucose hydrogen breath test; treated with antibiotics
B. Mucosal Malabsorption (Enteropathies)
1. Celiac Disease (Gluten-Sensitive Enteropathy)
The most important cause of mucosal malabsorption. Affects ~1% of the population.
Pathogenesis:
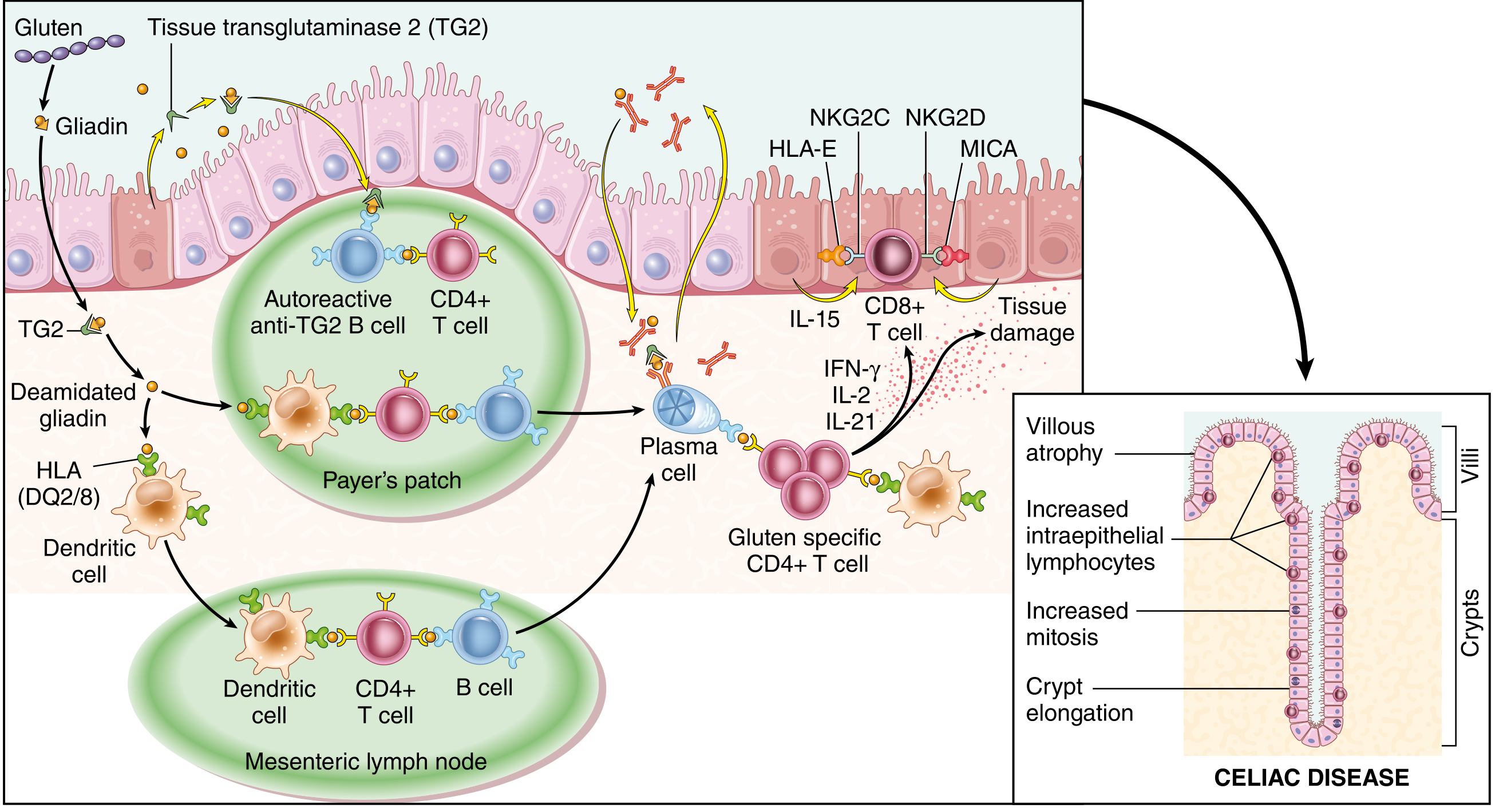
Figure: Celiac disease pathogenesis showing gliadin deamidation by TG2, HLA DQ2/8-mediated CD4+ T cell activation, CD8+ intraepithelial lymphocyte expansion, and resulting villous atrophy - Robbins Cotran & Kumar
- Triggered by gluten (wheat, rye, barley) in genetically predisposed individuals
- HLA DQ2 (~90% of cases) or DQ8 required
- Tissue transglutaminase 2 (TG2) deamidates gliadin peptides → bound by DQ2/8 on antigen-presenting cells → CD4+ T cell activation → IFN-γ, IL-2, IL-21 release → CD8+ intraepithelial lymphocyte expansion → epithelial damage
- Histology: villous atrophy, crypt hyperplasia, intraepithelial lymphocytosis
- ~75% concordance in monozygotic twins
- Associated with: type 1 diabetes, thyroiditis, Sjögren's syndrome, IgA nephropathy
Diagnosis:
- Anti-tissue transglutaminase IgA (anti-TTG IgA) + total IgA level (to exclude IgA deficiency)
- Duodenal/proximal jejunal biopsy (confirmatory)
- Treatment: strict gluten-free diet (lifelong)
2. Tropical Sprue
- Similar histology to celiac disease (villous atrophy, crypt hyperplasia)
- Occurs in residents of/travelers to tropical climates
- Infectious etiology suspected (abrupt onset, responds to antibiotics + folate)
- Causes folate and B12 deficiency prominently
3. Whipple's Disease
- Due to Tropheryma whipplei bacillus → macrophage infiltration of small bowel mucosa
- Primarily impairs lymphatic transport
- Typically in young to middle-aged men
- Classic tetrad: diarrhea/steatorrhea, arthralgias, fever, lymphadenopathy + extreme fatigue
- May affect CNS and endocardium
- PAS-positive macrophages in lamina propria (pathognomonic)
- Treatment: antibiotics (usually trimethoprim-sulfamethoxazole)
4. Other Mucosal Causes
- Parasites: Giardia lamblia (most common parasitic cause), Cryptosporidium, Cyclospora
