Radionuclide Bone Scanning
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I have comprehensive content now. Let me compile the full answer:
Radionuclide Bone Scanning (Bone Scintigraphy)
Principle and Tracer
Bone scintigraphy uses a physiologic approach to imaging. An organic phosphate analogue - methylene diphosphonate (MDP) or hydroxymethylene diphosphonate (HDP) - is tagged with the radionuclide technetium-99m (⁹⁹ᵐTc), giving the combined tracer ⁹⁹ᵐTc-MDP or ⁹⁹ᵐTc-HDP. After intravenous injection, the tracer is:
- Distributed throughout the body in proportion to regional perfusion
- Adsorbed onto the surface of osteoid at sites of active mineralization (calcium phosphate formation)
- Detected by gamma cameras that record photons emitted by the decaying radionuclide
The delayed bone images (3 to 24 hours) provide an indirect measure of osteoblastic activity, making bone scintigraphy effectively an imaging map of bone metabolism. ⁹⁹ᵐTc has a 6-hour half-life, precluding imaging beyond 24 hours. Tracer not incorporated into bone is eliminated by renal excretion.
Three-Phase Bone Scan
The classic technique involves three phases performed sequentially:
| Phase | Timing | What it shows |
|---|---|---|
| Phase 1 - Perfusion (Flow) | Dynamic images for first 2 minutes post-injection | Arterial blood flow |
| Phase 2 - Blood Pool | 2-5 minutes after injection | Relative blood pool distribution; diffuse increased activity in infection |
| Phase 3 - Static (Delayed) | 3 hours post-injection | True tracer incorporation into osteoid; depicts osteoblastic activity |
- In infection, diffuse increased activity is seen on blood pool images; this activity becomes focally increased on delayed views, and may persist for months
- In low-grade infection, phases 1 and 2 may be negative - only phase 3 may show changes
- If all three phases are negative, infection is essentially excluded
- At 24 hours, clearance of normal tracer amplifies retention in pathologic bone
Planar vs. Tomographic Imaging
Planar scintigraphy provides whole-body and spot views. It is analogous to plain radiography.
SPECT (Single-Photon Emission Computed Tomography) uses tomographic principles to generate cross-sectional images from multiple planar images, providing improved contrast and spatial resolution. It is more sensitive for detecting active facet arthritis or spondylolysis.
