MANAGEMENT of status epilepyicus
Reading File
Finding Sources
Searching PubMed
"status epilepticus" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have very comprehensive content from multiple authoritative textbooks. Let me compile the full, well-structured answer.
Management of Status Epilepticus (SE)
Definition
Status epilepticus is defined as:
- A single seizure lasting ≥5 minutes, OR
- Two or more seizures without recovery of consciousness between them
After 5 minutes, seizures rarely terminate spontaneously, are less responsive to antiepileptic drugs, and begin causing neuronal damage. Treatment must begin at the 5-minute mark - do not wait for 30 minutes.
- Focal impaired awareness SE: diagnosis at 10 minutes
- Long-term neuronal injury threshold: ~30 min (convulsive) / ~60 min (focal)
(Goldman-Cecil Medicine, Tintinalli's Emergency Medicine, Katzung's Pharmacology)
Classification
| Type | Features |
|---|---|
| Generalized convulsive SE | Prominent tonic-clonic motor activity, impaired consciousness - most dangerous |
| Nonconvulsive SE (NCSE) | Persistent behavioral/cognitive change, continuous epileptiform EEG, no major motor signs; includes absence SE, focal SE, NCSE in coma |
| Refractory SE | Seizures persist after adequate first-line AND second-line treatment (20-30% of cases) |
| Super-refractory SE | Seizures persist/recur after ≥24 hours of third-line therapy |
Common Causes (MNEMONIC: SEAT)
- Subtherapeutic antiepileptic drug levels
- Electrolyte/metabolic abnormalities (glucose, Na, Ca, Mg), anoxia, hypoxia
- Acute CNS insult - stroke, infection, trauma, autoimmune encephalitis (most common cause in one study), posterior reversible encephalopathy syndrome (PRES)
- Toxic - alcohol/drug intoxication or withdrawal
Management Protocol
The management is time-critical and proceeds in three phases:
PHASE 1 - Stabilization (0-5 minutes)
Simultaneously with any seizure activity:
- Airway, Breathing, Circulation (ABCs) - position to maximize ventilation, prevent aspiration
- Administer oxygen (nasal cannula or face mask)
- Large-bore IV access (or IO if IV cannot be established)
- Cardiac monitor, pulse oximetry, end-tidal capnography
- Point-of-care glucose - give IV dextrose if hypoglycemic (give thiamine 100 mg IV first if alcoholism suspected)
- Normal saline IV fluid (avoid glucose-containing solutions - phenytoin incompatible)
- Blood samples: electrolytes, glucose, calcium, magnesium, renal function, liver function, CBC, antiepileptic drug levels (when indicated), urine toxicology
- Treat hyperthermia with antipyretics and cooling blankets
- Correct metabolic abnormalities
Important: Delays in benzodiazepine initiation >10 minutes are associated with higher mortality, longer seizure duration, and more complications.
PHASE 2 - Active/Established SE: First-Line Treatment (5-30 minutes)
Benzodiazepines are the first-line drugs - terminate seizures ~70% of the time.
| Drug | Route | Adult Dose | Notes |
|---|---|---|---|
| Lorazepam | IV | 0.1 mg/kg (2-4 mg) at 2 mg/min | Preferred IV agent; longer duration than diazepam due to less peripheral redistribution |
| Diazepam | IV | 5-10 mg bolus at 5 mg/min; up to 20 mg total | Rapid CNS entry but shorter effective duration |
| Midazolam | IM | 10 mg IM | Preferred if NO IV access; shown non-inferior to IV lorazepam in prehospital setting |
| Diazepam | Rectal | 0.5 mg/kg | Prehospital/home use |
| Midazolam | Intranasal/buccal | Weight-based (see pediatric dosing) | Acceptable if IV/IO unavailable |
Protocol note: Give a second benzodiazepine dose only after 5 minutes of continued seizure. Consider a third benzodiazepine dose and simultaneously begin loading a second-line agent if seizure persists 5 minutes after the second dose.
PHASE 2b - Established SE: Second-Line Treatment (concurrent with benzodiazepines or if benzodiazepines fail)
Three options are equally effective (~45-50% cessation after benzodiazepine failure):
| Drug | Dose | Rate | Notes |
|---|---|---|---|
| Fosphenytoin (preferred over phenytoin) | 15-20 mg PE/kg IV | 150 mg PE/min | Water-soluble; can give IM; less cardiotoxic than phenytoin; given as phenytoin equivalents (PE) |
| Levetiracetam | 30-60 mg/kg (or 2000-4500 mg) IV over 10 min | Rapid infusion | Favorable safety profile; no drug interactions; no hepatic monitoring needed |
| Valproic acid | 30-40 mg/kg at 5 mg/kg/min | Contraindicated in liver disease, thrombocytopenia, possible metabolic disease, pregnancy (1st trimester) | |
| Phenytoin (if fosphenytoin unavailable) | 20 mg/kg IV | 50 mg/min | Must use NS (incompatible with dextrose); cardiotoxic risk; ECG monitoring required |
| Lacosamide | IV loading dose | Alternative second-line; ECG monitoring needed (risk of arrhythmia) | |
| Phenobarbital | 10 mg/kg at 100 mg/min | Highly effective but prolonged sedation, respiratory depression, hypotension |
Consider endotracheal intubation for airway protection at this stage. Use a short-acting paralytic (succinylcholine preferred) - avoid long-acting paralytics as they mask ongoing seizure activity. Arrange continuous EEG monitoring if paralytics are used.
