Intra operative neuro physiological monitoring ( SSEP / MEP / Wake up test )
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
intraoperative neurophysiological monitoring SSEP MEP wake up test spine surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
intraoperative neurophysiological monitoring SSEP MEP spinal surgery
I now have all the content needed for a comprehensive, well-structured answer. Let me compile it.
Intraoperative Neurophysiological Monitoring (IONM)
Overview
Intraoperative neurophysiological monitoring (IONM) is now considered mandatory for all surgeries in which the spinal cord is at risk of injury - including spinal deformity correction, spinal tumor resection, aortic surgery, and intracranial procedures. The primary goal is rapid identification of surgically induced neurophysiological changes to allow prompt correction before irreversible neurological injury occurs.
The three principal methods of spinal cord monitoring are:
- SSEP - Somatosensory Evoked Potentials
- MEP - Motor Evoked Potentials
- Wake-up Test (Stagnara test)
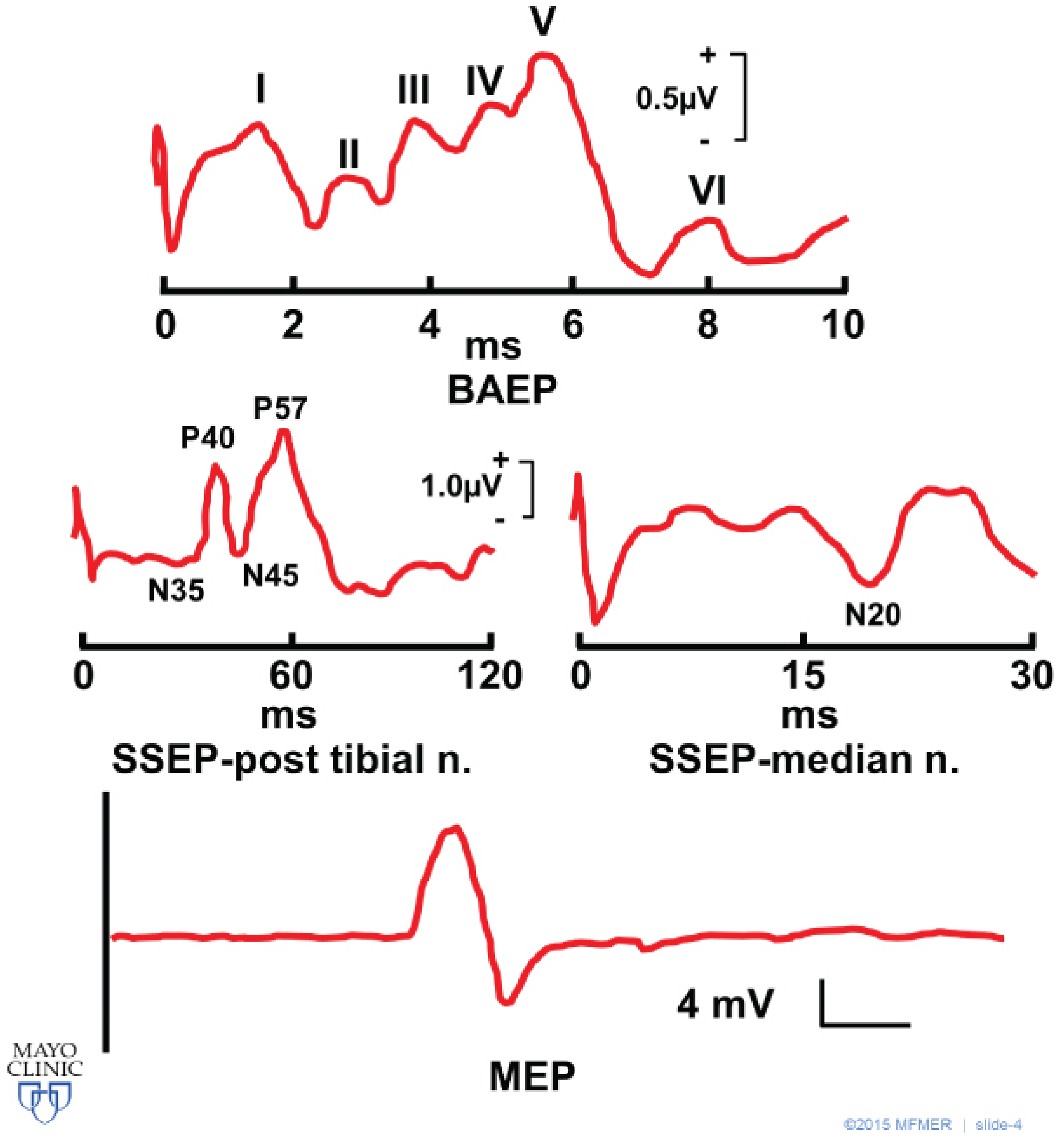
Representative BAEP, SSEP, and MEP waveforms (Mayo Clinic):
1. Somatosensory Evoked Potentials (SSEP)
Physiology and Pathway
SSEPs monitor the dorsal column/posterior spinal cord - specifically the proprioception and vibration pathways supplied by the posterior spinal artery. Stimuli travel predominantly via the posterior column/medial lemniscal pathway.
