Please thoroughly explain me the cvs examinations
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich content and key diagrams. Let me compile the full, thorough explanation.
Cardiovascular System (CVS) Examination
The CVS examination is a systematic bedside assessment of the heart and peripheral vasculature. It follows the standard clinical framework: general inspection → pulse → blood pressure → JVP → inspection of the precordium → palpation → auscultation, supplemented by peripheral vascular examination.
1. General Inspection
Before touching the patient, observe:
- Dyspnoea at rest - raised respiratory rate, use of accessory muscles (heart failure)
- Cyanosis - central (lips, tongue) vs. peripheral (fingertips). Central cyanosis indicates right-to-left shunting or severe pulmonary oedema
- Pallor - anaemia, poor perfusion
- Jaundice - right heart failure causing hepatic congestion
- Oedema - peripheral pitting oedema (ankles, sacrum in bed-bound patients) suggests biventricular failure
- Malar flush - butterfly-shaped redness of cheeks seen in mitral stenosis
- Diaphoresis - sweating from sympathetic activation (acute MI, cardiogenic shock)
- Cachexia - chronic heart failure
- Frailty - gait speed, handgrip strength, and muscle wasting should be assessed, particularly in patients undergoing catheter-based interventions
Syndromic Features
Certain genetic syndromes have cardiovascular associations and should be recognized on inspection:
| Syndrome | Inspection Findings | Cardiovascular Feature |
|---|---|---|
| Marfan | Tall stature, arachnodactyly, high-arched palate, pectus | Aortic root dilatation, MVP |
| Turner | Short stature, webbed neck, shield chest | Bicuspid aortic valve, coarctation |
| Down | Characteristic facies | ASD, VSD, AVSD |
| Ehlers-Danlos | Joint hypermobility, lax skin | Arterial aneurysms, MVP |
| Noonan | Webbed neck, widely spaced nipples | Pulmonary stenosis, HCM |
| Holt-Oram | Radial/carpal bone aplasia | ASD, VSD |
(Fuster & Hurst's The Heart, 15th Ed., Table 2-4)
Hands and Peripheries
- Clubbing - infective endocarditis, cyanotic congenital heart disease
- Splinter haemorrhages - linear dark streaks under nails, seen in endocarditis (but also trauma)
- Osler's nodes - tender red nodules on finger pulps (endocarditis)
- Janeway lesions - painless erythematous macules on palms/soles (endocarditis)
- Xanthomata - tendon xanthomata (familial hypercholesterolaemia)
- Koilonychia - spoon-shaped nails in iron deficiency (associated with high-output states)
- Capillary refill time - >2 seconds indicates poor perfusion
Eyes and Face
- Corneal arcus - lipid deposition (hyperlipidaemia)
- Xanthelasma - yellowish periorbital plaques (hyperlipidaemia)
- Fundus - hypertensive retinopathy (A/V nipping, flame haemorrhages, papilloedema), Roth spots (endocarditis)
2. Arterial Pulse
Palpate the radial pulse first, then the carotid for rate, rhythm, character, and volume.
Rate