PHASE 3 - Refractory SE: Third-Line Treatment (>30 minutes, or failed 1st + 2nd line)
Requires ICU admission, intubation, ventilation, and continuous EEG monitoring.
Goal: Suppress epileptiform EEG activity (burst suppression pattern).
| Drug | Dose |
|---|---|
| Midazolam (most commonly used) | Load 0.2 mg/kg IV, then infusion 0.05-2 mg/kg/hr |
| Propofol | 1 mg/kg IV bolus, then 1-10 mg/kg/hr infusion |
| Phenobarbital | 20 mg/kg at 50-75 mg/min |
| Ketamine | 5 mg/kg/hr infusion (or 2.2 mg/kg/hr); emerging evidence, useful especially in pediatric refractory SE |
| Pentobarbital/Thiopental | 0.5-3 mg/kg/hr (pentobarbital); 3-5 mg/kg/hr (thiopental) |
(Tintinalli's Emergency Medicine, Miller's Anesthesia, Goldman-Cecil Medicine)
PHASE 4 - Super-Refractory SE (seizures >24 hours despite 3rd-line therapy)
Options with limited but growing evidence:
- Inhaled anesthetics (isoflurane, desflurane)
- Ketamine (NMDA antagonist - mechanistically attractive as glutamate receptors upregulate in prolonged SE)
- Vagal nerve stimulation (VNS)
- Electroconvulsive therapy (ECT)
- Surgical resection (systematic review PMID 38456595 supports surgical management in select refractory cases)
- Evaluation for rare/treatable etiologies (autoimmune encephalitis - NMDA receptor antibody, etc.)
- Transfer to specialized epilepsy center with continuous EEG capability
Management Flowchart
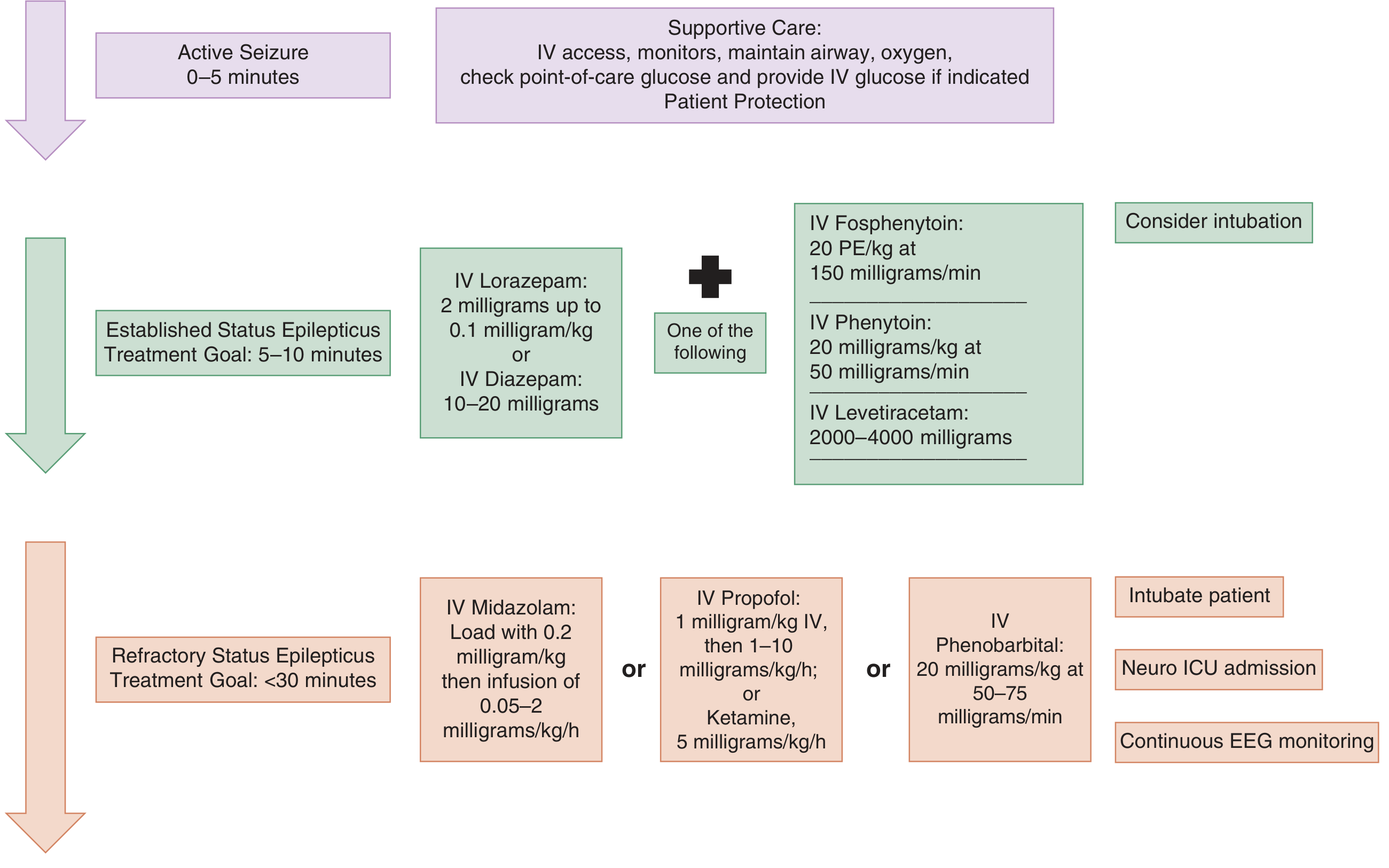
Figure: Three-phase treatment protocol from Tintinalli's Emergency Medicine
Nonconvulsive SE - Special Considerations
- Diagnosis confirmed by EEG (mandatory)
- Clinical clues: prolonged postictal state, subtle twitching/eye deviation/blinking, fluctuating altered mental status, unexplained stupor/coma
- Less urgency than convulsive SE; treatment can be initiated more cautiously with lower doses
- Must suspect in any comatose patient without explanation - begin continuous EEG monitoring
Systemic Complications to Monitor
| Complication | Action |
|---|---|
| Hypoxic respiratory failure / acidosis | Early airway management |
| Hypoglycemia or hyperglycemia | Glucose monitoring and correction |
| Hyperthermia | Antipyretics + cooling blanket |
| Rhabdomyolysis | Monitor CK, urine output, renal function |
| Cardiac arrhythmias / hypotension | Continuous cardiac monitoring, vasopressors if needed |