SPECT/CT is a fusion imaging technique acquiring both a CT and a nuclear SPECT study concurrently. It localizes areas of increased bone metabolism precisely, increasing overall sensitivity and specificity. Without CT, precise anatomic localization on conventional SPECT alone can be very difficult - for example, distinguishing facet arthritis from active spondylolysis in the posterior vertebral elements.
Clinical Applications
Oncology
- Most sensitive method for detecting bone metastases (whole-body skeletal scintigraphy)
- Screening tool to identify areas of increased bone activity that could represent metastatic spread
- Important limitation: multiple myeloma and purely lytic metastases may be negative on bone scan, as these tumors do not stimulate significant osteoblastic response
Orthopaedic Infection
- Relatively effective in identifying spinal infection (adjunct to MRI)
- Used as a screening tool for osteomyelitis, spondylodiscitis
- Low specificity - positive in infection but also in recent trauma or surgery, diabetic arthropathy, gout
- Sensitivity ~90%, Specificity ~100%, Accuracy ~94% when combined with ⁶⁷Ga scan
Bone & Joint Disorders
- Stress fractures
- Paget's disease
- Avascular necrosis (osteonecrosis)
- Pars interarticularis defects
- Pseudarthrosis (incomplete fusion)
- Active bone lesions: osteoid osteoma, osteoblastoma
- Discitis / vertebral body osteomyelitis
- Transient osteoporosis
Arthritis (Rheumatology)
Bone scintigraphy shows characteristic distribution patterns in different arthritides:
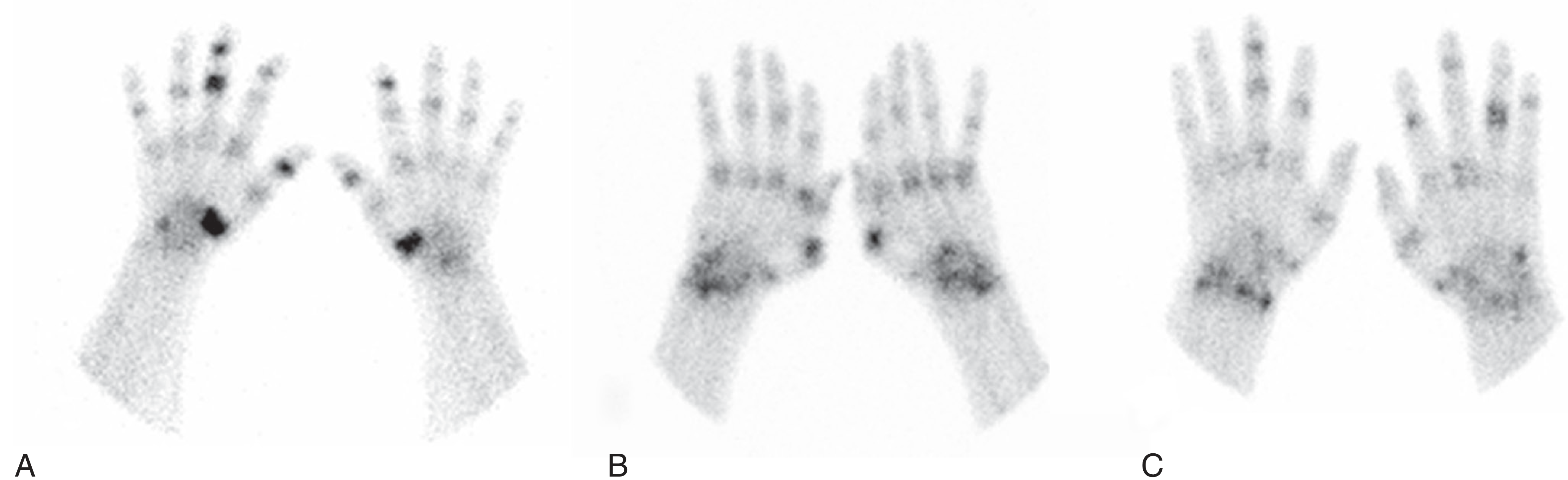
Distributions of activity on planar bone scintigraphy: (A) Osteoarthritis - severe activity in first CMC joints bilaterally with DIP/PIP involvement. (B) Rheumatoid arthritis - symmetric activity in radiocarpal joints, MCP and PIP joints. (C) Psoriatic arthritis - bilateral asymmetric distribution with ray pattern (Firestein & Kelley's Rheumatology)
- Bone scans are more sensitive than plain radiography because radionuclide uptake precedes morphologic bone changes visible on X-ray
- A suggestive bone scan must be confirmed with further imaging (not diagnostic alone)
Other Radionuclide Agents
| Agent | Use |
|---|---|
| ⁶⁷Ga (Gallium-67) scan | Good adjunct to ⁹⁹ᵐTc for osteomyelitis; especially detects soft-tissue infection in spondylodiscitis. Rapidly changes with resolution of acute infection (useful to document clinical improvement). Does NOT distinguish pyogenic from granulomatous infection |