- Tachycardia: >100 bpm
- Bradycardia: <60 bpm
Rhythm
- Regular
- Irregularly irregular - atrial fibrillation (no two beats the same)
- Regularly irregular - 2nd-degree AV block, bigeminy
Volume (Amplitude)
- High volume: aortic regurgitation, fever, anaemia, thyrotoxicosis, AV fistula
- Low volume: aortic stenosis, cardiogenic shock, pericardial tamponade
Character (Waveform)
This is best assessed at the carotid artery. The following waveform patterns are clinically important:
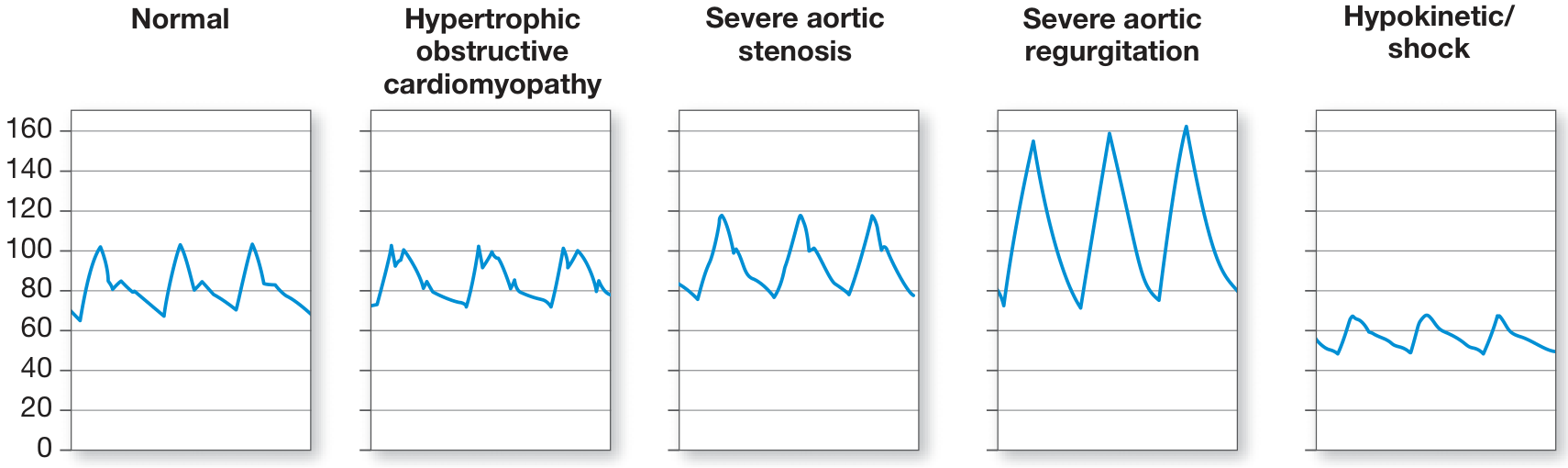
| Pattern | Description | Cause |
|---|---|---|
| Normal | Single smooth upstroke, rounded peak | - |
| Pulsus parvus et tardus | Small amplitude + slow rise ("plateau pulse") | Severe aortic stenosis |
| Collapsing (water-hammer) | Rapid rise, rapid fall | Aortic regurgitation, PDA, AV fistula |
| Bisferiens pulse | Two systolic peaks | HOCM (spike-and-dome), combined AS+AR |
| Pulsus alternans | Beat-to-beat alternation in amplitude (regular rhythm) | Severe LV systolic dysfunction |
| Pulsus paradoxus | Systolic BP fall >10 mmHg on inspiration | Cardiac tamponade, massive PE, severe asthma |
| Dicrotic pulse | Palpable dicrotic notch (felt as double pulse) | Low cardiac output states, sepsis |
Pulsus paradoxus is measured by noting the cuff pressure difference between when Korotkoff sounds are first heard (expiration only) and when they are heard on every beat. It is an exaggerated consequence of interventricular dependence.
Pulsus alternans is defined by beat-to-beat variability of pulse amplitude in a patient with a regular rhythm; it is seen in severe LV systolic dysfunction and is thought to result from cyclic changes in intracellular calcium and action potential duration. When associated with T-wave alternans on ECG, arrhythmic risk is increased.
(Harrison's Principles of Internal Medicine, 22nd Ed., p. 1906)
Radio-Femoral Delay
Simultaneous palpation of radial and femoral pulses: delay suggests coarctation of the aorta.
3. Blood Pressure
- Measured in the seated position, arm at heart level, back supported, after 5-10 minutes of rest
- Appropriate cuff size: bladder length 80%, width 40% of arm circumference
- Cuff too small = overestimates; cuff too large = underestimates
- Systolic = first Korotkoff sound; Diastolic = fifth Korotkoff sound (disappearance)
- In severe aortic regurgitation or large AV fistula, diastolic pressure may approach 0 mmHg; record both phase IV and V sounds in these cases
- Check both arms - >15 mmHg difference suggests subclavian stenosis or aortic dissection
Postural (orthostatic) hypotension: BP fall >20 mmHg systolic or >10 mmHg diastolic on standing; indicates hypovolaemia or autonomic dysfunction.
4. Jugular Venous Pulse (JVP)
The JVP is the single most important bedside measurement for estimating volume status and right heart haemodynamics. The internal jugular vein is preferred (the external jugular is valved and not directly in line with the right atrium).