| Aspiration / pulmonary edema | Respiratory support |
| Raised ICP | Elevate head of bed 30°, treat underlying cause |
(Miller's Anesthesia, Rosen's Emergency Medicine)
Pediatric Considerations (Harriet Lane Handbook)
| Drug | Age | Dose |
|---|---|---|
| Diazepam IV | <5 yr | 0.2-0.5 mg/dose Q2-5 min; max 5 mg |
| Diazepam IV | ≥5 yr | 1 mg/dose Q2-5 min; max 10 mg |
| Diazepam rectal | Any | 0.5 mg/kg then 0.25 mg/kg in 10 min PRN |
| Midazolam IN | 6-11 yr | 0.3 mg/kg/dose (weight-based table) |
| Midazolam IN | ≥12 yr | 0.2 mg/kg/dose (weight-based table) |
| Ketamine infusion | Pediatric | Supported by 2024 systematic review (PMID 38881333) |
Recent Evidence Updates (2024-2026)
- A 2024 systematic review of clinical practice guidelines (Vignatelli et al., Epilepsia 2024) confirmed the three-phase treatment approach and highlighted significant variability in guideline recommendations internationally, especially for second-line agents - levetiracetam, valproate, and fosphenytoin remain equally recommended.
- A 2024 meta-analysis on ketamine in pediatric SE (Epilepsia 2024) supports ketamine as a viable option in refractory pediatric SE.
- A 2026 systematic review on brivaracetam for SE (J Neurol 2026) suggests brivaracetam may be a promising second- or third-line IV option, though routine use is not yet established.
Summary: Time-Action Table
| Time | Phase | Action |
|---|---|---|
| 0-5 min | Pre-treatment | ABCs, IV/IO access, glucose check, labs, monitors |
| 5-10 min | 1st line | Benzodiazepine IV (lorazepam 0.1 mg/kg or diazepam 10-20 mg); IM midazolam 10 mg if no IV |
| 10-30 min | 2nd line | Fosphenytoin 20 PE/kg OR levetiracetam 2000-4500 mg OR valproate 30-40 mg/kg; consider intubation |
| >30 min | 3rd line (Refractory) | Intubate + ICU; midazolam/propofol/pentobarbital continuous infusion + EEG monitoring |
| >24 hr | Super-refractory | Ketamine, inhaled anesthetics, VNS, ECT; workup rare etiologies |
Sources: Tintinalli's Emergency Medicine (9780323757898) - Rosen's Emergency Medicine (9781260019933) - Miller's Anesthesia 10e (9780323935920) - Goldman-Cecil Medicine (9780323930345) - Katzung's Pharmacology 16e (9781260463309) - Harriet Lane Handbook 23e (9780323876988)
This is a shared conversation. Sign in to Orris to start your own chat.