Osteomalacia in pregnancy definition causes signs mangement of this high risk pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
osteomalacia pregnancy management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching the Web
osteomalacia in pregnancy high risk management antenatal complications obstetric
Loading Image
I now have comprehensive information. Here is the full structured answer:
Osteomalacia in Pregnancy
Definition
Osteomalacia is a metabolic bone disease characterized by impaired mineralization of newly formed bone matrix (osteoid) in adults. Calcium, phosphate, and vitamin D are all necessary for normal bone mineralization. When any of these are deficient or their metabolism is disrupted, osteoid accumulates without being mineralized - producing soft, weak, pain-prone bones.
In the context of pregnancy, vitamin D requirements are significantly increased to meet both maternal and fetal skeletal demands. Women - particularly during pregnancy and lactation - are at heightened risk because:
- Fetal skeletal development draws heavily on maternal calcium and vitamin D stores
- Nutritional intake may be inadequate
- Limited sunlight exposure worsens the deficit
"In adults, vitamin D deficiency may result in osteomalacia which occurs mainly in women, especially during pregnancy and lactation when requirements of vitamin D are increased."
- Park's Textbook of Preventive and Social Medicine
Causes
Primary Cause: Vitamin D Deficiency
The most common underlying mechanism. Vitamin D undergoes two hydroxylations:
- In the liver → 25-hydroxyvitamin D (25-OHD) - the storage form
- In the kidney → 1,25-dihydroxyvitamin D (calcitriol) - the active form
Calcitriol promotes intestinal calcium absorption and bone mineralization. Deficiency at any step results in osteomalacia.
Causes Classified by Mechanism
| Category | Examples |
|---|---|
| Insufficient UV exposure | Purdah/veiling practices, housebound women, dark skin pigmentation, northern latitudes |
| Dietary deficiency | Vegetarian/vegan diet, poverty, malnutrition |
| Malabsorption | Celiac disease, Crohn's disease, post-gastrectomy, biliary disorders, pancreatic insufficiency |
| Reduced 25-OHD synthesis | Severe liver disease, nephrotic syndrome (urinary losses of vitamin D metabolites) |
| Reduced 1,25(OH)₂D synthesis | Chronic kidney disease, vitamin D-dependent rickets type I |
| Drug-induced | Anti-epileptic drugs (phenobarbital, phenytoin) accelerate 25-OHD catabolism |
| Hypophosphatemia | X-linked hypophosphatemia, autosomal dominant hypophosphatemic rickets |
| Inhibitors of mineralization | Hypophosphatasia (alkaline phosphatase deficiency), aluminum toxicity, bisphosphonate overuse |
| Pregnancy-aggravated | Pre-existing subclinical deficiency unmasked by increased fetal demand |
In India and developing countries, the purdah system, low dietary intake, and limited healthcare access compound the risk, especially in pregnant women.
Signs and Symptoms
Symptoms
- Bone pain - generalized, poorly localized; worse in pelvis, spine, ribs, lower extremities; worse at night and with weight bearing
- Proximal muscle weakness - difficulty climbing stairs, rising from a chair/toilet; patients pull themselves up by hand rails
- Waddling gait - flat-footed, springless "mother penguin's walk" due to combined bone pain and muscle weakness
- Muscle cramps, paresthesias - fingertip tingling from hypocalcemia
Signs on Examination
- Bone tenderness - elicited by pressing on the tibiae, wrists, pubic rami, iliac crests, or rib cage compression
- Chvostek's sign - facial twitch with gentle tap anterior to the ear (hypocalcemia)
- Trousseau's sign - carpopedal spasm with blood pressure cuff inflation (hypocalcemia)
- Pelvic deformity - the pelvis may become narrowed/contracted (triradiate or flat-rachitic pelvis), creating contracted pelvis - a major obstetric concern
- Kyphoscoliosis, scoliosis in severe long-standing cases
- Wrist enlargement, rickety rosary in coexisting rickets/severe deficiency
Specific Obstetric Concern
A contracted or deformed pelvis from osteomalacia is a recognized cause of cephalopelvic disproportion (CPD) and obstructed labor. This is one of the primary reasons why osteomalacia in pregnancy is classified as a high-risk pregnancy.