Measuring JVP Height
- Position patient at 30-45° elevation
- Identify the top of the venous pulsation column
- Measure the vertical distance above the sternal angle (angle of Louis)
- Normal: ≤4.5 cm above the sternal angle
- Venous pulsations visible above the clavicle in the sitting position are always abnormal (distance from clavicle to right atrium is at least 10 cm)
- Elevated JVP predicts pulmonary artery wedge pressure >22 mmHg with a positive predictive value of 88%
- An elevated JVP is an independent predictor of hospitalization and death in heart failure patients
Distinguishing JVP from Carotid Pulse
| Feature | JVP | Carotid |
|---|---|---|
| Waveform | Biphasic (a and v waves) | Monophasic |
| Obliteration by pressure | Yes (light pressure) | No |
| Change with posture | Yes | No |
| Change with inspiration | Normally falls | No change |
JVP Waveform Components
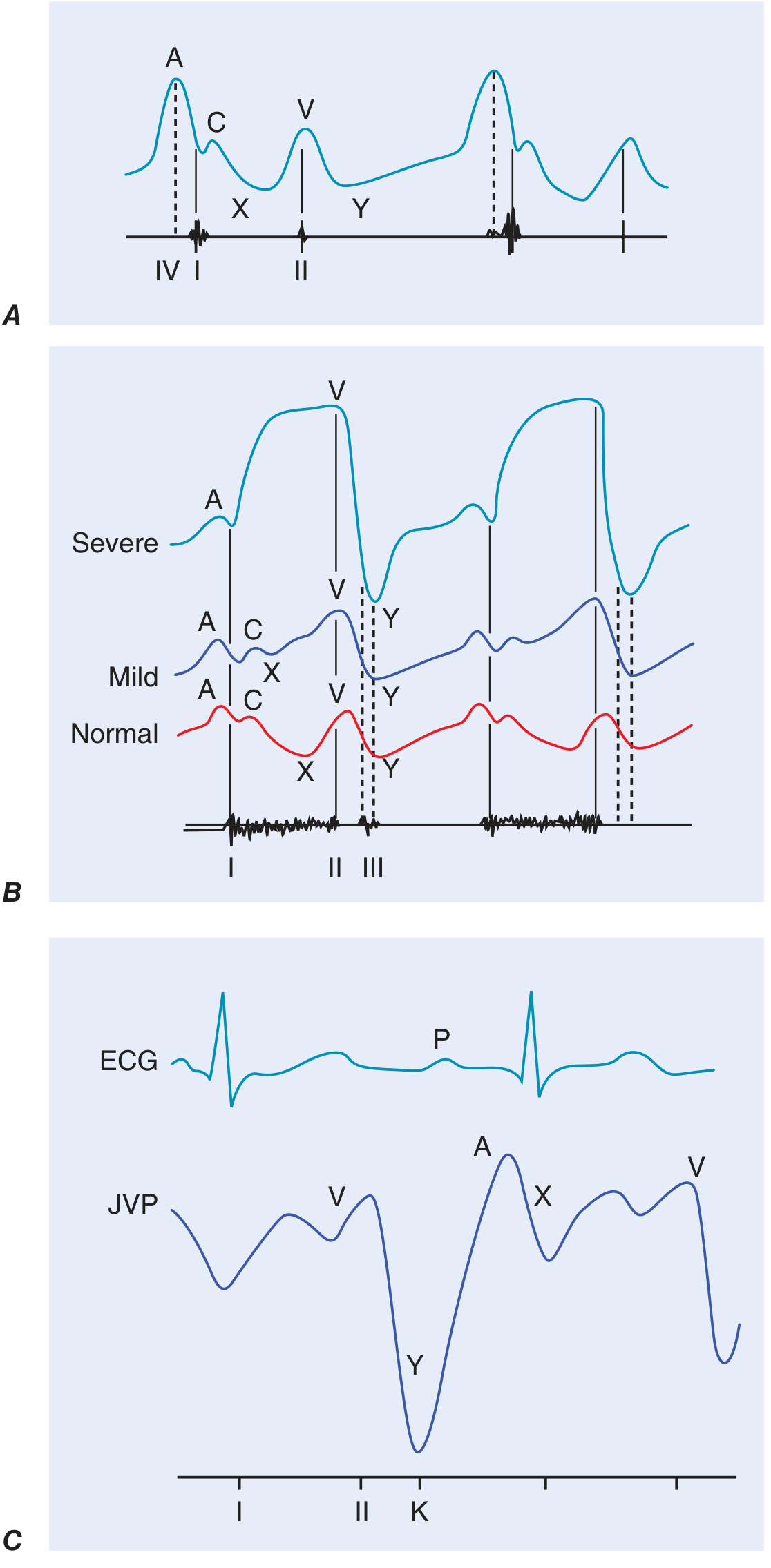
| Wave/Descent | Timing | Mechanism | Clinical Significance |
|---|---|---|---|
| a wave | Just before S1 (after P wave) | Right atrial presystolic contraction | Prominent in reduced RV compliance; absent in AF |
| Cannon a wave | a wave that is very large | RA contracts against closed tricuspid valve (AV dissociation) | Identifies VT in wide complex tachycardia |
| c wave | Early systole | Tricuspid valve pushed into RA during RV contraction | Usually not visible clinically |
| x descent | After a wave | Fall in RA pressure after tricuspid opening + atrial relaxation | Obliterated in tricuspid regurgitation |
| v wave | During ventricular systole (peaks at S2) | Atrial filling while tricuspid is closed | Large v wave = tricuspid regurgitation |
| y descent | After S2 (tricuspid opening) | Fall in RA pressure after tricuspid valve opens | Slow in tricuspid stenosis; prominent/rapid in constrictive pericarditis |
Abnormal JVP Patterns
- Large a wave: Pulmonary hypertension, pulmonary stenosis, tricuspid stenosis, reduced RV compliance
- Absent a wave: Atrial fibrillation
- Cannon a waves: Complete heart block, VT, ventricular pacing
- Large v wave: Tricuspid regurgitation (waveform becomes "ventricularized")
- Prominent y descent: Constrictive pericarditis (corresponds to pericardial knock)
- Kussmaul's sign: JVP rises (or fails to fall) with inspiration - indicates constrictive pericarditis or restrictive cardiomyopathy (normally JVP falls with inspiration)
- Abdominojugular reflux (hepatojugular reflux): Sustained JVP rise with firm abdominal pressure for >10-15 seconds - indicates elevated right-sided filling pressures
(Harrison's Principles of Internal Medicine, 22nd Ed., pp. 1904-1905; Fuster & Hurst's The Heart, 15th Ed.)
