corpulmonale
Reading File
Finding Sources
Searching PubMed
"cor pulmonale" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of cor pulmonale based on Fuster and Hurst's The Heart (15th Ed.), Robbins & Kumar Basic Pathology, and Fishman's Pulmonary Diseases and Disorders.
Cor Pulmonale
Definition
Cor pulmonale is right ventricular hypertrophy and dilation — frequently accompanied by right-sided heart failure — caused by pulmonary hypertension due to primary disorders of the lung parenchyma or pulmonary vasculature. RV dysfunction caused by left ventricular failure or congenital heart disease is excluded by definition.
Pathogenesis
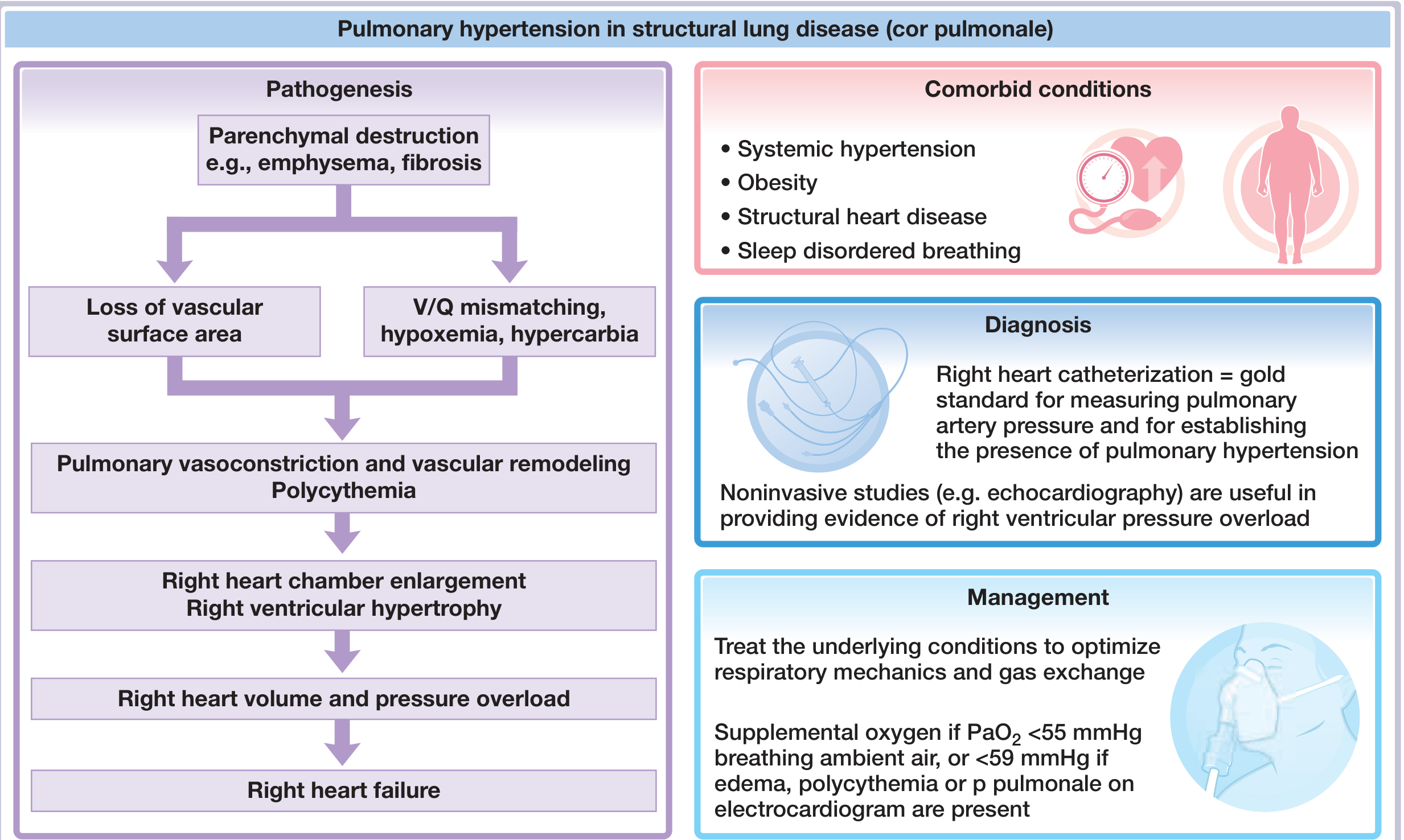
The cascade proceeds as follows:
- Parenchymal destruction (emphysema, fibrosis) → loss of pulmonary vascular surface area
- V/Q mismatch → hypoxemia ± hypercarbia
- Hypoxic pulmonary vasoconstriction + vascular remodeling → pulmonary hypertension
- Polycythemia (hypoxia-driven erythropoiesis) → increased blood viscosity → further ↑ PVR
- RV pressure overload → RV hypertrophy → dilation → right heart failure
Causes
| Category | Examples |
|---|---|
| Obstructive lung disease | COPD, bronchiolitis, emphysema |
| Restrictive lung disease | Interstitial fibrosis, pulmonary fibrosis |
| Mixed obstructive/restrictive | Cystic fibrosis, combined pulmonary fibrosis and emphysema (CPFE) |
| Hypoventilation syndromes | Sleep-disordered breathing, obesity hypoventilation |
| Neuromuscular/mechanical | Kyphoscoliosis |
| Pulmonary vascular | Chronic thromboembolic PH (CTEPH) |
COPD from smoking is the most common cause worldwide.