- Crohn's disease (especially with ileal involvement)
- Autoimmune enteropathy
- Drug-induced: olmesartan, mycophenolate, colchicine, cholestyramine
- AIDS-related: Mycobacterium avium-intracellulare (similar picture to Whipple's)
C. Post-Mucosal / Lymphatic Obstruction
- Congenital intestinal lymphangiectasia or acquired obstruction (tumor, trauma, cardiac disease, infection)
- Unique pattern: fat malabsorption + protein-losing enteropathy (edema, hypoalbuminemia) + lymphocytopenia
- Carbohydrate and amino acid absorption are preserved
- Harrison's Principles of Internal Medicine 22E, p. 1170
D. Short Bowel Syndrome
- Massive small bowel resection (e.g., mesenteric ischemia, Crohn's)
- Critical mass of absorptive surface lost
- Management: enteral/parenteral nutrition, intestinal adaptation, sometimes transplantation
E. Specific Enzyme Deficiencies
- Lactase deficiency: most common, causes osmotic diarrhea, bloating, flatulence with dairy - abates with fasting
- Disaccharidase deficiencies: impair terminal digestion phase
- Abetalipoproteinemia: rare defect in chylomicron formation → fat malabsorption in children; associated with acanthocytic RBCs, ataxia, retinitis pigmentosa
Clinical Features
GI Symptoms
- Chronic diarrhea (bulky, frothy, offensive, greasy stools = steatorrhea)
- Abdominal bloating, distension, flatulence
- Borborygmi (loud bowel sounds)
- Abdominal cramps
- Weight loss, muscle wasting
- Anorexia
Systemic Manifestations (from nutrient deficiencies)
| Deficient Nutrient | Clinical Manifestation |
|---|---|
| Fat / Carbohydrate | Diarrhea, weight loss, growth retardation |
| Protein | Muscle wasting, edema (hypoalbuminemia) |
| Iron | Microcytic anemia, cheilosis, angular stomatitis |
| Vitamin B12 / Folate | Megaloblastic anemia, glossitis, paresthesias, ataxia (B12) |
| Vitamin D / Calcium | Bone pain, fractures, tetany, osteomalacia/rickets |
| Magnesium | Paresthesias, tetany |
| Vitamin K | Ecchymoses, bleeding (prolonged PT) |
| Vitamin A | Night blindness, xerophthalmia, hyperkeratosis |
| Vitamin E | Paresthesias, ataxia, retinopathy |
