Embryological and imaging considerations in a case of cryptorchidism
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Searching PubMed
cryptorchidism management orchiopexy
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the full answer.
Cryptorchidism: Embryological and Imaging Considerations
1. Definition and Epidemiology
Cryptorchidism (from Greek kryptos = hidden) refers to complete or partial failure of one or both testes to descend from the abdomen into the scrotal sac. Key epidemiological points:
- Affects ~30% of premature male infants (100% of those <900 g birthweight) and 3-5% of full-term males
- Falls to <1% by 1 year of age as most descend spontaneously
- Usually right-sided; bilateral in 10-25% of cases
- The most common defect found in neonates overall
(The Developing Human, Clinically Oriented Embryology; Grainger & Allison's Diagnostic Radiology)
2. Embryology of Testicular Descent
2a. Gonadal Differentiation
The embryological cascade begins well before descent:
- Gonads are first identifiable on the medial aspect of the urogenital ridge at 32 days postovulation
- SRY (sex-determining region, Y chromosome) expression starts at ~40 days' gestation, triggering testicular development via a cascade: SRY + SF1 → prolonged SOX9 expression → Sertoli cell differentiation
- By 6 weeks, primordial germ cells (PGCs) migrate from the yolk sac; by 8 weeks they are localized within testicular cords as gonocytes
- Leydig cells (producers of testosterone and INSL3) differentiate from mesenchymal precursors
(Campbell-Walsh-Wein Urology)
2b. Two Phases of Testicular Descent
