General medicine topic Surgical infection
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I now have comprehensive content to write a thorough answer on surgical infection. Let me compile this into a well-structured response.
Surgical Infection - Complete Overview
Source: Bailey and Love's Short Practice of Surgery, 28th Edition
1. Historical Background
Surgical infections have been documented for 4000-5000 years. Key milestones:
- Hippocrates: Used wine and vinegar to irrigate infected wounds - recognised that pus needed to be drained
- Galen: Named suppuration "pus bonum et laudabile" (good and praiseworthy pus) as it signalled localisation of infection
- Koch's Postulates (19th century): Established the scientific basis for infective disease
Koch's Postulates (Summary box 5.1):
-
The organism must be found in every case
-
It must be isolatable from the host and grown in culture
-
It must reproduce the disease when injected into a healthy host
-
It must be recovered from the experimentally infected host
-
Semmelweis: Reduced puerperal sepsis from >10% to <2% by handwashing between cases
-
Pasteur: Germ theory - microorganisms responsible for infection
-
Lister: Pioneered antiseptic surgery using carbolic acid spray
2. Microbiology of Surgical Infection
Gram-Positive Organisms
Streptococci (form chains, Gram +ve):
- Streptococcus pyogenes (Group A, β-haemolytic) - most pathogenic; causes cellulitis and tissue destruction via streptolysin, streptokinase, streptodornase
- Streptococcus faecalis (Lancefield Group D, enterococcus) - acts in synergy with other organisms
- Peptostreptococcus - anaerobic streptococcus
- All streptococci remain sensitive to penicillin and erythromycin; cephalosporins as alternative in penicillin allergy
Staphylococci (form clumps, Gram +ve):
- Staphylococcus aureus - most important pathogen; found in nasopharynx of up to 15% of the population; causes suppuration and implant infections
- MRSA (Methicillin-resistant S. aureus): Asymptomatic nasal carriage; managed by pre-admission screening in elective surgery; "search and destroy" methods used in northern Europe
- Staphylococcus epidermidis - coagulase-negative; causes prosthetic and line infections
Clostridia (Gram +ve anaerobes):
- Clostridium perfringens - gas gangrene; produces collagenase, hyaluronidase, phospholipase (lecithinase) causing myonecrosis
- Clostridium tetani - tetanus; produces tetanospasmin (neurotoxin); prevention by immunisation and wound toilet
- Clostridium difficile (C. diff) - antibiotic-associated colitis; produces toxins A and B; risk increased after broad-spectrum antibiotics (especially clindamycin, ampicillin, cephalosporins)
Gram-Negative Organisms
- Coliforms (E. coli, Klebsiella, Proteus) - bowel flora; common in abdominal surgical infections
- Pseudomonas aeruginosa - particularly in burns and wound infections; resistant to many antibiotics
- Bacteroides fragilis - most common anaerobe; bowel operations; sensitive to metronidazole
- Haemophilus influenzae - respiratory tract infections
3. Wound Classification (CDC/NNIS)
First introduced in 1964 by the US National Research Council; adapted by CDC:
| Class | Type | Description |
|---|---|---|
| I | Clean | Uninfected; no inflammation; GI/respiratory/GU tracts NOT entered; primarily closed |
| II | Clean-contaminated | GI, respiratory, GU tracts entered under controlled conditions without unusual contamination; no infection, no major break in technique |
| III | Contaminated | Open/fresh accidental wounds; major break in sterile technique; gross GI spillage; acute non-purulent inflammation |
| IV | Dirty | Old traumatic wounds with devitalised tissue; existing clinical infection or perforated viscera |
NNIS Risk Score (predicts SSI risk; scored 0-3, one point each for):
- Contaminated or dirty wound
- ASA score ≥3
- Operative time > 75th percentile for that procedure
4. Factors Determining Wound Infection (Summary box 5.4)
- Host response (immune competence)
- Virulence and inoculum of the infecting organism
- Vascularity and health of tissue (local ischaemia, systemic shock)
- Presence of dead or foreign tissue
- Presence of antibiotics during the "decisive period"
The Decisive Period
There is a 4-hour window after bacterial contamination before infection becomes established. Prophylactic antibiotics must achieve tissue levels above the MIC90 for expected pathogens during this period - after it, preventive strategies become ineffective.
