Teratomas
Reading File
Finding Sources
Finding Sources
Searching PubMed
teratoma pathology classification
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to write a thorough overview. Let me compile everything.
Teratomas
Teratomas are germ cell tumors (GCTs) that contain elements derived from at least two — and usually all three — embryonic germ cell layers (ectoderm, mesoderm, endoderm). The name derives from the Greek teras ("monster"), reflecting their bizarre admixture of tissues such as hair, teeth, cartilage, and neural tissue within a single mass.
Classification
Teratomas are divided into three major categories:
1. Mature (Benign) Teratomas
The most common type. Usually cystic and commonly called dermoid cysts, because the lining is predominantly skin-like (squamous epithelium, sebaceous glands, hair follicles). Characteristics:
- Found chiefly in young adult females (ovarian location)
- Bilateral in 10–15% of ovarian cases
- Cyst wall contains hair, sebum, teeth, bone, cartilage, thyroid, neural tissue
- Karyotype: 46,XX; most arise from an ovum after the first meiotic division
- ~1% undergo malignant transformation, most commonly to squamous cell carcinoma
- May cause paraneoplastic syndromes — notably anti-NMDAR encephalitis (inflammatory limbic encephalitis), which can remit after tumor removal
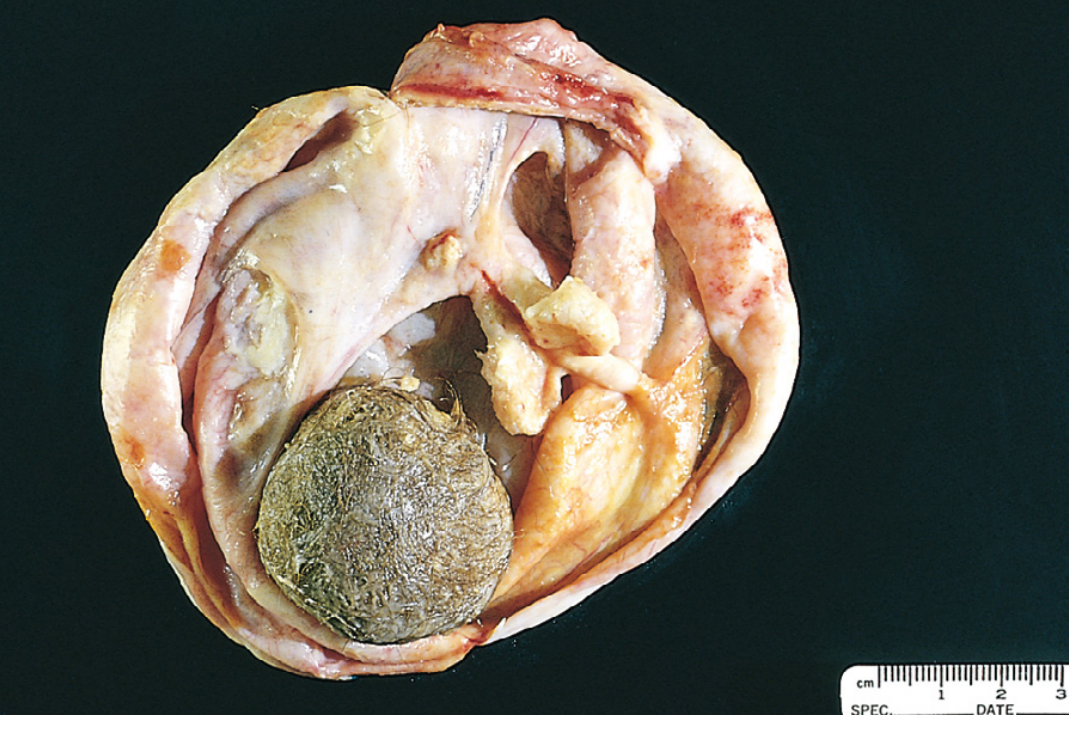
Gross appearance: Unilocular cyst filled with sebaceous material and hair:
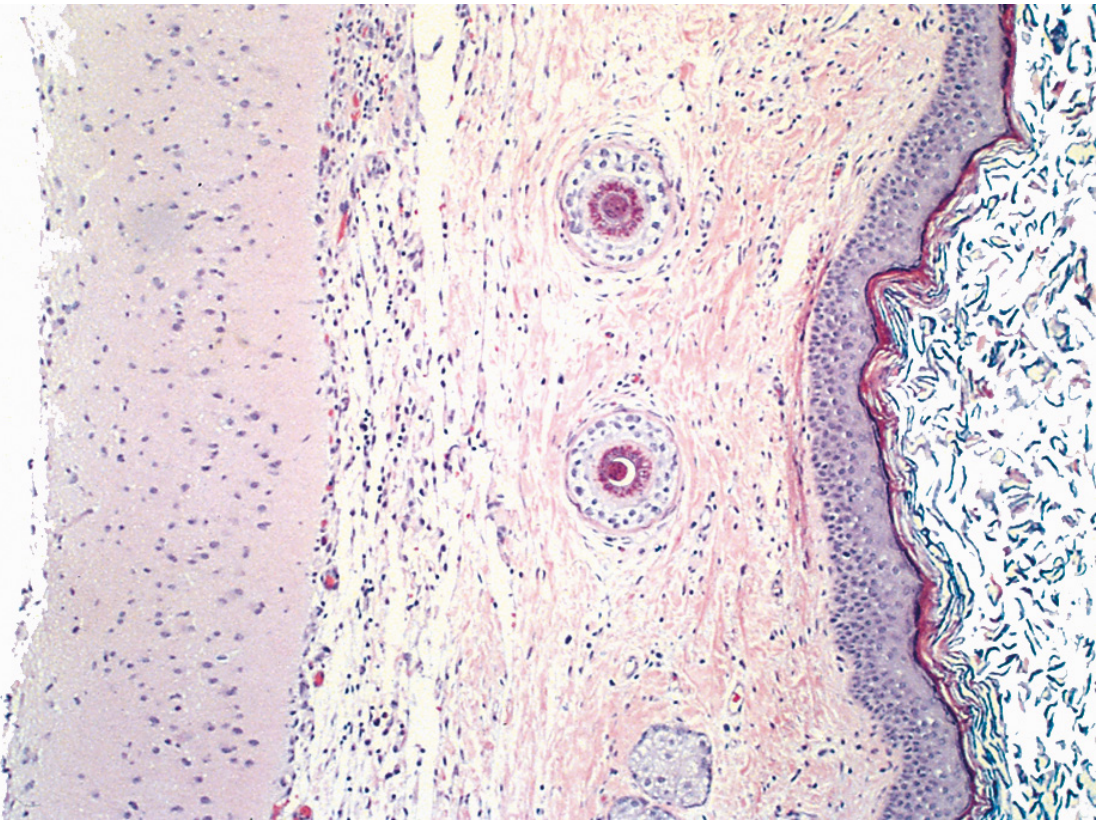
Histology: Stratified squamous epithelium with hair shafts and sebaceous glands, with brain tissue from other germ layers:
2. Immature (Malignant) Teratomas
Rare tumors where the component tissues resemble embryonal or fetal tissue rather than mature structures.
- Found chiefly in prepubertal adolescents and young females (mean age ~18 years)
- Macroscopically: bulky, solid, with hair, sebaceous material, areas of necrosis and hemorrhage
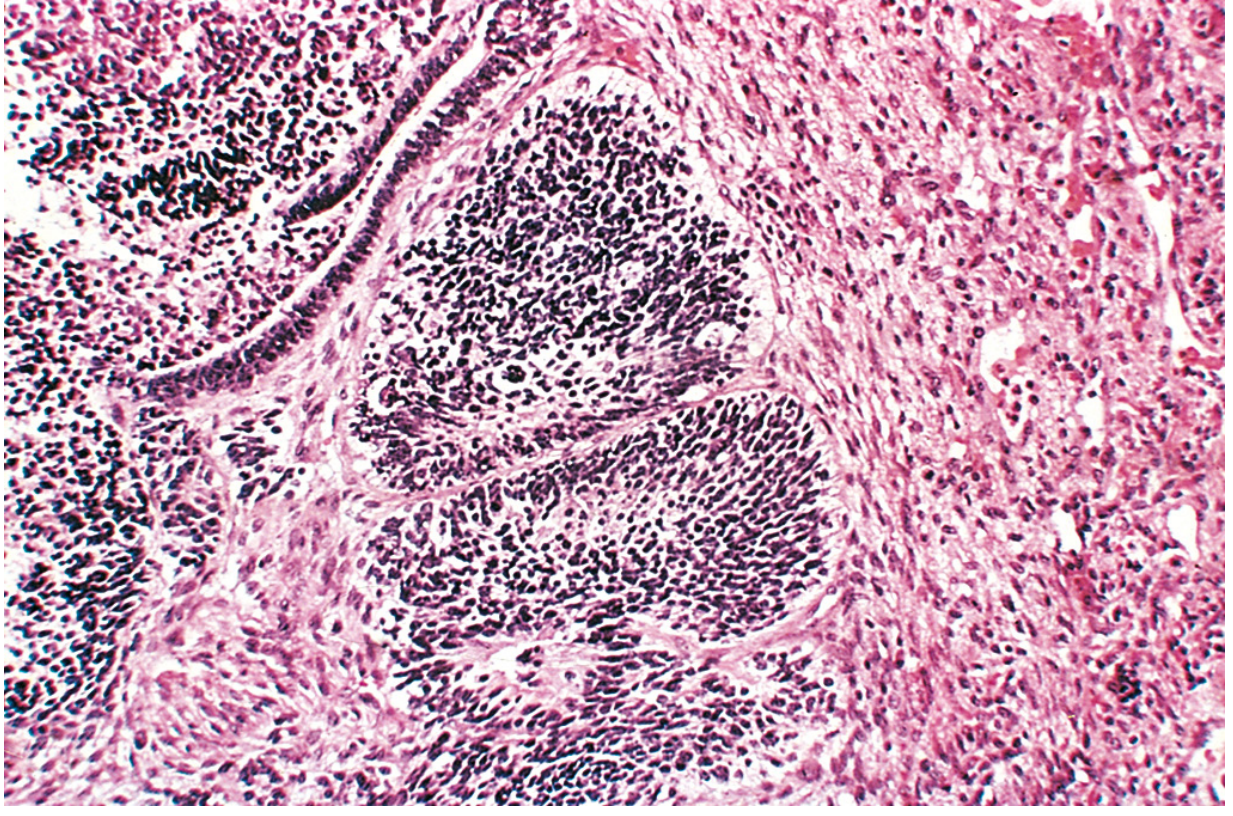
- Microscopically: contains immature neuroepithelium — the proportion of which determines histologic grade I–III