Acute vs. Chronic
| Feature | Acute Cor Pulmonale | Chronic Cor Pulmonale |
|---|---|---|
| Onset | Sudden (e.g., massive PE) | Insidious |
| Morphology | RV dilation only; heart may be normal size in sudden death | RV + RA hypertrophy; wall thickness may equal LV |
| Vascular changes | None | Pulmonary artery intimal thickening |
Morphology (Gross Pathology)
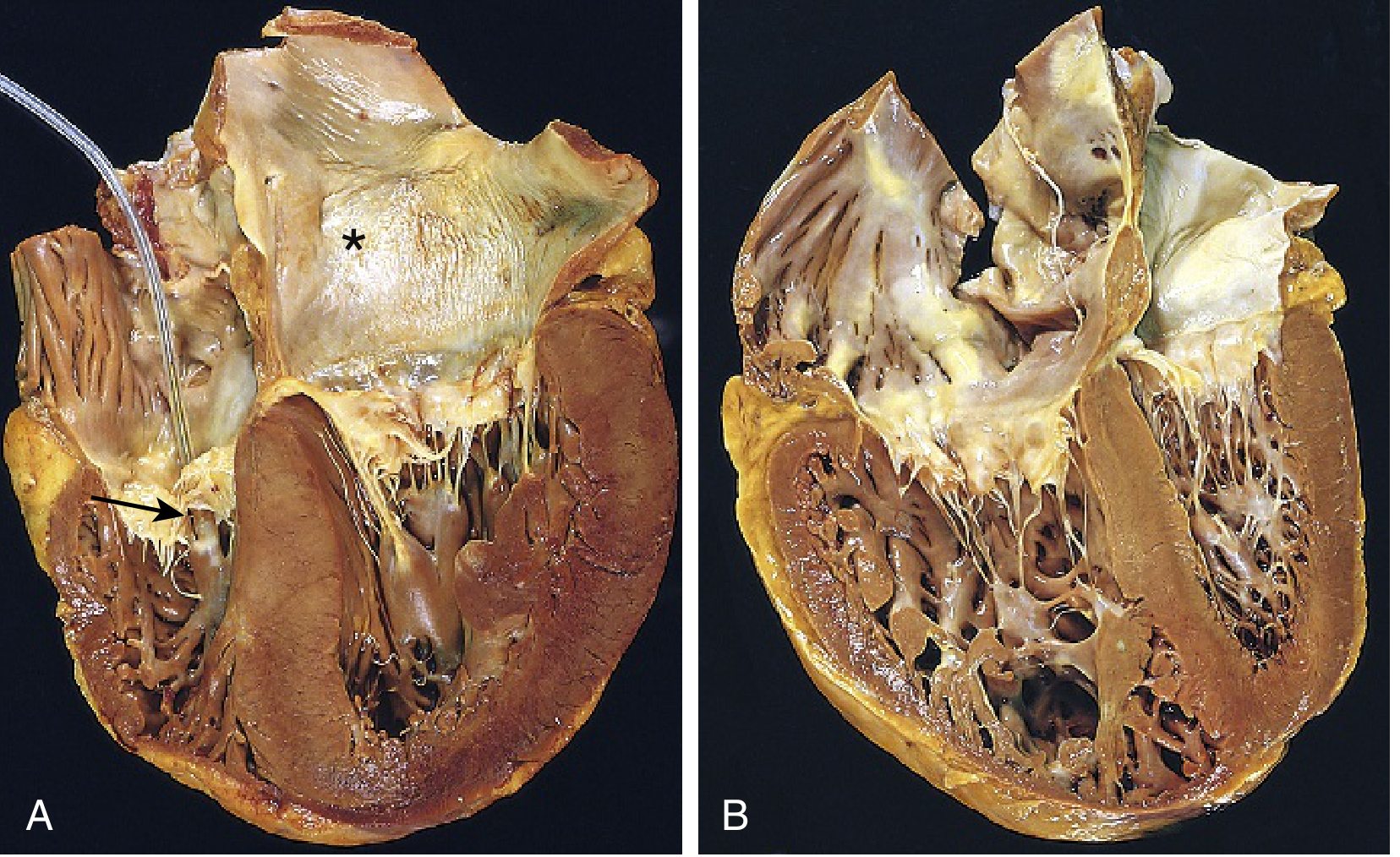
In panel B (chronic cor pulmonale), the right ventricle (left side of image) is markedly dilated and hypertrophied with a thickened free wall and prominent trabeculae. The enlarged RV distorts the shape and volume of the LV. Compare with panel A (left-sided hypertensive heart disease) showing concentric LV thickening.