Risk Factors for Wound Infection (Summary box 5.5)
- Malnutrition (obesity or weight loss)
- Metabolic disease (diabetes, uraemia, jaundice)
- Immunosuppression (cancer, AIDS, steroids, chemo/radiotherapy)
- Gut colonisation and translocation
- Poor perfusion (systemic shock, local ischaemia)
- Foreign body material
- Poor surgical technique (devitalised tissue, dead space, haematoma)
5. Host Defence Mechanisms
Natural defences that can be compromised by surgery:
- Mechanical: Intact skin and mucosal barriers
- Chemical: Gastric acid, bile salts, enzymes
- Humoral: Immunoglobulins, complement, opsonins, interferons
- Cellular: Phagocytes, macrophages, polymorphs, killer lymphocytes
6. Presentation of Surgical Infection
Major SSI
- Significant quantity of pus (spontaneous discharge or requiring secondary drainage procedure)
- Patient systemically unwell: tachycardia, pyrexia, raised WCC
- Delayed discharge from hospital
Minor SSI
- Small discharge of pus or infected serous fluid
- Not associated with systemic signs or delayed discharge
- Often resolves without antibiotics
Abscess
- Classical signs of Celsus: calor (heat), rubor (redness), dolor (pain), tumor (swelling), plus functio laesa (loss of function)
- Pus = dead/dying neutrophils succumbed to bacterial toxins
- Predominantly caused by Staphylococcus aureus
- Treatment: Incision and Drainage (I&D) - "ubi pus, ibi evacua" (where there is pus, evacuate it)
- Antibiotics alone are ineffective for an established abscess
Cellulitis
- Diffuse spreading infection of dermis and subcutaneous tissue
- Caused by β-haemolytic Streptococcus (Group A) - spreads via lymphatics and tissue planes
- Red, hot, tender skin without discrete margin
- Treatment: Penicillin (or erythromycin/cephalosporin); mark borders to monitor spread; elevation
7. Specific Surgical Infections
Necrotising Fasciitis (Synergistic Spreading Gangrene)