| Zinc | Dermatitis, hypogeusia (loss of taste), diarrhea |
| Selenium | Cardiomyopathy |
- Goldman-Cecil Medicine, Table 126-5
Investigations
Diagnostic Flowchart
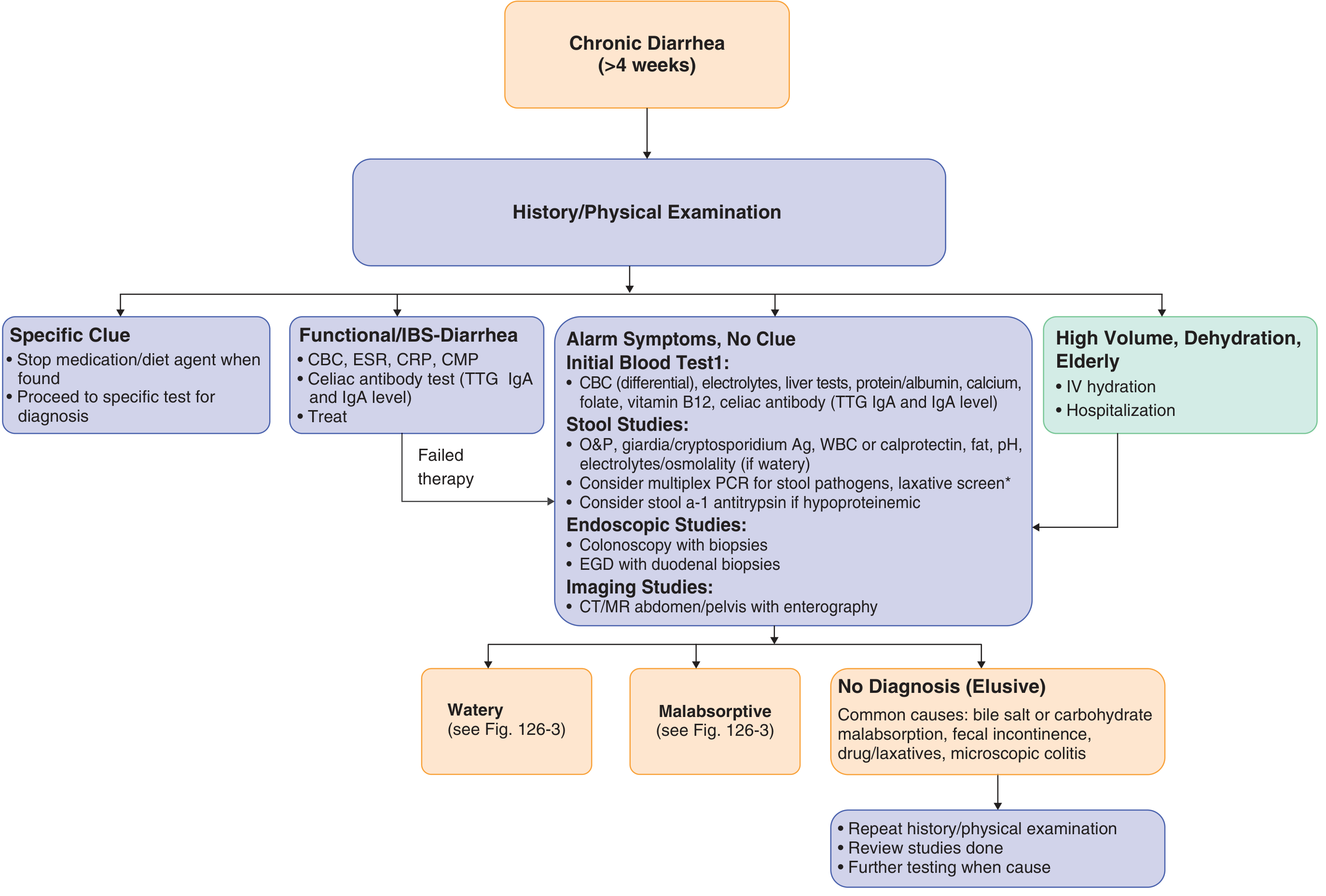
Figure: Algorithm for evaluation of chronic diarrhea including malabsorptive causes - Goldman-Cecil Medicine
Blood Tests
- CBC: anemia (microcytic = Fe; macrocytic = B12/folate deficiency)
- Serum iron, ferritin, vitamin B12, folate, vitamin A/D/E/K (PT)
- Serum albumin and total protein
- Anti-TTG IgA + total IgA (celiac screening)
- Serum calcium, magnesium, phosphate
Stool Tests
- Qualitative stool fat: Sudan stain (screening)
- Quantitative stool fat (72-hour collection on 100 g/day fat diet): gold standard; >7 g/24 hr = abnormal; sensitivity 90%, specificity 90%
- Stool ova and parasites + Giardia antigen/PCR
- Fecal calprotectin / leukocytes (if inflammatory cause suspected)
- Fecal elastase-1 (for pancreatic exocrine insufficiency)
Breath Tests
- Hydrogen breath test: lactose, fructose malabsorption or SIBO
- 14C or 13C-triolein breath test: fat malabsorption
Imaging
- CT/MR enterography: structural small bowel disease, Crohn's, lymphoma, diverticula
- MRCP / CT pancreas: pancreatic disease
Endoscopy / Biopsy
- Upper GI endoscopy with duodenal biopsies (multiple): mandatory if mucosal disease suspected
- Key histological patterns:
- Celiac disease: villous atrophy + crypt hyperplasia + intraepithelial lymphocytosis
- Whipple's: PAS-positive macrophages in lamina propria
- Tropical sprue: similar to celiac but less severe
- Giardia: trophozoites on biopsy
Specific Tests
- Secretin stimulation test: pancreatic function
- Small bowel aspirate/culture: SIBO (>10⁵ organisms/mL)
- Serum gastrin: if Zollinger-Ellison suspected
- Serum 7αC4 or fecal bile acids: bile acid diarrhea
Types of Diarrhea - Distinguishing Features
| Type | Stool Character | Effect of Fasting | Osmotic Gap |
|---|---|---|---|
| Osmotic (e.g., lactase deficiency) | Watery | Stops | >50 mOsm above plasma |
| Secretory (e.g., VIPoma) | Watery, large volume | Persists | Normal (<50) |
