g protein coupled reaction. Pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
That's a nicotinic receptor image (ligand-gated ion channel), not a GPCR diagram. I have all the material needed now. Let me compile the comprehensive answer.
G Protein-Coupled Receptors (GPCRs) - Pharmacology
1. Overview
GPCRs are the largest family of cell surface receptors in the human genome (>800 members). They mediate responses to hormones, neurotransmitters, odorants, and photons, and are targets for approximately 30-40% of all approved drugs.
They are also called:
- Seven-transmembrane (7-TM) receptors - because the polypeptide chain crosses the membrane 7 times
- Serpentine receptors - because of their winding structure across the membrane
Katzung's Basic and Clinical Pharmacology, 16th Edition - The receptor polypeptide chain "snakes" across the plasma membrane seven times. Agonist binds from the extracellular side; the G protein interacts with cytoplasmic regions, especially the third cytoplasmic loop connecting transmembrane regions V and VI.
2. Structure of a GPCR
- Extracellular N-terminus - ligand binding domain
- 7 hydrophobic transmembrane helices (I-VII) - embedded in the lipid bilayer
- 3 extracellular loops and 3 intracellular loops
- Intracellular C-terminus - couples to G proteins
The G protein heterotrimer has 3 subunits:
- Gα - binds GTP/GDP; determines effector specificity
- Gβ and Gγ - anchor the complex to the cytoplasmic membrane face; also have independent signaling roles
3. The Activation Cycle (GTP-GDP Cycle)
This is the core mechanism - illustrated below:
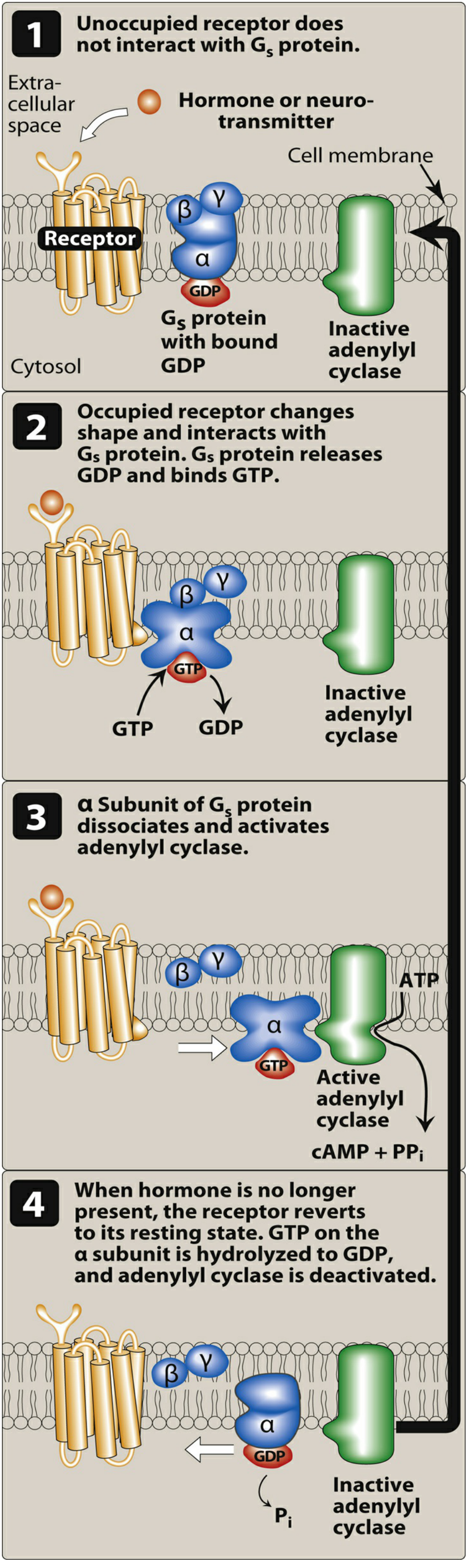
Step-by-step:
| Step | Event |
|---|---|
| 1. Basal state | Receptor is unoccupied. Gα subunit is bound to GDP; heterotrimer (αβγ) is inactive. |
| 2. Agonist binds | Agonist binds receptor → receptor undergoes conformational change → receptor acts as a guanine nucleotide exchange factor (GEF) |
| 3. GDP → GTP exchange | Activated receptor promotes release of GDP from Gα; GTP (abundant in cytoplasm) enters the nucleotide binding site |
| 4. Dissociation | GTP-bound Gα dissociates from Gβγ; both GTP-Gα and free Gβγ can now activate downstream effectors |
| 5. Effector activation | GTP-Gα (or Gβγ) activates enzymes (adenylyl cyclase, PLC) or ion channels |
| 6. Signal termination | Gα has intrinsic GTPase activity → hydrolyzes GTP to GDP → Gα becomes inactive again → reassociates with Gβγ → cycle resets |
Katzung's, p. 57: "GTP-bound Gs may remain active for tens of seconds before it is inactivated by hydrolysis, prolonging and enormously amplifying the original signal."