A rare but life-threatening deep fascial infection caused by a mixed polymicrobial flora acting synergistically:
- Coliforms, staphylococci, Bacteroides, anaerobic streptococci, peptostreptococci
- Aerobic bacteria destroy living tissue → anaerobic bacteria thrive
Named variants:
- Meleney's synergistic gangrene - abdominal wall
- Fournier's gangrene - scrotal/perineal
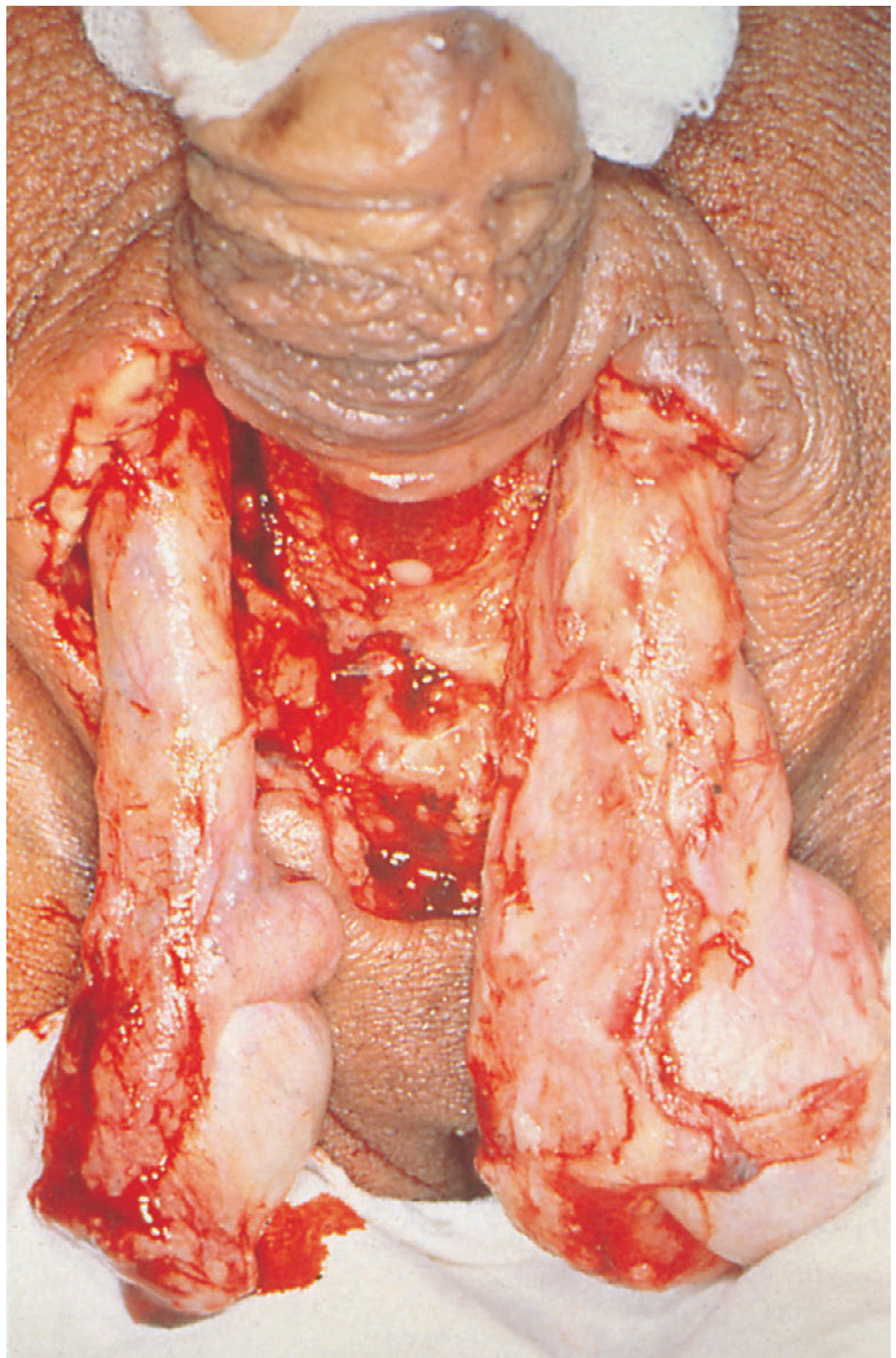
Clinical features:
- Severe wound pain
- Spreading inflammation with crepitus (gas in tissues) and odour
- Usually in immunocompromised patients (especially diabetics)
Diagnosis - The Finger Test:
- Infiltrate area with local anaesthetic
- Make 2-cm incision down to deep fascia
- Lack of bleeding = positive sign
- "Dishwater-coloured fluid" from wound = positive sign
- Gentle probing at deep fascia level - if tissues dissect with minimal resistance = positive
- Tissue biopsies for frozen section: characteristic findings - obliterative vasculitis, acute inflammation, subcutaneous necrosis
Treatment (surgical emergency):
- Broad-spectrum antibiotics + aggressive circulatory support
- Wide excision and laying open of all affected areas (debridement may be very extensive)
- Survivors may need large skin grafting
8. Systemic Infection
Bacteraemia
- Uncommon after superficial SSI (drains through wound)
- Common after deep space SSI (anastomotic breakdown)
- Often transient after instrumentation through infected bile or urine
- Dangerous in patients with implanted prostheses (haematogenous seeding)
- Causative organisms: aerobic Gram-negative bacilli, S. aureus, fungi
SIRS, Sepsis, and Septic Shock
(Table 5.1 definitions)
SIRS - presence of 2 out of 3 of the following:
- Hyperthermia (>38°C) or hypothermia (<36°C)
- Tachycardia (>90/min) or tachypnoea (>20/min)
- WCC >12 × 10⁹/L or <4 × 10⁹/L
Sepsis = SIRS + documented source of infection