| Malabsorptive | Steatorrhea, bulky | Improves | Variable |
| Exudative / Inflammatory | Bloody, purulent | Persists | Variable |
Management Principles
| Cause | Treatment |
|---|---|
| Celiac disease | Strict, lifelong gluten-free diet |
| Pancreatic insufficiency | Oral pancreatic enzyme replacement (high-lipase), fat-soluble vitamin supplementation |
| SIBO | Antibiotics (rifaximin, metronidazole, amoxicillin-clavulanate), treat underlying cause |
| Lactase deficiency | Lactose-free diet, lactase enzyme supplements |
| Tropical sprue | Tetracycline + folic acid |
| Whipple's disease | Long-term trimethoprim-sulfamethoxazole |
| Bile acid malabsorption | Cholestyramine (bile acid sequestrant) |
| Short bowel syndrome | Nutritional support (enteral > parenteral), teduglutide (GLP-2 analogue) |
| Giardiasis | Metronidazole / tinidazole |
| All cases | Correct nutritional deficiencies: iron, B12, folate, fat-soluble vitamins (A, D, E, K), calcium, magnesium |
Key Summary Points
- Malabsorption = failure of one or more of four absorption phases (intraluminal, terminal, transepithelial, lymphatic)
- Hallmark: steatorrhea + weight loss + multiple nutritional deficiencies
- Three most common causes in Western countries: pancreatic insufficiency, celiac disease, SIBO
- Celiac disease: HLA DQ2/8, anti-TTG IgA antibody, villous atrophy on biopsy, treat with gluten-free diet
- Whipple's disease: T. whipplei, PAS-positive macrophages, systemic features (arthralgia, fever, CNS)
- Stool fat test (72-hour collection) = best screening test for fat malabsorption
- Management = treat underlying cause + correct nutritional deficiencies
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.), Ch. 17
- Robbins & Kumar Basic Pathology, Ch. 13
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 5
- Goldman-Cecil Medicine International Edition, Ch. 126
- Yamada's Textbook of Gastroenterology 7th Ed., Ch. 27
Preterm labor
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the comprehensive information needed to write a thorough answer. Let me compile it.