4. G Protein Subtypes and Their Effectors
| G Protein | Receptors (Examples) | Effector | Effect |
|---|---|---|---|
| Gs | β-adrenoceptors, glucagon-R, TSH-R, D1/D5 dopamine, 5-HT4 | ↑ Adenylyl cyclase | ↑ cAMP |
| Gi | α2-adrenoceptors, muscarinic M2/M4, opioid receptors, D2 dopamine | ↓ Adenylyl cyclase; open K+ channels | ↓ cAMP; ↓ heart rate |
| Gq | Muscarinic M1/M3, α1-adrenoceptors, 5-HT2, histamine H1 | ↑ Phospholipase C-β | ↑ IP3 + DAG → ↑ Ca2+ + PKC |
| Golf | Odorant receptors (olfactory epithelium) | ↑ Adenylyl cyclase | ↑ cAMP |
| Gt (Transducin) | Rhodopsin, color opsins (retinal rods/cones) | ↑ cGMP phosphodiesterase | ↓ cGMP (phototransduction) |
| G12/13 | Thromboxane, LPA receptors | Rho-GEF | Cytoskeletal changes |
Source: Katzung's Basic and Clinical Pharmacology, Table 2-1
5. Second Messenger Pathways
Pathway A: cAMP (via Gs or Gi)
Gs → ↑ adenylyl cyclase → ATP → cAMP → ↑ Protein Kinase A (PKA)
PKA phosphorylates target proteins, producing effects like:
- Cardiac: ↑ heart rate and contractility (β1 adrenoceptor)
- Smooth muscle: relaxation (β2 adrenoceptor)
- Metabolic: glycogenolysis (glucagon receptor)
Gi → ↓ adenylyl cyclase → ↓ cAMP → ↓ PKA (opposite effects)
Pathway B: IP3/DAG/Ca²+ (via Gq)
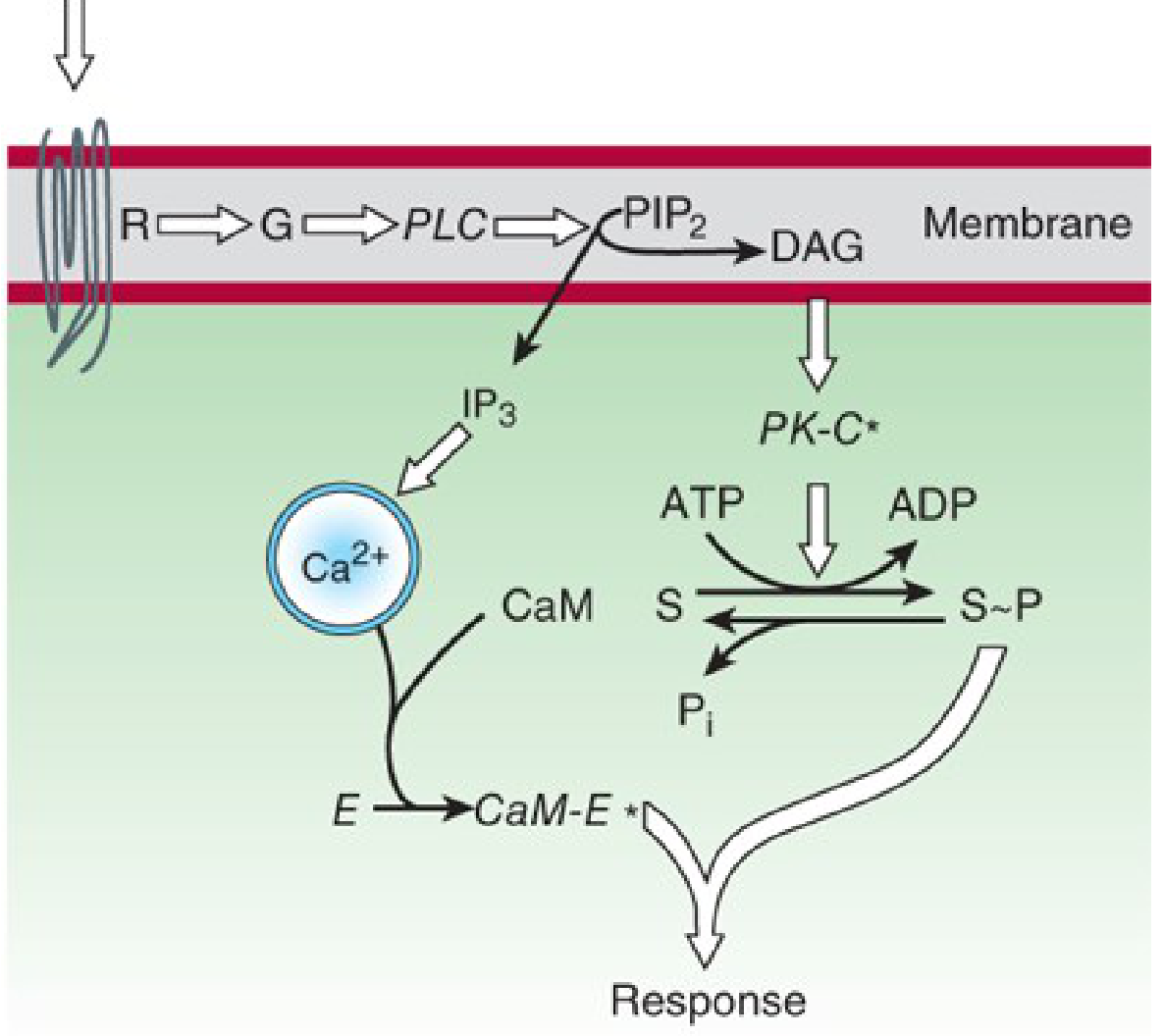
Gq → ↑ Phospholipase C-β (PLC-β) → cleaves PIP2 into IP3 + DAG
- IP3 (inositol-1,4,5-trisphosphate): diffuses to ER/sarcoplasmic reticulum → releases Ca²+ into cytoplasm → Ca²+ binds calmodulin → activates calmodulin-dependent kinases (e.g., myosin light chain kinase - smooth muscle contraction)
- DAG (diacylglycerol): stays in membrane → activates Protein Kinase C (PKC) → phosphorylates various substrates
Lippincott Illustrated Reviews: Pharmacology: "DAG and cAMP activate specific protein kinases within the cell, leading to a myriad of physiological effects. IP3 increases intracellular calcium concentration, which in turn activates other protein kinases."
