CTG
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiotocography" AND "fetal monitoring"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer on CTG (Cardiotocography).
Cardiotocography (CTG)
CTG is the simultaneous, continuous electronic recording of the fetal heart rate (FHR) and uterine contractions. It is the cornerstone of intrapartum fetal monitoring and relies on the coupling of fetal neurologic status to cardiovascular reflex responses.
How the CTG Machine Works
The monitor has two components:
1. Fetal Heart Rate Detection
- Fetal scalp electrode (internal): A small spiral stainless steel wire attached to the fetal scalp detects the R wave of the fetal ECG. This is the most accurate method as it measures true beat-to-beat variability directly.
- Doppler ultrasound transducer (external / cardiotachometer): Emits ~2.5 MHz ultrasound, picks up movement from cardiac structures, and calculates intervals between beats. Uses autocorrelation to improve accuracy. Can be affected by maternal/fetal movement and maternal body habitus.
2. Uterine Contraction Detection
- Intrauterine pressure catheter (IUPC): Soft plastic catheter placed transcervically into the amniotic cavity. Measures true contraction intensity in mmHg.
- Tocodynamometer (external): Placed on the maternal abdomen over the fundus. Detects frequency and duration of contractions but not intensity.
The Four Key Features of a CTG Trace
| Feature | What to Assess |
|---|---|
| Baseline FHR | Mean rate over 10 minutes, excluding accelerations/decelerations |
| Variability | Amplitude of fluctuations in FHR between beats |
| Accelerations | Transient rises in FHR |
| Decelerations | Transient falls in FHR - early, late, variable, prolonged |
1. Baseline FHR
- Normal: 110-160 beats/min
- Bradycardia: <110 beats/min
- Tachycardia: >160 beats/min
- Changes within the normal range during labor are common and not predictive of neonatal morbidity.
2. Baseline Variability
Reflects the amplitude of FHR fluctuations:
- Absent: Amplitude undetectable
- Minimal: >0 but ≤5 beats/min
- Moderate (normal): 6-25 beats/min
- Marked: >25 beats/min
Normal FHR variability predicts a fetal CNS that is normally interacting with the fetal heart. It is the most reliable indicator of current fetal oxygenation.
3. Accelerations
- Definition: Abrupt rise (<30 seconds onset to peak) of ≥15 beats/min above baseline, lasting 15 seconds to 2 minutes.
- In fetuses <32 weeks, 10 beats/min rise lasting 10 seconds is acceptable.
- Presence of an acceleration is almost always indicative of the absence of fetal acidemia at that moment.
- The Nonstress Test (NST) is considered reactive when ≥2 such accelerations occur in 20-30 minutes.
4. Decelerations
| Type | Timing relative to contraction | Mechanism | Significance |
|---|---|---|---|
| Early | Mirrors contraction (simultaneous onset/nadir) | Fetal head compression → vagal reflex | Benign |
| Late | Nadir after peak of contraction (lag ≥30 sec) | Uteroplacental insufficiency → hypoxia | Pathological |
| Variable | Variable timing, abrupt onset (<30 sec) | Umbilical cord compression | Severity depends on depth/duration |
| Prolonged | Lasts 2-10 minutes | Same as late/variable mechanisms | Concerning if recurring |
A sinusoidal pattern is a distinct finding: smooth sine-wave baseline at 3-6 cycles/min, amplitude up to 30 beats/min, lasting ≥20 minutes, with absent beat-to-beat variability. It is classically associated with severe fetal anemia (Rh alloimmunization, fetomaternal hemorrhage) and requires urgent intervention.