Testicular descent occurs in two distinct hormonally regulated phases:
| Phase | Timing | Key Regulator | Mechanism |
|---|---|---|---|
| Transabdominal (Phase 1) | Weeks 8-15 | INSL3 (insulin-like factor 3) via its receptor RXFP2; also Müllerian-inhibiting substance (MIS/AMH) | Gubernacular swelling draws testis to the inguinal brim |
| Inguinoscrotal (Phase 2) | Weeks 25-35 | Androgens (DHT/testosterone via AR) + intact genitofemoral nerve (GFN) | Transinguinal passage; CGRP from GFN is the downstream mediator |
Key developmental milestones:
- Gubernacular swelling causes cellular proliferation and extracellular matrix expansion, enlarging the inguinal canal
- Transinguinal passage rarely occurs before 22 weeks; the majority of testes are scrotal after 27 weeks
- The scrotum itself forms from genital swellings first visible at 7 weeks, fusing by 10-12 weeks under dihydrotestosterone influence
- INSL3 and androgens synergistically stimulate gubernacular growth
Genetic factors include: INSL3, RXFP2, AR, SOX9, FGF9, AMH/MIS — mutations in any of these can cause cryptorchidism susceptibility.
(Campbell-Walsh-Wein Urology, "Embryology of Testicular Descent and Maldescent")
2c. Normal Positions vs. Cryptorchidism vs. Ectopia
The diagram below from The Developing Human maps the key positions:
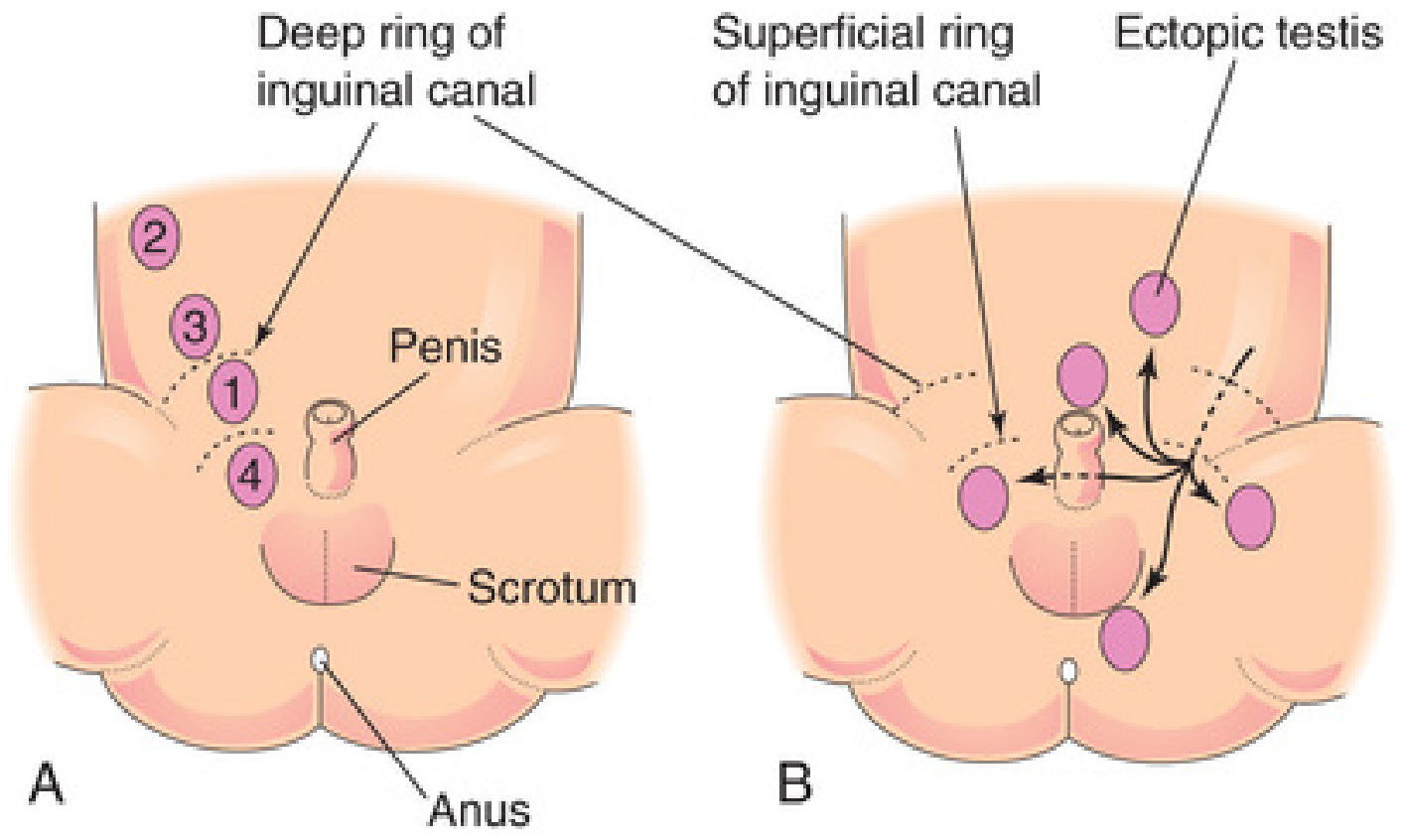
Fig. 12.48 - Positions of cryptorchid (A) and ectopic (B) testes. Cryptorchid positions in order of frequency: (1) inguinal canal, (2) abdominal, (3) just outside the deep ring, (4) just above the scrotum. Ectopic positions include perineal, femoral, suprapubic, and contralateral scrotal.