Termination:
- IP3 is dephosphorylated (lithium inhibits this step - relevant to bipolar disorder treatment)
- DAG is phosphorylated to phosphatidic acid or deacylated to arachidonic acid
- Ca²+ is actively pumped out by Ca²+ pumps
Pathway C: cGMP
Relevant in:
- Retina: rhodopsin (GPCR for light) → Gt (transducin) → ↑ cGMP phosphodiesterase → ↓ cGMP → closure of cGMP-gated Na+ channels → hyperpolarization → visual signal
- Vascular smooth muscle: NO → guanylyl cyclase → ↑ cGMP → ↑ PKG → myosin dephosphorylation → vasodilation (basis for sildenafil's action - PDE5 inhibitor prevents cGMP breakdown)
6. Key Pharmacological Concepts
Signal Amplification
One agonist-receptor complex can activate many G proteins; each active adenylyl cyclase molecule generates many cAMP molecules - this creates a cascade amplification effect.
Desensitization (Tachyphylaxis)
Prolonged agonist exposure causes:
- GPCR kinases (GRKs) phosphorylate the activated receptor
- β-arrestin binds the phosphorylated receptor → sterically uncouples G protein
- Receptor internalization (endocytosis) - reduces surface receptor density
Biased Agonism (Functional Selectivity)
Most GPCRs can signal through both G protein and β-arrestin pathways. Some drugs preferentially activate one pathway - e.g., G protein-biased opioid agonists (aim: analgesia without β-arrestin-mediated side effects).
Kaplan & Sadock's: "Classical receptor pharmacology theory posits that a full agonist at a receptor will activate all signaling pathways equally... [but] biased agonism describes drugs that selectively activate one pathway over another."
7. Clinically Important GPCRs and Drugs
| Receptor | Drugs Acting on It | Indication |
|---|---|---|
| β1/β2-adrenoceptor (Gs) | Salbutamol (agonist), Propranolol (antagonist) | Asthma, hypertension, heart failure |
| α1-adrenoceptor (Gq) | Prazosin (antagonist) | Hypertension, BPH |
| α2-adrenoceptor (Gi) | Clonidine (agonist) | Hypertension, ADHD |
| Muscarinic M1/M3 (Gq) | Atropine (antagonist), Pilocarpine (agonist) | Glaucoma, dry secretions |
| Muscarinic M2 (Gi) | Atropine | Bradycardia |
| Opioid μ-receptor (Gi) | Morphine, Fentanyl | Pain |
| D2 dopamine (Gi) | Haloperidol (antagonist) | Psychosis |
| H1 histamine (Gq) | Diphenhydramine (antagonist) | Allergies |
| 5-HT2 serotonin (Gq) | Clozapine (antagonist) | Atypical antipsychotic |
| Glucagon-R (Gs) | Glucagon, Semaglutide (GLP-1R) | Hypoglycemia, diabetes/obesity |
8. Toxins That Exploit the GPCR System
| Toxin | Mechanism | Effect |
|---|---|---|
| Cholera toxin | ADP-ribosylates Gsα → locks GTP in place (prevents GTPase) | Constitutive ↑ cAMP in intestinal cells → massive Cl-/water secretion → watery diarrhea |
| Pertussis toxin | ADP-ribosylates Giα → prevents receptor coupling | ↑ cAMP (blocks Gi suppression) → whooping cough pathology |
Sources: Katzung's Basic and Clinical Pharmacology (16th ed.), Lippincott Illustrated Reviews: Pharmacology, Goodman & Gilman's The Pharmacological Basis of Therapeutics, Costanzo Physiology (7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.