- Grade drives prognosis: Stage I, Grade 1 → excellent prognosis; Grade 2–3 → adjuvant chemotherapy
- Most recurrences occur within the first 2 years
Histology (primitive neuroepithelium):
3. Monodermal (Specialized) Teratomas
A rare group derived from only one germ layer or a specialized tissue type. Always unilateral. Key subtypes:
| Subtype | Tissue | Notes |
|---|---|---|
| Struma ovarii | Mature thyroid | Can cause hyperthyroidism |
| Ovarian carcinoid | Intestinal neuroendocrine | Can produce serotonin → carcinoid syndrome even without hepatic mets (ovarian veins → systemic) |
| Strumal carcinoid | Thyroid + carcinoid | Extremely rare combination |
Only ~2% of carcinoids arising in teratomas metastasize.
Sites & Location-Specific Features
Ovary (most common site in females)
The most common location for teratomas overall. Pure mature cystic teratomas are benign; ~1% undergo malignant transformation.
Testis (males)
- In adults: teratoma is histologically benign-appearing but clinically malignant — it is resistant to chemotherapy and frequently found at metastatic sites in NSGCT
- ~47% of mixed GCTs contain teratoma; pure testicular teratomas are uncommon
- Contains genetic hallmarks of malignancy: aneuploidy, isochromosome 12p [i(12p)]
- Can grow uncontrollably (growing teratoma syndrome), transform into somatic malignancies (rhabdomyosarcoma, adenocarcinoma, PNET) — termed "teratoma with somatic-type malignancy" — aggressive, chemo-resistant, poor prognosis
- In prepubertal boys: pure teratoma IS benign (different biology — no i[12p])
- Management: Residual masses after chemotherapy for NSGCT require surgical resection (retroperitoneal lymph node dissection), since teratoma is chemo-resistant and untreated teratoma → late relapse
Mediastinum (anterior)
- Commonest site for extragonadal GCTs
- CT: well-defined anterior mediastinal mass with mixed density — fat + fluid + soft tissue + calcification
- MRI: fat appears as high T1 with signal drop on fat-saturation; cysts are low T1/high T2; fat signal is virtually diagnostic of teratoma