5. Inspection of the Precordium
- Apex beat location: Normally at the 5th intercostal space, midclavicular line
- Abnormal pulsations: Visible heaves or pulsations elsewhere are pathological
- Left parasternal heave: RV enlargement or pressure overload
- Right upper parasternal pulsation: Ascending aortic aneurysm
- Epigastric pulsation: May be normal in thin/tall patients or seen in advanced COPD (displaced heart), but also RV hypertrophy
6. Palpation of the Precordium
Start with the patient supine at 30°. Enhance the apex beat assessment by placing the patient in the left lateral decubitus position.
Apex Beat
The normal LV impulse is <2 cm in diameter, moves quickly away from the fingers, and is best felt at end-expiration.
| Finding | Significance |
|---|---|
| Displaced laterally/inferiorly | LV cavity enlargement (volume overload, dilated cardiomyopathy) |
| Sustained (heaving) apex | LV pressure overload (aortic stenosis, systemic hypertension) |
| Tapping apex | Palpable S1 in mitral stenosis |
| Double impulse | Palpable S4 + apex beat (LV hypertrophy, ischaemia) |
| Triple impulse | Rare - S4 + bisferiens pulse in HOCM |
| Dyskinetic impulse | LV aneurysm |
| Impalpable | COPD, obesity, pericardial effusion, dextrocardia |
Right Ventricular Palpation
- Left lower sternal border (thenar/hypothenar surface)
- Right 3rd-5th intercostal spaces (finger pads)
- Subxiphoid area
- A parasternal/sternal heave = RV pressure or volume overload
- A zone of retraction between RV and LV impulses may be felt in patients with RV overload when in the left lateral position
Thrills
Palpable vibrations (grade 4+ murmurs). Location indicates the source:
- Aortic area: aortic stenosis
- Left sternal edge (5th space): VSD
- Apex: mitral regurgitation/stenosis
7. Cardiac Auscultation
Use the diaphragm (high-pitched sounds: S1, S2, aortic/mitral regurgitation) and bell (low-pitched sounds: S3, S4, mitral stenosis rumble) of the stethoscope.
Auscultation Areas
| Area | Location | Valves Best Heard |
|---|---|---|
| Aortic | 2nd right intercostal space, sternal edge | Aortic valve |
| Pulmonary | 2nd left intercostal space, sternal edge | Pulmonary valve |
| Tricuspid | 4th-5th left intercostal space, lower sternal border | Tricuspid valve |
| Mitral (Apex) | 5th intercostal space, midclavicular line | Mitral valve |
Also auscultate the carotid arteries, axilla (radiation of mitral regurgitation), and the back (aortic coarctation).
Heart Sounds
S1 (First Heart Sound)
- Caused by mitral and tricuspid valve closure
- Best heard at the apex
- Loud S1: Mitral stenosis (early), hyperkinetic states, short PR interval, tachycardia
- Soft S1: Late mitral stenosis (calcified leaflets), long PR interval, beta-blockers, LV dysfunction
- Variable S1: Complete heart block (changing PR interval), AF
- Normal splitting: appreciated in young patients and RBBB
S2 (Second Heart Sound)
- Caused by aortic (A2) and pulmonary (P2) valve closure
- Best heard at the base
- Physiological splitting: A2 before P2; widens on inspiration (RV fills more, pulmonary valve closes later), narrows on expiration - normal
- Wide fixed splitting: ASD (right heart volume overload, equal throughout respiratory cycle)
- Wide splitting: RBBB, pulmonary stenosis, RV failure (delayed P2)
- Reversed (paradoxical) splitting: LBBB, severe AS, RV pacing (A2 delayed beyond P2, splits on expiration, narrows on inspiration)
- Loud P2: Pulmonary arterial hypertension
- Single S2: Severe AS (immobile aortic valve), Eisenmenger syndrome
S3 (Third Heart Sound)
- Low-pitched, early diastole (just after S2) - "Ken-tuc-KY"
- Normal in children, adolescents, young adults
- Pathological in older adults = rapid early ventricular filling in heart failure
- Left-sided S3 = heart failure with reduced OR preserved EF (equally prevalent in both)
- Right-sided S3 = louder at LLSB, increases with inspiration
- A left-sided S3 in chronic heart failure predicts cardiovascular morbidity and mortality
S4 (Fourth Heart Sound)
- Low-pitched, late diastole (just before S1) - "TEN-nes-see"
- Indicates presystolic LV expansion due to atrial kick into a non-compliant ventricle
- Seen in LV hypertrophy, active myocardial ischaemia, hypertension
- Absent in atrial fibrillation (no atrial contraction)
- A palpable presystolic impulse corresponding to S4 = marker of reduced LV compliance
Gallop Rhythm: S3 or S4 at a fast rate produces a triple rhythm resembling a gallop.