Technique
- A peripheral nerve is stimulated repetitively (e.g., median nerve, ulnar nerve, posterior tibial nerve)
- Responses recorded at:
- Subcortical level: upper cervical spine (C5), inion/popliteal fossa
- Cortical level: scalp electrodes
- For lower limb: electrodes placed on bilateral malleoli to stimulate posterior tibial nerve; recordings at popliteal fossa, C5, and vertex
Waveform Parameters
- Amplitude (microvolts): voltage of a peak relative to baseline
- Latency (milliseconds): delay after stimulation - reflects neural transit time
- SSEP-posterior tibial nerve shows peaks P40, N35, N45, P57
- SSEP-median nerve shows the important N20 peak (cortical)
Alert Criteria
- >50% decrease in amplitude - significant warning sign
- >10% increase in latency - significant warning sign
Advantages
- Continuous, real-time monitoring
- Does not require muscle relaxant avoidance
- Detects ischemia, compression, and direct trauma
Disadvantages and Limitations
- Monitors only posterior cord (sensory pathways) - can miss anterior cord injury
- "SSEP-silent paraplegia" - postoperative paraplegia can occur despite preserved intraoperative SSEPs (anterior spinal artery syndrome)
- Affected by: volatile anesthetics (dose-dependent amplitude decrease and latency increase), hypothermia, hypotension, hypoxia, hypercarbia
- Requires signal averaging (thousands of stimuli) - takes more time per reading
Effect of Anesthesia on SSEPs
- Volatile agents: dose-dependent increases in latency and decreases in cortical (but NOT subcortical) amplitude
- 0.5-1 MAC with nitrous oxide is generally compatible with SSEP monitoring in neurologically intact patients
- Neurologically impaired patients show much greater sensitivity to inhaled agents
- Propofol: minimal effects on early cortical and subcortical SSEPs - often the preferred agent for SSEP monitoring
- Nitrous oxide: decreases amplitude without significant latency change
- Muscle relaxants: do not affect SSEPs
2. Motor Evoked Potentials (MEP)
Physiology and Pathway
MEPs monitor the anterior spinal cord (corticospinal tracts) supplied by the anterior spinal artery. They assess the motor cortex and anterolateral spinal cord.