- Differentiates from thymoma/lymphoma by fat content on MRI
Sacrococcygeal Teratoma
- Most common congenital neoplasm
- Associated with significant neurourologic dysfunction
- Urologic complications in ~33%: neurogenic bladder, urinary incontinence, vesicoureteral reflux
- Prenatal hydronephrosis on imaging significantly predicts urologic sequelae
- Altman classification (I–IV) based on external vs. presacral component
CNS / Pineal Teratomas
- WHO classifies CNS teratomas as: mature teratoma, immature teratoma, and teratoma with somatic-type malignancy
- Located classically in the pineal region
- A clear distinction from hamartomas can be difficult in some pineal teratomas
Pathogenesis
- Most teratomas arise from primordial germ cells that fail to migrate properly during embryogenesis
- Genetic analyses of ovarian teratomas: majority arise from an ovum after the first meiotic division; minority arise before it
- In testicular teratomas: hallmark genetic change is i(12p) — isochromosome 12p — confirming GCT origin even when histologically benign
Tumor Markers
| Marker | Relevance |
|---|---|
| AFP | Usually normal; mildly elevated in some teratomas (cystic fluid contains AFP) |
| β-hCG | Negative in pure teratoma |
| LDH | Nonspecific |
Absence of marker elevation does not exclude teratoma; teratoma is a marker-negative GCT element.
Key Clinical Points
- Testicular teratoma in adults: surgical resection is mandatory — chemo-resistance means chemotherapy alone is insufficient
- Expert pathology review is critical for GCTs: one study showed 31% discrepancy in histologic subtype between community and expert (Indiana University) pathologists
- Anti-NMDAR encephalitis associated with mature ovarian teratoma → oophorectomy is part of treatment
- Sacrococcygeal teratoma → long-term urologic follow-up required
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Campbell-Walsh-Wein Urology; Grainger & Allison's Diagnostic Radiology; Adams & Victor's Principles of Neurology; Sabiston Textbook of Surgery
Pluripotent
Finding Sources
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.