Additional Sounds
Ejection Sound (Click)
- High-pitched, early systole (just after S1), coincides with carotid upstroke
- Bicuspid aortic or pulmonary valve, aortic/pulmonary root dilatation
- Pulmonic ejection sound is the only right-sided sound that decreases with inspiration
- Becomes inaudible as the bicuspid valve calcifies
Opening Snap (OS) of Mitral Stenosis
- High-pitched, early diastole (just after S2), heard at apex/lower sternal border
- The A2-OS interval is inversely proportional to the left atrial-LV pressure gradient
- Shorter interval = higher gradient = more severe stenosis
- Disappears as leaflets calcify and become rigid
Pericardial Knock
- High-pitched, slightly later than OS, in constrictive pericarditis
- Corresponds to abrupt cessation of ventricular expansion after tricuspid valve opening
- Corresponds to prominent rapid y descent in JVP
Mid-Systolic Click
- Mitral valve prolapse (MVP)
- Single or multiple non-ejection clicks
- May introduce a late systolic murmur
- Moves toward S1 on standing (decreased preload); moves away from S1 on squatting (increased preload)
Tumor Plop
- Low-pitched sound, rare, in atrial myxoma
- Diastolic prolapse of the tumor across the mitral valve; may vary with position
Heart Murmurs
Murmurs are graded 1-6:
| Grade | Description |
|---|---|
| 1 | Barely audible, requires effort |
| 2 | Quiet but readily audible |
| 3 | Moderate, no thrill |
| 4 | Loud + palpable thrill |
| 5 | Very loud, heard with stethoscope partially off chest |
| 6 | Audible without stethoscope |
A thrill is present at grade 4 or greater.
Systolic Murmurs
Ejection (Mid-Systolic) Murmurs - crescendo-decrescendo, starts after S1, ends before S2
| Murmur | Location | Radiation | Features |
|---|---|---|---|
| Aortic stenosis | 2nd right ICS | Carotids | Harsh, plateau pulse; S4 common; single/paradoxically split S2 |
| Pulmonary stenosis | 2nd left ICS | None/back | Pulmonic ejection click; loud with inspiration |
| HCM | LLSB/apex | Variable | Dynamic - louder on standing/Valsalva; softer on squatting |
| Innocent flow murmur | 2nd-3rd left ICS | None | Soft, no radiation, normal S2, no other abnormalities |
Holosystolic (Pansystolic) Murmurs - start with S1, persist to S2
| Murmur | Location | Radiation | Features |
|---|---|---|---|
| Mitral regurgitation | Apex | Axilla | Blowing; soft S1; S3 if severe |
| Tricuspid regurgitation | LLSB | None | Increases with inspiration (Carvallo's sign); large v wave in JVP |
| VSD | 4th-5th left ICS | Entire precordium | Harsh; thrill common |
Late-Systolic Murmurs
- MVP: follows mid-systolic click
Diastolic Murmurs (always pathological)
| Murmur | Location | Radiation | Features |
|---|---|---|---|
| Aortic regurgitation | 3rd-4th left ICS sternal edge | Apex | High-pitched, blowing, decrescendo; heard leaning forward in expiration; collapsing pulse |
| Pulmonary regurgitation | 2nd-3rd left ICS | - | Graham-Steell murmur in pulmonary hypertension |
| Mitral stenosis | Apex | None | Low-pitched rumble; best heard with bell; opening snap precedes; increased by rolling to left lateral; patient exercise |
| Tricuspid stenosis | LLSB | None | Increases with inspiration |
Austin-Flint Murmur
A mid-diastolic rumble at the apex in severe aortic regurgitation, due to the AR jet impinging on the mitral valve and creating functional mitral stenosis. Distinguished from true MS by absence of opening snap.