| ¹¹¹In (Indium-111) WBC scan | Useful for detecting abscesses; differentiates noninfectious lesions (hematomas, seromas) from true infection; not reliable in acute infections; false-negatives occur in chronic infections |
| ⁹⁹ᵐTc-labeled leukocytes | Useful for acute infection; localizes in areas of acute inflammation |
| ¹⁸F-FDG PET | Highest sensitivity and specificity; delineates lesions at very early disease stages; FDG enters glucose cycle and concentrates in activated leukocytes/macrophages |
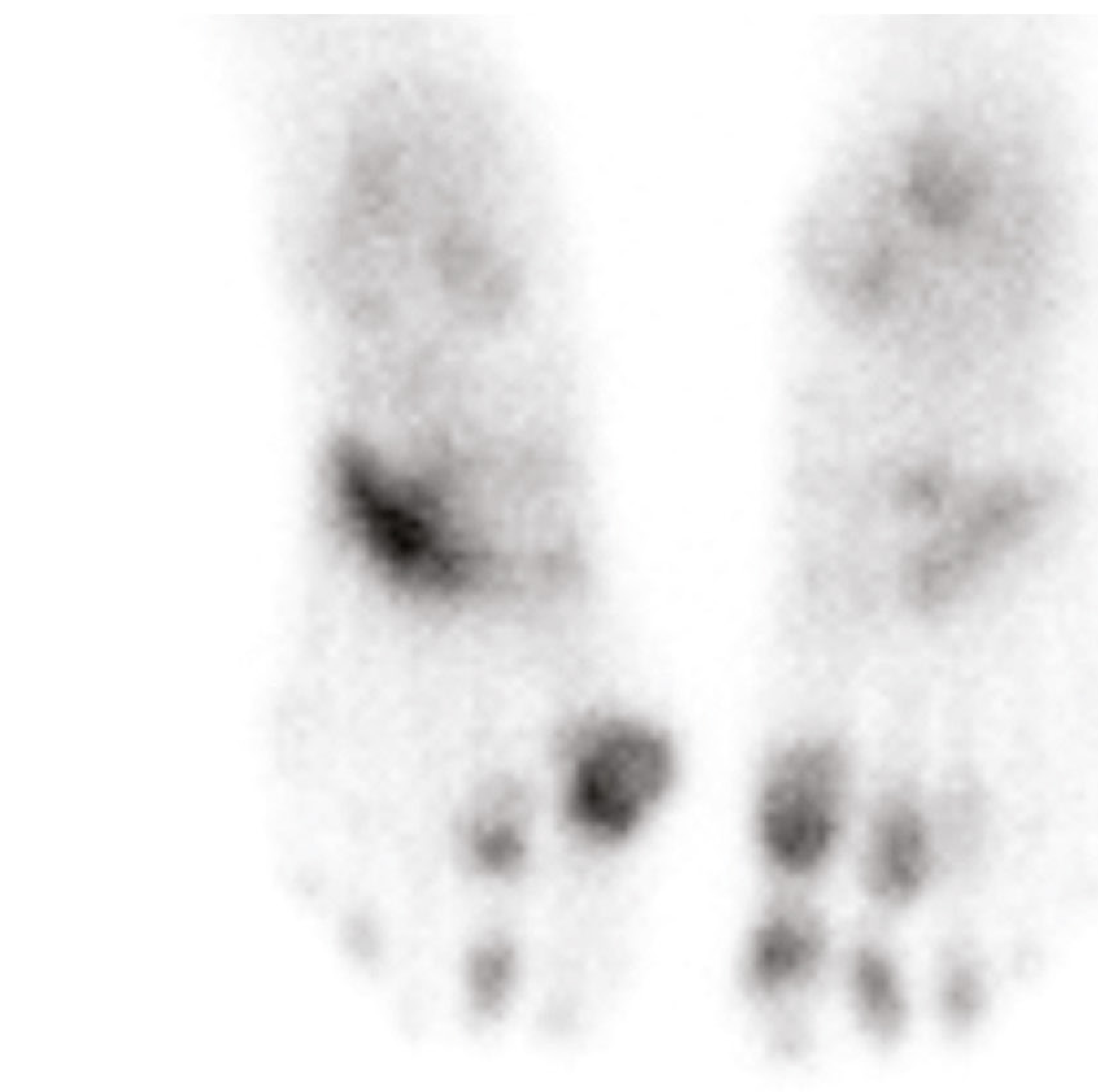
Below is a bone scan of both feet showing focal intense uptake in the left ankle region (likely infection or active arthritis):
Limitations and Pitfalls
- Low specificity: positive in any condition causing increased osteoblastic activity (infection, tumor, fracture, arthritis, Paget's, etc.)
- False negatives: multiple myeloma, purely lytic lesions, early osteonecrosis (cold scan), photopenic ("cold spot") metastases
- False positives: recent trauma or surgery, diabetic arthropathy, gout, degenerative changes
- Cannot show bone or joint detail well; distinguishing between bone, joint, or soft-tissue inflammation is often difficult on bone scan alone
- Multifocal vertebral lesions may be detected but bone scintigraphy is limited in depicting detailed surgical anatomy, particularly compared with CT or MRI
- Positive findings in the spine may be attributed to degenerative changes
Summary
| Feature | Detail |
|---|---|
| Tracer | ⁹⁹ᵐTc-MDP or ⁹⁹ᵐTc-HDP |
| Half-life | 6 hours |
| Mechanism | Adsorption onto osteoid at sites of active mineralization |
| Sensitivity | High (whole-body; detects early metabolic changes) |
| Specificity | Low (non-specific; many causes of increased uptake) |
| Imaging window | Up to 24 hours post-injection |
| Best for | Bone metastases survey, osteomyelitis (adjunct), metabolic bone disease, stress fractures |
| Pitfall | Negative in myeloma/lytic mets; false-positive from degenerative disease |
Sources:
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set, pp. 1152-1154
- Rockwood and Green's Fractures in Adults, 10th Ed 2025, p. Block 9
- Campbell's Operative Orthopaedics 15th Ed 2026, Blocks 9 & 23
- Bailey and Love's Short Practice of Surgery 28th Ed
- Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.