Cryptorchid testis = arrested along the normal path of descent (most commonly in the inguinal canal, ~80% of cases; abdominal arrest accounts for only 5-10%)
Ectopic testis = deviated from the normal path after exiting the superficial inguinal ring (possible locations: perineum, femoral canal, suprapubic region, base of penis, contralateral scrotum)
Retractile testis = normally descended testis that retracts due to an overactive cremaster reflex; can be brought down on examination and does NOT require surgery
3. Pathology and Histological Changes
Histological changes in the undescended testis begin as early as 6 months of age and become definitive by 2 years:
- Thickening of the basement membrane of spermatic tubules - the earliest change
- Loss of spermatogonia - tubules retain only Sertoli cells ("Sertoli cell-only" pattern)
- Tubular atrophy with hyaline connective tissue replacement
- Increased interstitial stroma - Leydig cells are spared and thus appear relatively prominent
- Germ cell neoplasia in situ (GCNIS) - may be present even at early ages
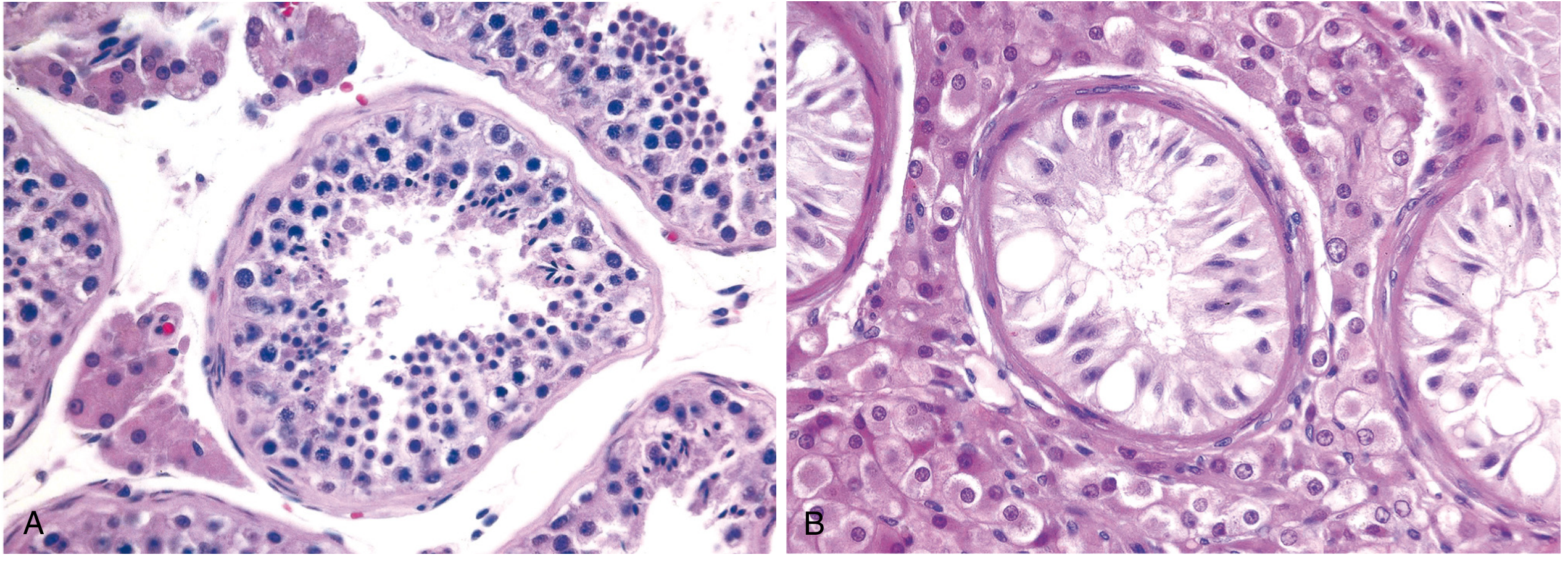
Fig. 21.15 - (A) Normal tubules with active spermatogenesis. (B) Testicular atrophy in cryptorchidism: tubules contain only Sertoli cells, no spermatogenesis, thickened basement membranes, apparent increase in interstitial Leydig cells.
Importantly, similar changes occur in the contralateral, normally descended testis in unilateral cryptorchidism, suggesting an intrinsic gonadal developmental defect (testicular dysgenesis syndrome) rather than purely a positional/thermal effect.
(Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology)
4. Imaging Considerations
4a. Ultrasound (US)
Technique:
- High-resolution linear array transducer required
- Begin with the scrotum to confirm bilateral absence
- Search in transverse planes with patience - the testis may be atrophic
- Trace the inguinal canal from the internal ring to the external ring
Performance characteristics:
| Location | Sensitivity |
|---|---|
| Palpable inguinal testes | ~97% |
| Non-palpable testes | ~75% |
| Intra-abdominal testes | ~45% (specificity 75%) |
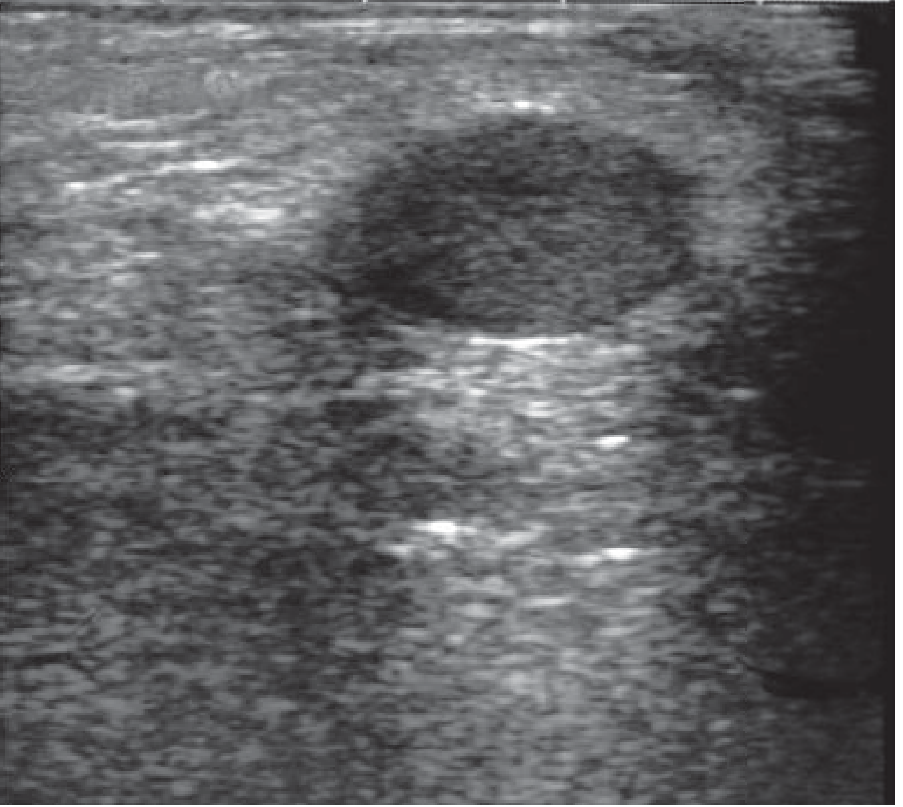
Fig. 33.22 - Undescended testis in an infant. The testis lies in the inguinal canal surrounded by suprapubic fat.
Clinical verdict on US: The American Urological Association states that routine scrotal ultrasound should NOT be pursued for standard cryptorchidism - multiple studies confirm poor sensitivity for locating the undescended testicle, and it does not alter the treatment plan. A reasonable exception is the difficult-to-examine obese child where inguinal US may simplify the surgical approach.
(Campbell-Walsh-Wein Urology; Grainger & Allison's Diagnostic Radiology)
4b. CT
CT studies offer the advantage of retroperitoneal imaging and have been used for non-inguinal undescended testes. Five CT patterns have been described based on combined assessment of the spermatic cord and testis. However, radiation exposure limits its use in children.
4c. MRI
MRI is far superior to US for localizing near-normal non-palpable testes and is preferred in:
- Ambiguous genitalia
- Severe hypospadias with non-palpable gonads
- Intra-abdominal testes not seen on US
MRI characteristics of undescended testis:
- Typically hypoplastic
- Low T2 signal (distinguishes from normal testicular tissue)
- Small, dysplastic testes may be indistinguishable from non-specific nodules
US is also useful in DSD cases for detecting Müllerian structures (uterus, fallopian tubes) that guide subsequent workup.