- Robbins & Kumar Basic Pathology, p. 363
Clinical Manifestations
- Dyspnea on exertion (the dominant symptom)
- Features of right heart failure: peripheral edema, raised JVP, hepatomegaly
- Symptoms of the underlying lung disease (cough, wheeze, orthopnea in COPD)
- Note: Peripheral edema correlates poorly with resting right atrial pressure and may reflect RAAS activation rather than true RV failure
Diagnosis
ECG
- P pulmonale (peaked P waves in lead II)
- Right axis deviation
- RV hypertrophy pattern (R > S in V1, deep S in V5–V6)
- Right bundle branch block
Echocardiography (noninvasive standard)
- RV enlargement and hypertrophy
- ↑ tricuspid regurgitant jet velocity (estimates RVSP)
- Paradoxical septal motion (with severe RV pressure overload)
- ↑ RV/LV ratio and eccentricity index
- TAPSE (tricuspid annular plane systolic excursion): normal ≥16 mm; severe RV dysfunction <10 mm
- Absence of TR jet makes PH unlikely
Chest Radiograph / CT
- Right ventricular enlargement (↑ retrosternal density on lateral CXR)
- Enlarged pulmonary arteries (R PA >16 mm, L PA >18 mm suggests PH)
Right Heart Catheterization (gold standard)
- Directly measures mean pulmonary artery pressure (mPAP ≥25 mmHg at rest = PH)
- Also measures PCWP (to exclude left heart disease as cause)
- Required before starting PAH-targeted therapies
MRI
- Assesses pulmonary arterial stiffness/compliance (altered early in PH)
- Useful for RV function quantification
Prognosis
- Once cor pulmonale is present, survival is significantly reduced
- If mPAP >25 mmHg → average 5-year survival reduced by ~50%
Management
The cornerstone is treating the underlying lung disease and correcting hypoxemia:
| Intervention | Details |
|---|---|
| Supplemental O₂ | Continuous O₂ if PaO₂ <55 mmHg (ambient air), or <59 mmHg if edema, polycythemia, or P pulmonale on ECG present |
| Treat underlying disease | Bronchodilators, corticosteroids, anti-inflammatory agents for COPD/ILD |
| Diuretics | Optimize volume status |
| NIV / nocturnal ventilation | For hypoventilation syndromes, neuromuscular disease, sleep apnea overlap |
| PAH-targeted therapies | Controversial — can worsen V/Q mismatch and hypoxemia; not routinely recommended |
| Calcium channel blockers / vasodilators | Can dilate pulmonary vasculature but worsen hypoxemia; benefit not established in cor pulmonale |
Key point: PAH-specific drugs (prostacyclins, endothelin receptor antagonists, PDE-5 inhibitors) are approved for Group 1 PAH but their role in Group 3 PH (cor pulmonale from lung disease) is controversial and potentially harmful.
Edema in Cor Pulmonale
The mechanism is multifactorial — RAAS activation from reduced cardiac output, hypercapnia-driven renal sodium retention, and elevated right atrial pressure all contribute. Peripheral edema is a late and unreliable sign of right heart failure in this context.
Sources:
- Fuster and Hurst's The Heart, 15th Edition, Ch. 59
- Robbins & Kumar Basic Pathology, p. 363
- Fishman's Pulmonary Diseases and Disorders, p. 734
This is a shared conversation. Sign in to Orris to start your own chat.