Preterm Labor
Definition
Preterm labor is defined as uterine contractions occurring before 37 weeks of gestation that cause cervical change (dilation or effacement). Cervical change is confirmed if:
- Initial examination shows cervix ≥2 cm dilated or ≥80% effaced, or
- Interval examinations document progressive effacement or dilation
Preterm contractions without cervical change do not constitute preterm labor and do not require intervention. - Textbook of Family Medicine 9e
Preterm birth (delivery before 37 weeks) occurs in >10% of pregnancies in the US and is a leading cause of neonatal morbidity and mortality. - Goodman & Gilman's Pharmacological Basis of Therapeutics
Epidemiology
- Preterm birth rate before 34 weeks: 20% in twin pregnancies, 63% in triplet pregnancies (US, 2019)
- 55% of twins are low birth weight (<2500 g); 10% are very low birth weight (<1500 g)
- Not all are spontaneous - many are medically indicated preterm births
- Overdiagnosis of preterm labor occurs in 40-70% of women presenting with symptoms, due to imprecise clinical criteria
- Creasy & Resnik's Maternal-Fetal Medicine
Risk Factors
| Category | Risk Factors |
|---|---|
| Obstetric history | Prior preterm labor/birth (single strongest predictor), cervical insufficiency |
| Current pregnancy | Multiple gestation, polyhydramnios, placenta previa, placental abruption, pPROM |
| Infection | Bacterial vaginosis, bacteriuria/UTI, chorioamnionitis |
| Maternal factors | Low socioeconomic status, African American ethnicity, poor nutrition, low maternal weight (<50 kg), poor pregnancy weight gain, poor prenatal care |
| Uterine factors | Uterine anomalies, uterine leiomyoma |
| Substances | Cocaine use, nicotine/smoking |
- Textbook of Family Medicine 9e, Table 20-17
Pathophysiology
Preterm labor results from premature activation of the normal parturition pathway. The key mechanisms include:
- Infection/inflammation - Intrauterine or decidual infection (most common and important) → cytokines (IL-1, IL-6, TNF-α) → prostaglandin synthesis (PGE₂, PGF₂α) → uterine contractions + cervical ripening
- Uteroplacental ischemia - Placental insufficiency, abruption, preeclampsia → decidual hemorrhage → thrombin → uterine contractions
- Uterine overdistension - Multiple gestation, polyhydramnios → mechanical stretch → myometrial activation
- Cervical insufficiency - Structural weakening of the cervix (congenital or acquired) → silent cervical dilation without contractions
- Premature activation of the fetal HPA axis - Fetal stress → CRH → prostaglandins → labor
The clinical presentations of preterm labor, preterm premature rupture of membranes (pPROM), and cervical insufficiency are indistinct and overlapping. - Creasy & Resnik; Goodman & Gilman's
Clinical Features / Diagnosis
Symptoms
Preterm labor must be considered whenever abdominal or pelvic symptoms occur after 16 weeks:
- Pelvic pressure
- Increased vaginal discharge
- Low backache
- Menstrual-like cramps
- Uterine contractions (painful or painless)
- Symptoms suggest preterm labor more by their persistence than severity
Contractions against a closed, uneffaced cervix tend to be painful; when cervical effacement precedes contractions, recurrent pressure or tightening may be the only symptom.