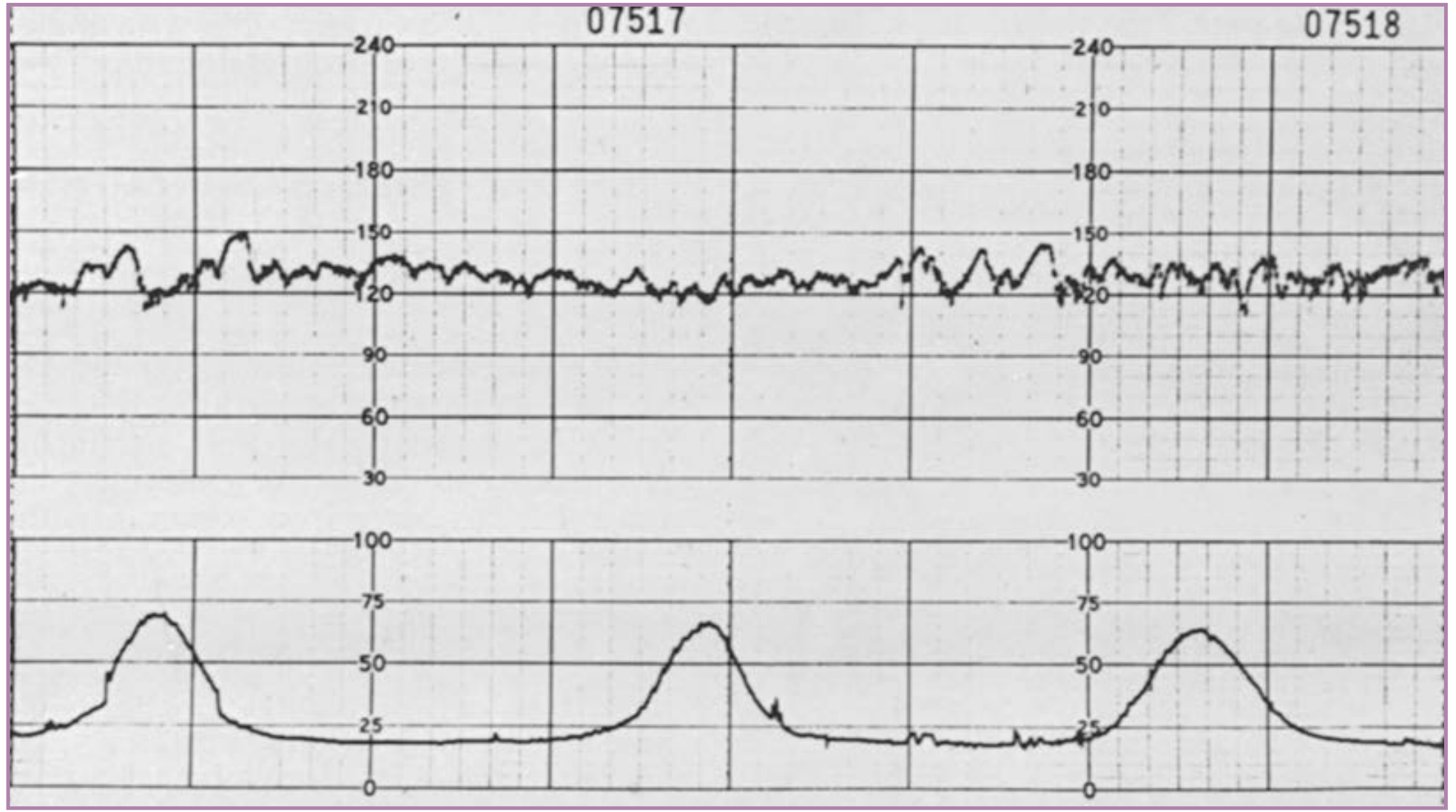
Here is what a normal CTG looks like - baseline ~130 bpm with good variability and uterine contractions visible in the lower channel:
NICHD Three-Tier Classification System (2008)
The NICHD/ACOG three-tiered system is the standard for FHR pattern categorization:
Category I - Normal (Reassuring)
ALL of the following must be present:
- Baseline rate: 110-160 beats/min
- Baseline variability: moderate
- Late or variable decelerations: absent
- Early decelerations: present or absent
- Accelerations: present or absent
Action: Routine monitoring. Strongly predictive of normal fetal acid-base status.
Category II - Indeterminate
All tracings not Category I or III. Includes:
- Bradycardia without absent variability, or tachycardia
- Minimal, absent (without recurrent decelerations), or marked variability
- No accelerations after fetal stimulation
- Recurrent variable decelerations with minimal/moderate variability
- Prolonged decelerations (2-10 min)
- Recurrent late decelerations with moderate variability
- Variable decelerations with slow return to baseline, overshoots, or shoulders
Action: Continuous surveillance, consider corrective measures, escalate if no improvement.
Category III - Abnormal (Non-reassuring)
Either:
- Absent variability + recurrent late decelerations, recurrent variable decelerations, OR bradycardia
- Sinusoidal pattern
Action: Expedited evaluation and delivery. Associated with fetal acidemia.
Fetal Physiology Underlying CTG Changes
During acute hypoxia or acidemia, the fetus initially redistributes blood flow to vital organs (heart, brain, adrenals) - a compensatory "diving reflex." This is reflected in FHR changes:
- Mild hypoxia: late decelerations via chemoreflex (vagal)
- Moderate-severe/prolonged hypoxia: myocardial depression, absent variability, bradycardia
The FHR is the most sensitive short-term predictor of worsening fetal hypoxemia or acidosis.
Corrective Maneuvers for Abnormal Patterns
| Cause | FHR Pattern | Corrective Action |
|---|---|---|
| Maternal hypotension | Bradycardia, late decelerations | IV fluids, lateral position, ephedrine |
| Cord compression | Variable decelerations | Position change (left/right lateral, Trendelenburg) |
| Excessive uterine activity | Bradycardia, late decelerations | Reduce/stop oxytocin, lateral position |
| Head compression | Early or variable decelerations | Amnioinfusion |
| Prolonged asphyxia | Decreased variability, late decelerations | Delivery |
Adjuncts to CTG
- Fetal scalp stimulation / acoustic stimulation: Absence of FHR acceleration after stimulation = Category II finding
- Fetal scalp blood sampling (pH/lactate): Rarely used in the US; useful in ambiguous Category II traces
- Fetal pulse oximetry: Can detect fetal SpO2 but not widely adopted
- Umbilical cord blood gas analysis: Post-delivery objective assessment; umbilical artery pH <7.10 with metabolic acidosis = significant birth asphyxia
Limitations of CTG
Intrapartum CTG has high sensitivity but low specificity for fetal acidemia - it over-predicts compromise, leading to increased cesarean section rates. The combination with biophysical profile (BPP) assessment or adjunctive testing improves specificity.
A 2026 systematic review and meta-analysis in BJOG (PMID: 41074594) reassessed the value of admission CTG in term pregnancies, reflecting ongoing debate about its routine use.
Sources: Creasy & Resnik's Maternal-Fetal Medicine, 9th ed.; Miller's Anesthesia, 10th ed.; Barash, Cullen & Stoelting's Clinical Anesthesia, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.