Investigations / Diagnosis
Biochemistry
| Test | Finding |
|---|---|
| Serum calcium | Low to low-normal |
| Serum phosphate | Low (precedes hypocalcemia due to secondary hyperparathyroidism) |
| Serum PTH | Elevated (secondary hyperparathyroidism) |
| Serum alkaline phosphatase | Elevated (classically raised; "healing flare" occurs during treatment) |
| Serum 25-OHD | < 10-15 ng/mL is diagnostic |
| Serum 1,25(OH)₂D | Usually elevated (due to PTH-driven conversion) - not helpful for diagnosis |
| Serum magnesium | Low in malabsorption (can worsen hypocalcemia by impairing PTH secretion) |
Radiology
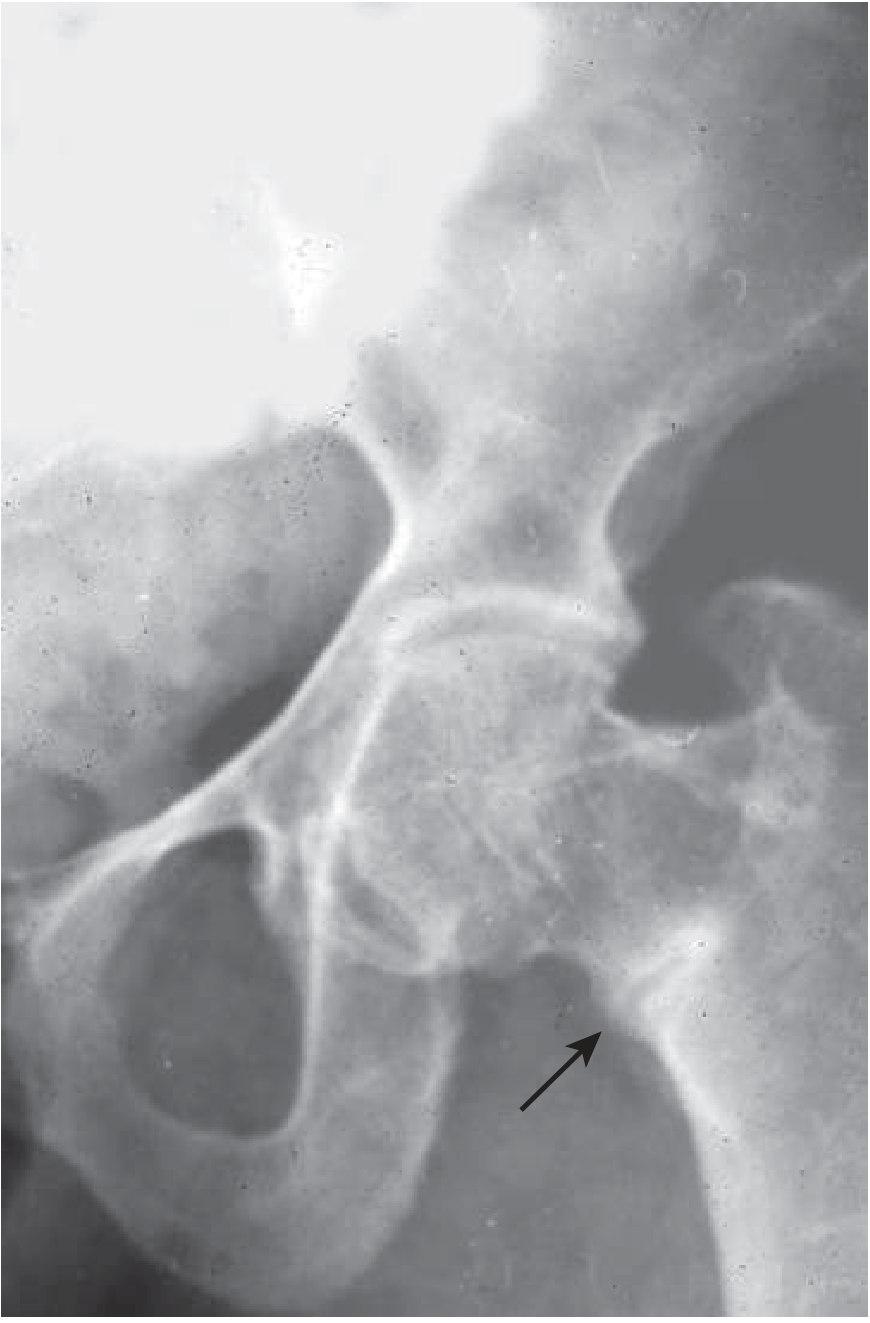
- Looser's zones (pseudofractures) - pathognomonic: narrow lucent bands perpendicular to the bone cortex, often bilateral and symmetric, seen at the femoral neck, pubic rami, ribs, and scapulae
- Generalized bone rarefaction / osteopenia
- Pelvic deformity on X-ray: triradiate pelvis, platypelloid shape
- Bone scan may show focal uptake that can be mistaken for metastatic disease
Bone Biopsy (rarely needed in pregnancy)
- Tetracycline double-labeling showing excess unmineralized osteoid - gold standard but impractical in pregnancy
Management as a High-Risk Pregnancy
Osteomalacia in pregnancy is classified as high-risk for the following reasons:
- Contracted pelvis → CPD → obstructed/prolonged labor → risk of uterine rupture, fetal distress
- Hypocalcemia → maternal tetany, seizures, cardiac arrhythmia; neonatal hypocalcemia and congenital rickets
- Maternal bone fragility → pathological fractures (pelvis, vertebrae, femoral neck) during labor
- Neonatal consequences → neonatal hypocalcemia, neonatal seizures, congenital rickets, low birth weight, fractures in the newborn
Antenatal Management
1. Early Identification
- Detailed history: diet, sunlight exposure, veiling practices, previous pregnancies with similar symptoms, malabsorption disorders
- Book as high-risk; refer to a tertiary center with multidisciplinary team (obstetrician, endocrinologist, neonatologist)
- Baseline blood work: serum calcium, phosphate, alkaline phosphatase, 25-OHD, PTH, renal and liver function tests
2. Vitamin D Supplementation
The dose depends on baseline 25-OHD levels:
| Serum 25(OH)D | Loading Dose (Vitamin D₂ or D₃) | Maintenance |
|---|---|---|
| 20-30 ng/mL | 50,000 IU once/week × 10 weeks | Once/month |
| 10-20 ng/mL | 50,000 IU twice/week × 10 weeks | Twice/month |
| < 10 ng/mL | 50,000 IU three times/week × 10 weeks | Three times/month |
| Malabsorption/severe | Calcitriol 0.25-0.5 µg/day (acts faster, safer to monitor) | Ongoing with monitoring |
- The goal is to raise 25-OHD to > 30 ng/mL and normalize PTH
- Calcitriol is preferred in malabsorption because it bypasses the need for hepatic and renal hydroxylation
- Monitor serum calcium every 2-3 weeks once treatment starts
- Urinary Ca:Cr ratio should remain < 0.22 (mg/mg)
- Caution: excess vitamin D in pregnancy can cause fetal/neonatal hypercalcemia; do not exceed safe doses