Technique
- Transcranial electrical stimulation (indirect stimulation via scalp electrodes over the precentral/motor cortex) is most common; magnetic stimulation is less used
- A single pulse or train of pulses depolarizes upper motor neurons, signal travels caudad to the ventral horn, then via α-motor neurons to the motor endplates
- Responses recorded as Compound Muscle Action Potentials (CMAPs) from:
- Abductor digiti minimi
- Tibialis anterior
- Abductor hallucis muscle
- Unlike SSEPs, MEPs do not require signal averaging - results in seconds
Alert Criteria
- >50% decrease in amplitude = significant (Pelosi criterion)
- >70% reduction - alert threshold used by Kobayashi et al. (spinal deformity/tumor)
- >80% reduction - Langeloo criterion for predicting neurological deficit
- Total loss of MEP signal = most alarming finding (binary: present/absent)
- Increased stimulation intensity needed to maintain a reproducible signal also indicates a worrisome change
- Latency is less important for MEPs than for SSEPs
Advantages
- Directly monitors motor pathways - what SSEPs cannot
- More sensitive than SSEPs for detecting impending motor deficits
- No signal averaging needed - rapid feedback
- Superior to SSEPs for assessing spinal cord integrity (Level I evidence, AANS/CNS position statement)
- Can predict recovery in traumatic cervical spinal cord injury
Disadvantages and Limitations
- Muscle relaxants abolish MEP signals - neuromuscular blockade must be avoided or minimized
- More technically difficult than SSEPs
- Volatile anesthetics profoundly suppress MEPs more than SSEPs
- Patient movement during MEP stimulation can be a concern (risk of bite injury - mouth guard recommended)
Effect of Anesthesia on MEPs
- Volatile agents: potently suppress MEPs even at low concentrations
- Total intravenous anesthesia (TIVA) - propofol + opioid infusion is the preferred technique when MEPs are monitored
- If both SSEP and MEP are needed: ultrashort-acting opioid infusion (e.g., remifentanil) + low-dose inhaled anesthetic or TIVA with BIS/EEG monitoring to prevent awareness
- Neuromuscular blocking agents: must be avoided (MEPs cannot be recorded in the presence of full muscle relaxation)
- Etomidate infusions have been used to enhance SSEP amplitudes in patients with poor baseline signals
3. The Wake-Up Test (Stagnara Test)
Concept
First described by Stagnara, the wake-up test involves intraoperative awakening of the patient after completion of spinal instrumentation to assess conscious voluntary motor function of the upper and lower extremities.
Procedure
- Surgical anesthesia maintained with volatile anesthetic + nitrous oxide + opioids ± propofol
- After instrumentation, anesthetic agents are reduced/stopped
- Patient is asked to move hands and feet on command
- If hands move but not feet → distraction on the rod is released one notch → wake-up test repeated
- Once confirmed, re-anesthesia and surgery continues
Key: Opioids are important for analgesia and tolerance of the endotracheal tube while the patient is awake. 0-20% of patients have recall of the event, and it is rarely viewed as unpleasant.
Advantages
- Simple, no specialized equipment required
- Directly assesses voluntary motor function - the most clinically relevant endpoint
- Can provide therapeutic benefit: the hemodynamic changes associated with waking can improve spinal cord perfusion
- Useful when SSEP/MEP are unavailable, equivocal, or have failed
Disadvantages and Limitations
| Risk | Detail |
|---|---|
| Uncooperative patient | May thrash, dislodge ETT, or fall from table |
| Only a single time-point | Provides reassurance only at that moment; cannot detect injury occurring later |
| False reassurance | Cannot monitor injury between wake-up test and end of surgery |
| Recall | 0-20% of patients have intraoperative awareness |
| Delayed wake-up | Increases time-to-treatment if true injury present |
| Increased OR time | Adds time vs. continuous electrophysiologic monitoring |
When to Use the Wake-Up Test
- When SSEP/MEP are not available (resource-limited settings)
- When electrophysiologic signals are equivocal or fail
- As an adjunct to confirm a definitive neurological status when electrophysiologic changes occur
- After an SSEP/MEP alert - to determine if a true deficit exists before major surgical revision
4. Combined SSEP + MEP Monitoring