(Grainger & Allison's Diagnostic Radiology - Adult and Paediatric volumes)
4d. Diagnostic Laparoscopy
Laparoscopy is the definitive investigation for non-palpable testes - it allows for concurrent biopsy or immediate surgical correction, making preoperative imaging of questionable additional benefit to patient management.
5. Clinical Implications and Management
5a. Complications of Untreated Cryptorchidism
| Complication | Detail |
|---|---|
| Infertility | Associated even with unilateral cryptorchidism; sterility common if both testes remain undescended |
| Malignancy | 4-10x increased risk of germ cell tumors (seminoma most common); risk persists after orchiopexy and extends to the contralateral normally descended testis |
| Inguinal hernia | 10-20% of cases (due to patent processus vaginalis) |
| Torsion | Higher risk due to abnormal fixation |
| Trauma | Inguinal position vulnerable to crush injuries |
5b. Management Algorithm
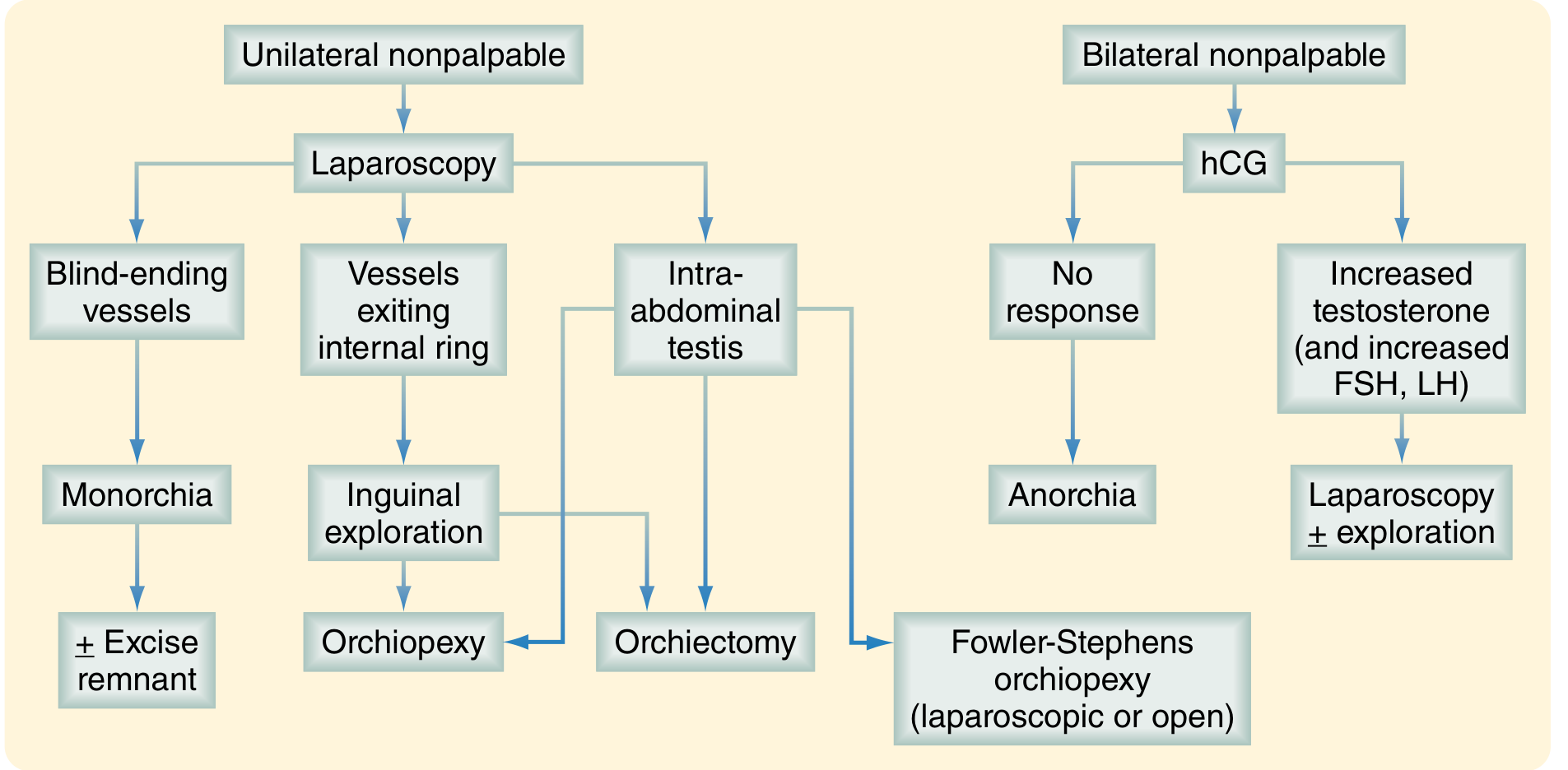
Fig. 117.20 - Management algorithm for nonpalpable undescended testes (Sabiston Textbook of Surgery)
Timing:
- Spontaneous descent expected by 1 year of age; observation until then
- If undescended at 1 year: orchiopexy at 6-12 months of age (or as soon as identified after 1 year)
- Early surgery is critical because histological changes begin by 6 months
Surgical options by location:
- Palpable inguinal testis: Standard dartos pouch orchiopexy
- Non-palpable / intra-abdominal: Diagnostic laparoscopy first
- Blind-ending vessels = monorchia (no testis present; consider excision of remnant)
- Vessels exiting internal ring = inguinal orchiopexy
- Intra-abdominal testis = Fowler-Stephens orchiopexy (two-stage: ligate testicular vessels first to develop collateral circulation; orchiopexy 6 months later) or laparoscopic single-stage orchiopexy