Severe Sepsis = Sepsis + evidence of organ failure:
- Respiratory: ARDS
- Cardiovascular: Septic shock (↓ cardiac output + ↓ peripheral vascular resistance)
- Renal failure
Pathophysiology of SIRS:
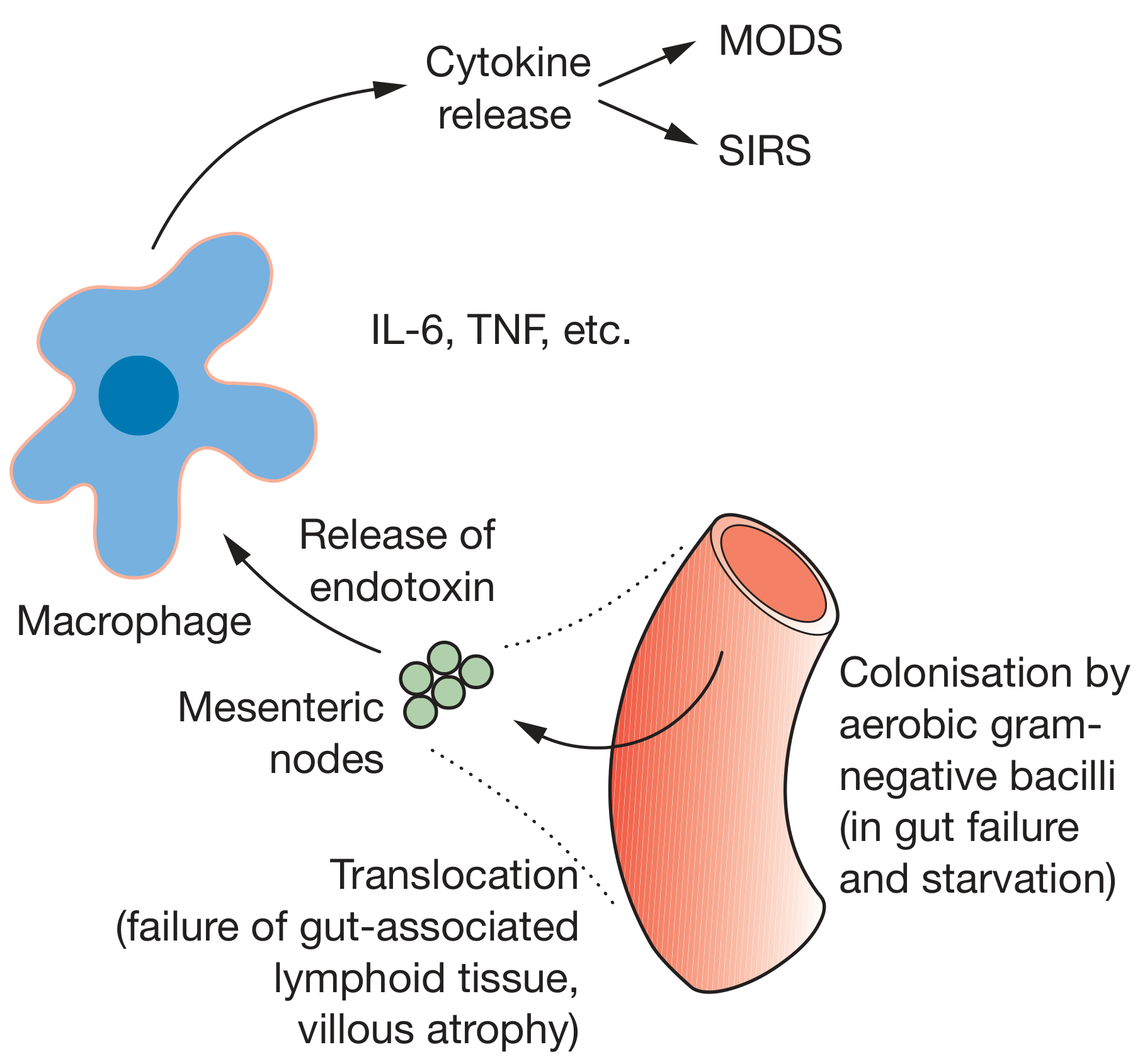 Gut failure → bacterial colonisation → endotoxin release → macrophage activation → cytokine release (IL-6, TNF) → SIRS/MODS
Gut failure → bacterial colonisation → endotoxin release → macrophage activation → cytokine release (IL-6, TNF) → SIRS/MODS
In gut failure and starvation, aerobic Gram-negative bacilli (mainly E. coli) colonise the gut. Bacterial translocation occurs through failed gut-associated lymphoid tissue (GALT) and villous atrophy → endotoxin (LPS from Gram-negative cell walls) reaches mesenteric nodes → macrophage activation → cytokine storm (TNF, IL-1, IL-6) → SIRS → Multi-Organ Dysfunction Syndrome (MODS)
Surviving Sepsis Campaign ("Sepsis Six" bundle)
- Give high-flow oxygen
- Take blood cultures
- Give IV antibiotics
- Start IV fluid resuscitation
- Check serum lactate and haemoglobin
- Measure urine output (insert catheter)
9. Antibiotic Prophylaxis
- Indicated for clean-contaminated and contaminated surgery
- Given to cover the "decisive period" (4 hours)
- Should be given 30 minutes before incision (IV at induction)
- Routine prophylaxis in clean, non-prosthetic surgery is of limited value and encourages resistant strains
- For prosthetic surgery (joint replacements, vascular grafts), prophylaxis is mandatory
Common prophylactic regimens:
- GI surgery: Cefuroxime + metronidazole
- Orthopaedic implant surgery: Cefuroxime or flucloxacillin
- Biliary surgery: Cefuroxime
10. Hospital-Acquired Infections (HAI)
Four main groups:
- Respiratory infections (incl. ventilator-associated pneumonia)
- Urinary tract infections (catheter-related)
- Bacteraemia (indwelling vascular catheter-related)
- Surgical Site Infections (SSI)