3. Calcium Supplementation
- 1,000-1,500 mg/day of elemental calcium in divided doses (3x/day with meals for best absorption)
- Calcium citrate is preferred over carbonate in malabsorptive conditions
- Monitor urinary calcium to avoid hypercalciuria/nephrolithiasis
4. Nutrition and Lifestyle
- High-calcium diet: dairy products, green leafy vegetables, fortified foods
- Safe sunlight exposure: 15-30 minutes/day to face and arms
- Treat underlying cause: gluten-free diet for celiac, manage liver/renal disease
- Correct hypomagnesemia if present (critical for PTH secretion)
5. Pelvic Assessment
- Clinical pelvic assessment and pelvimetry (X-ray pelvimetry is avoided in pregnancy; MRI pelvimetry preferred)
- Serial obstetric ultrasounds for fetal growth and biometry
- Document pelvic dimensions for delivery planning
Intrapartum Management
- Mode of delivery is the most critical decision:
- If pelvis is adequate and no deformity: allow trial of labor with close monitoring
- If pelvis is contracted (CPD) or deformed: elective Caesarean section is indicated to prevent obstructed labor, uterine rupture, and fetal demise
- Regional anesthesia (epidural/spinal) is generally safe; document vertebral deformities pre-procedure
- Monitor for hypocalcemic tetany during labor (calcium gluconate IV must be available)
- Calcium gluconate 10% (10 mL IV slowly) for acute hypocalcemic tetany or Chvostek-positive symptomatic patients during labor
Postpartum / Neonatal Management
- Continue vitamin D and calcium supplementation during lactation (requirements remain high)
- Breastfed infants of deficient mothers need vitamin D 400 IU/day supplementation
- Check neonatal serum calcium in the first 24-72 hours - neonatal hypocalcemia may manifest as jitteriness, apnea, or seizures
- Assess newborn for congenital rickets (bony deformities, soft skull/craniotabes)
- Arrange bone mineral density assessment for the mother postpartum
Summary Table
| Aspect | Key Point |
|---|---|
| Definition | Impaired mineralization of adult bone matrix |
| Primary cause in pregnancy | Vitamin D deficiency; increased by fetal demand |
| Key symptom | Bone pain, proximal myopathy, waddling gait |
| Key sign | Bone tenderness, Chvostek's, Trousseau's, contracted pelvis |
| Lab hallmark | Low 25-OHD, high ALP, low phosphate, high PTH |
| X-ray hallmark | Looser's zones (pseudofractures), pelvic deformity |
| High-risk feature | Contracted pelvis → CPD, neonatal hypocalcemia, fractures |
| Treatment | Vitamin D loading + calcium supplementation; treat underlying cause |
| Delivery | Elective LSCS if contracted pelvis or CPD confirmed |
Sources: Goldman-Cecil Medicine (26th ed.); Firestein & Kelley's Textbook of Rheumatology; Park's Textbook of Preventive and Social Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; ACOG Committee Opinion on Vitamin D in Pregnancy (reaffirmed 2024)
This is a shared conversation. Sign in to Orris to start your own chat.