The current standard for high-risk spinal surgery. The rationale is that the two modalities are complementary:
| Feature | SSEP | MEP |
|---|---|---|
| Pathway monitored | Posterior columns (sensory) | Corticospinal tract (motor) |
| Blood supply monitored | Posterior spinal artery | Anterior spinal artery |
| Detects | Proprioception/vibration deficits | Motor deficits / paraplegia |
| Averaging required | Yes (slow) | No (rapid) |
| Muscle relaxants | Not affected | Abolished |
| Preferred anesthesia | Propofol-based or low-dose volatile | TIVA mandatory |
Combined SSEP + MEP monitoring substantially increases sensitivity and specificity for detecting spinal cord compromise:
- A multicenter study of 1,156 thoracic spine surgeries using transcranial MEPs showed sensitivity 91.9%, specificity 88.4% for predicting postoperative outcomes
- MEPs in combination with SSEPs increase early detection of spinal cord ischemia, especially for anterior cord pathology
5. Response to an Intraoperative Alert
When there is an acute change in SSEP/MEP signal amplitude or latency:
- Stop the current surgical maneuver
- Raise blood pressure to normal or 20% above baseline (augment spinal cord perfusion pressure)
- Reduce or discontinue volatile agents (rule out anesthetic-related suppression)
- Check arterial blood gases (rule out hypoxia, hypercarbia, metabolic derangement)
- Communicate with the surgeon - release distraction/instrumentation if present
- If signals do not return to baseline → perform a wake-up test to definitively exclude neurological deficit
6. Other IONM Modalities
| Modality | Application |
|---|---|
| EMG (electromyography) | Pedicle screw testing ("triggered EMG"), nerve root monitoring, cranial nerve monitoring during acoustic neuroma/skull base surgery. Sensitive to mechanical and thermal injury. Abolished by muscle relaxants. |
| BAEP (brainstem auditory evoked potentials) | Acoustic neuroma resection, microvascular decompression of CN V/VII, brainstem surgery. Extremely robust - minimally affected by any anesthetic. |
| VEP (visual evoked potentials) | Orbital and optic pathway surgery. Highly variable - unreliable intraoperatively. |
| EEG | Carotid endarterectomy (cerebral ischemia detection), depth of anesthesia monitoring. |
7. Practical Anesthetic Considerations
| Drug Class | SSEP | MEP | BAEP |
|---|---|---|---|
| Volatile agents | Dose-dependent ↓ amplitude, ↑ latency (cortical) | Potent suppression | Minimal effect |
| Nitrous oxide | ↓ amplitude (alone) | Suppresses | No effect |
| Propofol | Minimal effect (preferred) | Relatively preserved | Minor |
| Opioids | Minimal | Minimal | Minimal |
| Benzodiazepines | Mild ↓ amplitude | Suppresses | Minimal |
| Ketamine | May enhance | Relatively preserved | Minimal |
| Etomidate | Can enhance SSEPs | Less suppression than propofol | No significant effect |
| Muscle relaxants | No effect | Abolished | No effect |
Key anesthetic principle: For combined SSEP + MEP monitoring, use TIVA (propofol + remifentanil infusion) with BIS monitoring to prevent awareness. Avoid neuromuscular blockade. If SSEP-only, low-dose volatile (≤0.5 MAC) is acceptable.
Summary: Comparison Table
| Feature | SSEP | MEP | Wake-up Test |
|---|---|---|---|
| What it monitors | Posterior cord (sensory) | Anterior cord (motor) | Voluntary motor function |
| Anesthesia required | Light volatile or TIVA | TIVA mandatory | Short-acting agents |
| Muscle relaxants | OK | Contraindicated | Not applicable |
| Continuous monitoring | Yes | Yes | No (single time-point) |
| Detects slow ischemia | Yes | Yes | No |
| Equipment needed | Yes (electrodes, computer) | Yes (stimulator + electrodes) | None |
| False negatives | Anterior cord lesions | Sensory-only lesions | Late injuries |
| Sensitivity/specificity | Moderate | High (91.9% / 88.4%) | Variable |
Sources:
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Spinal Cord Monitoring, p. 4359-4361
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Central Nervous System Function, p. 3074-3078
- Miller's Anesthesia, 10e - Anesthesia and Evoked Responses, p. 5243-5245
- Mulholland & Greenfield's Surgery, 7e - Neurologic Outcomes (TAAA), p. 5041-5042
- AANS/CNS Position Statement on IOM (Level I evidence)
- MDPI Journal of Clinical Medicine: IONM in Neurosurgery (2024)
This is a shared conversation. Sign in to Orris to start your own chat.