Prevention of HAI:
- Strict hand hygiene (Semmelweis principle)
- Aseptic technique
- Minimise indwelling catheters and their duration
- Regular replacement of IV cannulae
- MRSA screening pre-operatively for elective surgery
11. Universal Precautions (Bloodborne Viruses: HIV, Hepatitis B/C)
Applicable when operating on known or suspected infected patients:
- Full face mask or protective spectacles
- Fully waterproof disposable gowns and drapes
- Boots (not clogs) - prevent sharp injuries
- Double gloving (larger inner glove for comfort)
- Minimal essential personnel in theatre
- Respect for sharps - pass in a kidney dish only
- Slow, meticulous technique to minimise bleeding
Post-exposure (needle-stick injury):
- Wash under running water immediately
- Report the incident
- Occupational health advice + consider post-exposure prophylaxis (PEP)
- HIV and hepatitis testing; consider non-operative specialty if high-risk exposure
Key Summary Points for Exam
| Concept | Key Fact |
|---|---|
| Most common SSI organism | Staphylococcus aureus |
| Pus evacuation principle | "Ubi pus, ibi evacua" |
| Decisive period | Up to 4 hours |
| Necrotising fasciitis diagnosis | Finger test (lack of bleeding + minimal tissue resistance) |
| Fournier's gangrene | Scrotal necrotising fasciitis |
| Meleney's gangrene | Abdominal wall necrotising fasciitis |
| SIRS criteria | 2/3: temperature abnormality, tachycardia/tachypnoea, WCC abnormality |
| Sepsis definition | SIRS + documented infection source |
| MRSA decolonisation | Mupirocin nasal ointment + chlorhexidine washes |
| C. difficile treatment | Stop precipitating antibiotic; metronidazole or vancomycin (oral) |
| Gut translocation leads to | SIRS and MODS via endotoxin/cytokine release |
Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 5 - Surgical Infection
This is a shared conversation. Sign in to Orris to start your own chat.