Diagnostic Criteria
Traditional criteria (most reliable):
- Contraction frequency ≥6 per hour AND
- Cervical dilation ≥3 cm OR effacement ≥80%
At lower thresholds, false-positive rates are very high. - Creasy & Resnik, p. 897
Diagnostic Tests
1. Transvaginal Ultrasound (TVU) Cervical Length
- Measured at 20-24 weeks for risk stratification
- Cervical length ≥30 mm → preterm labor unlikely despite symptoms
- Cervical length <20 mm → 10-fold positive likelihood ratio for delivery before 32 weeks (in twins)
- Cervical length <15 mm in symptomatic women → associated with delivery within 7 days
| Cervical Length | Sensitivity | Specificity | NPV |
|---|---|---|---|
| <15 mm | 74% | 89% | 93% |
| <20 mm | 75% | 80% | 96% |
| CL + fFN (15-30 mm) | 71% | 97% | 99% |
2. Fetal Fibronectin (fFN)
- Tested in cervicovaginal fluid at 22-35 weeks
- Released from chorion-decidua interface when disrupted
- Used primarily for its high negative predictive value
- Negative fFN → extremely reassuring; patient will likely not deliver for at least 7-10 days
- Positive fFN → warrants closer surveillance or treatment
- Specimen collected before digital examination (contaminated by lubricants, blood, semen)
3. Combination Protocol
- Cervical length >30 mm: low risk - avoid unnecessary treatment
- Cervical length 15-30 mm: perform fFN testing
- Cervical length + fFN both positive: high risk for imminent delivery
Initial Assessment
- Uterine contraction monitoring + fetal heart rate monitoring (lateral recumbent position)
- Full history and physical examination (rule out treatable causes, contraindications to tocolysis)
- Sterile speculum exam if membrane rupture suspected (nitrazine + ferning test)
- Digital cervical exam only if no rupture suspected
- Urinalysis and urine culture (UTI as precipitant)
- Cervical cultures: GBS, Chlamydia, N. gonorrhoeae, HSV
- Rule out chorioamnionitis: uterine tenderness, fever, leukocytosis, fetal tachycardia
- Ultrasound: estimated fetal weight, amniotic fluid index, biophysical profile score (low BPP may contraindicate tocolysis)
Management
Step 1: Identify and Treat Precipitating Causes
- UTI → antibiotics
- BV → metronidazole or clindamycin
Step 2: Evaluate for Contraindications to Tocolysis
Maternal contraindications:
- Severe preeclampsia / gestational hypertension
- Hemorrhage / placental abruption
- Chorioamnionitis (infection)
- Significant maternal cardiac disease
- Puerperal infection
Fetal contraindications:
- Fetal distress / low BPP
- Intrauterine fetal death
- Lethal fetal anomaly
- Gestational age ≥34 weeks (risk of prematurity < risk of tocolysis side effects)
Step 3: Administer Adjunctive Therapies
A. Antenatal Corticosteroids (MOST IMPORTANT)
- Betamethasone 12 mg IM every 24 hours × 2 doses (preferred)
- OR Dexamethasone 6 mg IM every 12 hours × 4 doses
- Indicated for gestational age 24-34 weeks (consider 22-34 weeks in very preterm)
- Benefits: ↓ neonatal death, ↓ RDS, ↓ IVH, ↓ PDA, ↓ NEC
- Mechanism: promotes surfactant synthesis, increases lung compliance, reduces vascular permeability
- Maturational effects on brain, kidneys, and gut also documented
- Creasy & Resnik, p. 898
B. Magnesium Sulfate for Fetal Neuroprotection
- Recommended for anticipated delivery <32 weeks
- Loading dose: 4-6 g IV over 30 minutes, with or without maintenance 1-2 g/hr for 12-24 hours
- Reduces cerebral palsy: RR = 0.68 (95% CI 0.54-0.85) in meta-analysis of 6 trials
- Reduces moderate-to-severe CP: RR = 0.63 (95% CI 0.45-0.89)
- No significant adverse effects on infants at neuroprotective doses
- Creasy & Resnik, p. 901; ACOG recommendation
C. GBS Prophylaxis
- Penicillin or ampicillin IV for all women in preterm labor (preterm infants at higher risk for neonatal GBS)
- Antibiotic therapy to prolong pregnancy is not recommended for preterm labor with intact membranes (unlike pPROM, where antibiotics reduce perinatal morbidity)
Step 4: Tocolysis
Key principle: Tocolytic agents delay delivery by ~48 hours to 7 days in ~80% of women but do not prevent preterm birth or improve ultimate fetal outcomes. Their primary value is to provide a window for corticosteroid administration and maternal transfer to a tertiary center.