Continuous Murmurs
- Patent ductus arteriosus (PDA): "machinery" murmur, peaks around S2
- Arteriovenous fistula, coronary AV fistula, ruptured sinus of Valsalva aneurysm
Dynamic Auscultation - Bedside Maneuvers
These maneuvers change preload, afterload, or contractility and help differentiate murmurs:
| Maneuver | Effect | Louder | Softer |
|---|---|---|---|
| Valsalva (strain phase) | Decreases venous return (preload) | HCM, MVP click moves earlier | Most other murmurs |
| Standing | Decreases venous return | HCM, MVP click moves earlier | Most other murmurs |
| Squatting | Increases venous return + afterload | Most murmurs (especially AS, MR) | HCM (softens), MVP click moves later |
| Leg raise | Increases venous return | Most murmurs | HCM |
| Inspiration | Increases right heart filling | All right-sided murmurs (Carvallo's sign) | Left-sided |
| Expiration (leaning forward) | Best position for AR | Aortic regurgitation | - |
| Left lateral decubitus | Brings apex closer to chest wall | Mitral stenosis rumble, S3, S4 | - |
| Handgrip | Increases afterload | MR, AR, Austin-Flint | HCM (decreases obstruction) |
| Amyl nitrite | Decreases afterload/preload | HCM, AS, PS | MR, AR, VSD |
8. Peripheral Vascular Examination
Peripheral Pulses
Assess all major pulses bilaterally: carotid, brachial, radial, femoral, popliteal, posterior tibial, dorsalis pedis.
- Level of claudication-producing obstruction can be localized by the level of pulse loss
- Calf claudication + decreased popliteal pulse = superficial femoral artery obstruction
- Ankle-Brachial Index (ABI): Systolic ankle pressure / systolic brachial pressure
- Normal: >0.9; Peripheral arterial disease: <0.9; Critical ischaemia: <0.4
- Abnormal pulse oximetry (>2% difference between finger and toe O2 saturation) can detect lower extremity PAD
- Femoral and/or popliteal artery aneurysms should be sought in patients with abdominal aortic aneurysm
Bruits
Auscultate over carotid, subclavian, abdominal aorta, and femoral arteries.
- A cervical bruit is a weak indicator of degree of stenosis; absence does not exclude significant obstruction
- A bruit extending into diastole or a palpable thrill = severe obstruction
- Also consider an AV fistula with enhanced flow as a cause
Peripheral Signs of Heart Failure
- Pitting oedema: ankles/sacrum; graded 1+ to 4+
- Hepatomegaly: tender, pulsatile in TR; smooth and firm in chronic congestion
- Ascites: advanced right heart failure
- Pleural effusion: typically right-sided or bilateral in heart failure
Summary Table: Key Exam Findings and Their Diagnoses
| Finding | Think of... |
|---|---|
| Loud S1 + opening snap + mid-diastolic rumble at apex | Mitral stenosis |
| Pansystolic murmur at apex radiating to axilla + S3 | Mitral regurgitation |
| Ejection systolic murmur at 2nd right ICS + plateau pulse + S4 | Aortic stenosis |
| Early diastolic murmur at 3rd left ICS + collapsing pulse | Aortic regurgitation |
| Pansystolic murmur at LLSB + large JVP v wave + pulsatile liver | Tricuspid regurgitation |
| Mid-systolic click + late systolic murmur | Mitral valve prolapse |
| Loud P2 + right parasternal heave + large a wave in JVP | Pulmonary hypertension |
| Raised JVP + Kussmaul sign + pericardial knock + prominent y descent | Constrictive pericarditis |
| Pulsus paradoxus + raised JVP + muffled heart sounds | Cardiac tamponade (Beck's triad) |
| Elevated JVP + displaced apex + S3 + bilateral basal crackles | Biventricular heart failure |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 246: "Cardiovascular Examination," pp. 1904-1910 (McGraw Hill Medical)
- Fuster and Hurst's The Heart, 15th Ed., Chapter 2: "Clinical Cardiovascular Examination" (Miranda & Nishimura)
- Goldman-Cecil Medicine, International Edition: "Physical Examination for Detection of Signs of Cardiovascular Disease"
Injection romiplostin
Reading File
Finding Sources
Searching the Web
romiplostim injection mechanism dose ITP 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full explanation:
Romiplostim (Nplate) - Injection
Overview
Romiplostim is a thrombopoietin receptor agonist (TPO-RA), also called a TPO mimetic or thrombopoiesis-stimulating agent, administered as a subcutaneous injection once weekly. It is marketed under the brand name Nplate by Amgen.