- Post-pubertal bilateral: Consider orchiectomy given malignancy risk; a 2024 systematic review evaluated post-pubertal management from the malignancy risk standpoint
Hormonal therapy: hCG or GnRH analogs may be used in bilateral non-palpable cases to stimulate testosterone response and confirm viable testicular tissue before deciding on exploration.
(Sabiston Textbook of Surgery; Campbell-Walsh-Wein Urology; Robbins & Kumar Pathologic Basis of Disease)
6. Associated Conditions
- Unilateral testicular agenesis: Associated with ipsilateral renal agenesis - a crucial point for imaging workup
- Prader-Willi syndrome and Noonan syndrome - systemic causes of cryptorchidism
- Prune belly syndrome, Beckwith-Wiedemann syndrome, congenital rubella, renal agenesis - associated anomalies
- Hypospadias - when combined with bilateral non-palpable testes, raises concern for DSD
Summary
Cryptorchidism results from disruption of either the INSL3-mediated transabdominal phase or the androgen/GFN-mediated inguinoscrotal phase of testicular descent. The inguinal canal is the most common arrest site (~80%). Histological damage begins at 6 months, making early intervention (orchiopexy by 6-12 months) essential. For palpable testes, routine US adds little clinical value. For non-palpable testes, MRI outperforms US, but diagnostic laparoscopy remains the definitive investigation and treatment tool. The cancer risk - driven by underlying testicular dysgenesis - persists even after orchiopexy and even affects the contralateral testis.
10 mark
Here is a structured 10-mark exam answer on cryptorchidism covering embryological and imaging considerations:
Cryptorchidism: Embryological and Imaging Considerations
Definition (0.5 marks)
Cryptorchidism refers to failure of one or both testes to descend into the scrotal sac. It affects ~30% of preterm and 3-5% of full-term male infants, falling to <1% by 1 year as most descend spontaneously.