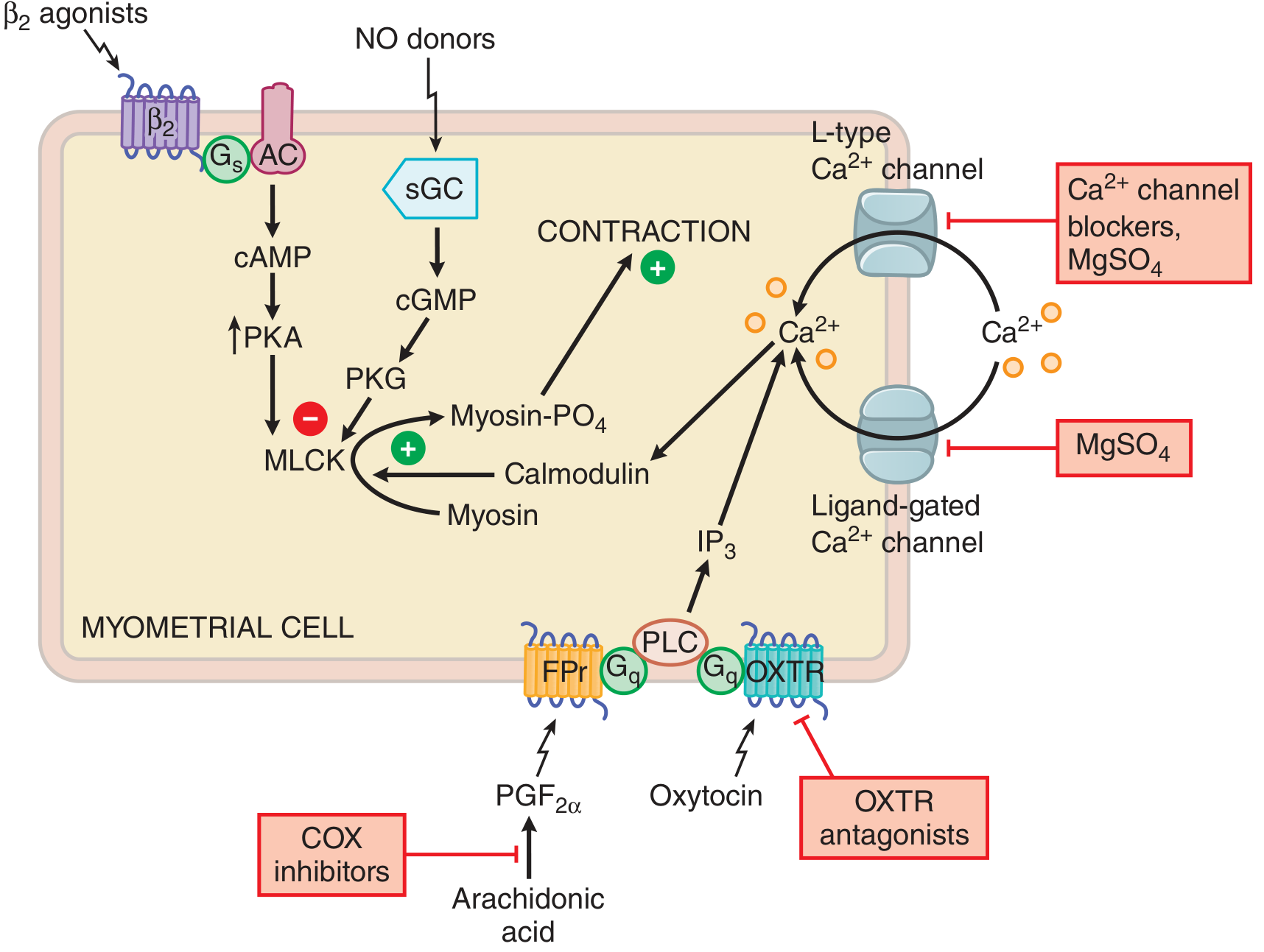
Figure: Sites of action of tocolytic drugs - Goodman & Gilman's Pharmacological Basis of Therapeutics
Tocolytic Agents
| Drug Class | Agent | Mechanism | Efficacy | Key Side Effects |
|---|---|---|---|---|
| Ca²⁺ channel blockers | Nifedipine (preferred first-line) | Blocks L-type voltage-sensitive Ca²⁺ channels → ↓ MLCK activation | Delays delivery 48h; fewer maternal side effects than β-agonists | Headache, flushing, hypotension |
| β₂-adrenergic agonists | Terbutaline, ritodrine | β₂ receptor → ↑ cAMP → PKA → inactivates MLCK → relaxation | Delays delivery 48h-7 days; only ritodrine FDA-approved (withdrawn) | Tachycardia, hypotension, pulmonary edema, hyperglycemia |
| COX inhibitors | Indomethacin | Inhibit COX → ↓ PGF₂α/PGE₂ → ↓ uterotonic stimulus | Some evidence for ↓ preterm births | Premature ductal arteriosus closure (avoid >32 weeks), oligohydramnios; use <72h |
| Oxytocin receptor antagonists | Atosiban | Blocks oxytocin (OXTR) receptor | Widely used in Europe (not FDA-approved in US); Cochrane: may be ineffective | Injection site reaction, concern about neonatal outcomes |
| MgSO₄ | Magnesium sulfate | Competes with Ca²⁺; inhibits voltage-gated Ca²⁺ channels | Cochrane: may be ineffective as tocolytic per se; used for neuroprotection | Respiratory depression (toxicity), flushing, loss of DTRs |
| NO donors | Nitroglycerin (transdermal) | ↑ cGMP → PKG → inactivates MLCK | Limited data; one trial showed ↓ neonatal morbidity before 28 weeks | Headache, hypotension |
No tocolytic agent has been shown to definitively improve fetal outcome. Choice of agent is less important than patient selection. - Creasy & Resnik, p. 901
Prevention
1. Progesterone Therapy
- Vaginal progesterone 200 mg nightly: reduces preterm birth in women with mid-trimester cervical shortening (CL <25 mm by ultrasound) - most evidence-based preventive therapy
- 17-hydroxyprogesterone caproate (17-OHPC) 250 mg IM weekly: historically used for women with prior spontaneous preterm singleton birth; the PROLONG trial (2020) showed no benefit vs placebo, casting doubt on this indication
- Mechanism: inhibits proinflammatory cytokines, delays cervical ripening
- Role in multiple gestations remains controversial (meta-analyses show no benefit)
2. Cervical Cerclage
- Indicated for documented cervical insufficiency (painless cervical dilation <24 weeks)
- History-indicated cerclage: prior second-trimester loss with painless dilation