Why Romiplostim Was Developed
Natural recombinant thrombopoietin (rHuTPO) and its pegylated form were initially developed in the 1990s but had to be abandoned after a clinical trial in healthy platelet donors found that they induced autoantibodies against native thrombopoietin, paradoxically causing severe thrombocytopenia. This led to the development of small, structurally unrelated peptides that activate the TPO receptor without triggering cross-reactive antibodies - the TPO-RAs.
Structure and Chemistry
Romiplostim is a peptibody - a unique fusion protein composed of:
- Four copies of a small synthetic peptide that binds with high affinity to the TPO receptor (c-MPL)
- Grafted onto an immunoglobulin (IgG1 Fc) scaffold - the antibody portion extends the peptide's half-life in circulation
Crucially, the MPL-binding peptide has no sequence homology with human thrombopoietin. Because of this, romiplostim does not induce antibodies against endogenous TPO, which was the fatal flaw of earlier TPO preparations. There is no evidence in animal or human studies that it induces anti-TPO antibodies.
(Katzung's Basic & Clinical Pharmacology, 16th Ed.)
Mechanism of Action
Romiplostim binds to and activates the thrombopoietin receptor (c-MPL) on the surface of megakaryocytes and their progenitors in the bone marrow - the same receptor that endogenous TPO activates. This stimulates:
- Proliferation and differentiation of megakaryocyte progenitor cells
- Maturation of megakaryocytes
- Production and release of platelets into the circulation
It produces a dose-dependent increase in platelet count. The resulting platelet count rise is typically seen 5-7 days after initiation, with the peak effect at about 10-14 days after each dose.
(Goodman & Gilman's The Pharmacological Basis of Therapeutics; Goldman-Cecil Medicine)
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Route | Subcutaneous injection only |
| Frequency | Once weekly |
| Elimination | Reticuloendothelial system |
| Half-life | Average 3-4 days |
| Unique feature | Half-life is inversely related to platelet count - longer half-life when platelets are low (more TPO receptor available for elimination); shorter when platelets have recovered |
This inverse relationship between half-life and platelet count means the drug has a self-regulating pharmacokinetic profile.
Indications
1. Immune Thrombocytopenia (ITP) - Primary Indication
- Chronic ITP in adults and children who have had an inadequate response to:
- Corticosteroids
- Immunoglobulins (IVIG or anti-D)
- Splenectomy
- Used as second-line or later therapy (in many centres considered alongside splenectomy and rituximab)
- Subcutaneously administered romiplostim (along with oral eltrombopag and avatrombopag) is capable of increasing platelet counts in approximately 70-90% of patients with ITP; some sources cite >90% for durable platelet count improvement
2. Hematopoietic Syndrome of Acute Radiation Syndrome (HS-ARS)
- To increase survival in adults and children (including term neonates) acutely exposed to myelosuppressive doses of radiation
NOT indicated for:
- Thrombocytopenia due to myelodysplastic syndrome (MDS) - see warnings
- Any cause of thrombocytopenia other than chronic ITP (except HS-ARS)
- Normalizing platelet counts in patients where thrombocytopenia is not causing bleeding risk
Dosing and Administration
ITP (Adults and Pediatrics)
Goal: Use the lowest dose necessary to achieve and maintain platelet count ≥ 50 × 10⁹/L to reduce bleeding risk. Do NOT aim to normalize platelets.
| Step | Detail |
|---|---|
| Initial dose | 1 mcg/kg subcutaneously once weekly (based on actual body weight) |
| Maximum dose | 10 mcg/kg/week |
| Typical maintenance | Median dose 2-3 mcg/kg in clinical studies |
Dose Adjustment Algorithm
| Platelet Count | Action |
|---|---|
| < 50 × 10⁹/L | Increase dose by 1 mcg/kg |
| 50-200 × 10⁹/L | Maintain current dose |
| > 200 and ≤ 400 × 10⁹/L for 2 consecutive weeks | Decrease dose by 1 mcg/kg |
| > 400 × 10⁹/L | Hold dose; do not administer. Resume at 1 mcg/kg lower when count falls back below 200 × 10⁹/L |
Monitoring
- Weekly CBC including platelet count and peripheral blood smear until a stable platelet count is established
- Once stable, monitoring can be reduced to monthly
- Assess peripheral blood smear for cellular morphology (to detect marrow changes)
HS-ARS (Radiation Syndrome)
- Single dose of 10 mcg/kg subcutaneously, administered as soon as possible after confirmed/suspected exposure to myelosuppressive radiation doses
Preparation and Reconstitution
- Available as a lyophilized powder in single-use vials: 250 mcg/0.5 mL and 500 mcg/1 mL (after reconstitution, concentration = 500 mcg/mL)
- Reconstitute with sterile water for injection
- Administer subcutaneously; injection volumes may be very small (e.g. < 0.1 mL for low-weight patients)
- Single-use only; discard unused portion
Place in ITP Management
Romiplostim is positioned as a second-line (or later) agent:
FIRST LINE:
Corticosteroids (prednisone 1 mg/kg/day or dexamethasone 40 mg × 4 days)
± IVIG (1 g/kg × 1-2 doses) for rapid response
SECOND LINE (if relapsed/refractory ~30-40% of patients):
├── Thrombopoietin receptor agonists: Romiplostim (SC) / Eltrombopag (oral) / Avatrombopag (oral)
├── Rituximab (anti-CD20, ~25% durable remission at 12 months)
└── Splenectomy (~2/3 durable complete response)
LATER LINE:
Fostamatinib (SYK inhibitor), immunosuppressants, danazol, etc.