- Ultrasound-indicated: cervical length <25 mm before 24 weeks in singleton with prior preterm birth
- Not beneficial in multiple gestations (meta-analyses show no benefit)
3. Cervical Pessary
- Silicone ring placed around cervix to redirect uterine weight
- Meta-analyses: no significant benefit in multiple gestations or unselected populations
4. Education and Surveillance
- Instruct high-risk women on symptoms of preterm labor
- More frequent prenatal visits
- Transvaginal cervical length screening at 18-24 weeks
Regionalized Care
Hospitals are designated:
- Level I: Normal obstetric/neonatal care
- Level II: NICU for infants >1500 g
- Level III: Sickest/smallest infants; complex maternal complications
- Level IV: ECMO, complex cardiothoracic surgery
Transfer to a regional center before delivery is preferred when preterm delivery is anticipated. - Creasy & Resnik, p. 897
Fetal Complications of Prematurity
| Problem | Mechanism |
|---|---|
| Respiratory distress syndrome (RDS) | Surfactant deficiency |
| Intraventricular hemorrhage (IVH) | Fragile germinal matrix vasculature |
| Necrotizing enterocolitis (NEC) | Immature gut mucosal immunity |
| Patent ductus arteriosus (PDA) | Failure of ductal closure |
| Cerebral palsy | Brain injury from IVH, ischemia, infection |
| Retinopathy of prematurity | Abnormal retinal vascularization |
| Sepsis | Immature immune system |
Key Summary Points
- Preterm labor = contractions + cervical change before 37 weeks
- Diagnosis is challenging; overdiagnosis in 40-70% - use TVU cervical length + fFN to avoid unnecessary treatment
- Negative fFN = no delivery for ≥7-10 days (excellent NPV); most useful to rule out preterm labor
- Tocolytics (nifedipine first-line) delay delivery 48 hours - do not reduce preterm birth rates; their purpose is to allow corticosteroids and transfer
- Antenatal corticosteroids (betamethasone 24-34 weeks) are the single most important intervention - reduce RDS, IVH, NEC, and neonatal death
- MgSO₄ before 32 weeks for fetal neuroprotection - reduces cerebral palsy by ~32%
- Vaginal progesterone for women with short cervix (<25 mm) is the best-evidenced preventive strategy
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Ch. 38
- Goodman & Gilman's The Pharmacological Basis of Therapeutics 14e, Ch. 48
- Textbook of Family Medicine 9e, Ch. 20
- Pfenninger and Fowler's Procedures for Primary Care 3e
- Morgan and Mikhail's Clinical Anesthesiology 7e, Ch. 6
This is a shared conversation. Sign in to Orris to start your own chat.