TPO-RAs produce durable platelet count improvements in >90% of ITP patients beginning 5-7 days after initiation. (Washington Manual of Medical Therapeutics)
Adverse Effects and Toxicity
Common
- Injection site reactions - pain, erythema, bruising at injection site
- Headache, fatigue, arthralgia, dizziness, insomnia
- Nausea, abdominal pain, diarrhoea
Important / Serious
| Adverse Effect | Details |
|---|---|
| Thromboembolic events | Thrombosis (DVT, PE, stroke) due to excessive platelet elevation; risk increases with platelet counts >400 × 10⁹/L - why dose is held at this threshold |
| Portal vein thrombosis | Reported with romiplostim, eltrombopag, and avatrombopag specifically in the setting of chronic liver disease |
| Bone marrow fibrosis / reticulin deposition | Can develop with long-term use; generally reversible on discontinuation; peripheral smear should be monitored for signs (teardrop cells, nucleated RBCs, immature WBCs) |
| Rebound thrombocytopenia | Platelet counts may fall sharply below baseline after discontinuation - do not stop abruptly; taper if needed |
| Increased blast count / progression to AML | In patients with myelodysplastic syndromes (MDS), romiplostim increases blast counts and risk of progression to acute myeloid leukaemia - contraindicated in MDS |
| Worsening thrombocytopenia if medication fails | If platelet count does not increase after 4 weeks at maximum dose (10 mcg/kg), reassess the diagnosis |
(Katzung's Basic & Clinical Pharmacology, 16th Ed., p. 945)
Contraindications / Special Warnings
- MDS: Do not use romiplostim to treat MDS-associated thrombocytopenia - increases risk of AML progression
- Do not use to normalize platelet counts - target is ≥50 × 10⁹/L to prevent bleeding, not normal range
- Avoid concurrent use with another TPO-RA (eltrombopag, avatrombopag, lusutrombopag)
- Chronic liver disease: Use with caution - portal vein thrombosis risk
Comparison with Other TPO-RAs
| Feature | Romiplostim | Eltrombopag | Avatrombopag |
|---|---|---|---|
| Route | Subcutaneous injection | Oral (tablet) | Oral (tablet) |
| Frequency | Once weekly | Once daily | Once daily |
| Receptor binding site | Extracellular domain of c-MPL | Transmembrane domain of c-MPL | Transmembrane domain of c-MPL |
| Structural homology to TPO | None (peptibody) | Non-peptide small molecule | Non-peptide small molecule |
| Starting dose (ITP) | 1 mcg/kg SC weekly | 50 mg/day orally (25 mg in Asian/liver impaired) | 20 mg/day orally |
| Max dose (ITP) | 10 mcg/kg weekly | 75 mg/day | - |
| Liver monitoring | Not required | Required (hepatotoxic) | Less stringent |
| Food restrictions | None | Yes (avoid calcium-rich foods ±4 hrs) | No |
| Liver disease use (procedural) | Not approved for this | Hepatitis C thrombocytopenia | Approved (10-13 days pre-procedure) |
Key Clinical Takeaways
- Romiplostim does not treat the underlying autoimmune cause of ITP - it compensates for increased platelet destruction by boosting production.
- Platelet count response begins within 5-7 days; full effect at 10-14 days.
- It is highly effective (~70-90% response rate) in refractory ITP.
- The dose is titrated to the platelet count, not the patient's symptoms.
- Never exceed 10 mcg/kg/week; hold when platelets >400 × 10⁹/L.
- Monitor for bone marrow fibrosis (peripheral smear changes) with long-term use.
- Rebound thrombocytopenia can occur after stopping - plan for gradual discontinuation.
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Chapter 33: "Megakaryocyte Growth Factors," pp. 944-945
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter: "Thrombopoietin Receptor Agonists"
- Goldman-Cecil Medicine, International Edition, Chapter: "Immune Thrombocytopenic Purpura - Second-Line Treatment"
- Washington Manual of Medical Therapeutics, Chapter on Hematology
- Nplate (romiplostim) Prescribing Information, Amgen (current)
Pt eaaily arousable manjhe
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.