Embryology of Testicular Descent (4 marks)
Normal Descent - Two Phases
Phase 1: Transabdominal (Weeks 8-15)
- Regulated by INSL3 (insulin-like factor 3) secreted by Leydig cells, acting via receptor RXFP2
- Also controlled by Müllerian-inhibiting substance (MIS/AMH) from Sertoli cells
- Gubernacular swelling draws the testis from the retroperitoneum to the inguinal brim
- Mutations in INSL3 or RXFP2 lead to cryptorchidism
Phase 2: Inguinoscrotal (Weeks 25-35)
- Regulated by androgens (testosterone/DHT via androgen receptor)
- Intact genitofemoral nerve (GFN) is essential; CGRP (calcitonin gene-related peptide) is the downstream mediator
- Gubernaculum is untethered distally; rapid transinguinal passage follows
- Majority of testes are scrotal by 27-32 weeks
Gonadal Differentiation Cascade
- SRY gene (Y chromosome) expressed at 40 days → activates SOX9 via SF1 → Sertoli cell differentiation
- Sertoli cells → testicular cord formation; Leydig cells → INSL3 and testosterone secretion
- Primordial germ cells migrate from yolk sac to testicular cords by 8 weeks
Sites of Arrest (in order of frequency)
- Inguinal canal (~80% - most common)
- Just outside the deep inguinal ring
- Abdominal (5-10%)
- Just above the scrotum
Ectopic testis = aberrant path after exiting the superficial ring (perineum, femoral canal, suprapubic region, base of penis)
Retractile testis = overactive cremaster; fully descendable on examination; no surgery needed
Pathological Consequences (1.5 marks)
Histological damage begins at 6 months and is pronounced by 2 years:
| Stage | Change |
|---|---|
| Early | Thickening of tubular basement membrane |
| Progressive | Loss of spermatogonia; Sertoli-cell-only pattern |
| Late | Tubular hyalinization, interstitial fibrosis; relatively prominent Leydig cells |
| Any stage | Germ cell neoplasia in situ (GCNIS) |
- The contralateral descended testis also shows similar changes in unilateral cryptorchidism - indicating an intrinsic gonadal dysgenesis, not purely a thermal/positional effect
- Associated conditions: inguinal hernia (10-20%), torsion, trauma, 4-10x increased cancer risk (seminoma most common)
Imaging Considerations (3 marks)
Ultrasound (US)
- High-resolution linear array transducer; search in transverse planes
- Begin by confirming bilateral absence from the scrotum
| Testis Location | US Sensitivity |
|---|---|
| Palpable inguinal | ~97% |
| Non-palpable | ~75% |
| Intra-abdominal | ~45% |
- AUA recommendation: Routine US should NOT be used for standard cryptorchidism - poor sensitivity, does not change management
- Exception: obese child where inguinal US may simplify surgical planning
- US role in DSD: detects Müllerian structures (uterus/fallopian tubes) to guide workup
MRI
- Far superior for localizing non-palpable, near-normal testes
- Preferred in: ambiguous genitalia, severe hypospadias, intra-abdominal testes not seen on US
- Cryptorchid testis appears hypoplastic with low T2 signal
- Small dysplastic testes may be indistinguishable from non-specific nodules
CT
- Advantage: retroperitoneal imaging
- Limited use in children due to radiation; 5 CT patterns described based on spermatic cord + testis morphology
Diagnostic Laparoscopy
- The definitive investigation for non-palpable testes
- Allows concurrent biopsy and surgical correction
- Makes preoperative imaging of limited additional value to patient management
Management Outline (1 mark)
- Observe until 1 year (spontaneous descent possible)
- Orchiopexy at 6-12 months if still undescended (before histological damage progresses)
- Non-palpable testes → laparoscopy:
- Blind-ending vessels = monorchia
- Vessels exiting internal ring = inguinal orchiopexy
- Intra-abdominal testis = Fowler-Stephens orchiopexy (two-stage) or laparoscopic orchiopexy
- Bilateral non-palpable → hCG stimulation test first to confirm viable testicular tissue
Key Points to Remember
- Two-phase descent: INSL3 (transabdominal) → Androgens/GFN (inguinoscrotal)
- Inguinal canal is the most common site of arrest
- Histological damage from 6 months → orchiopexy should not be delayed beyond 1 year
- Unilateral testicular agenesis is associated with ipsilateral renal agenesis (important for imaging workup)
- Cancer risk persists after orchiopexy and involves the contralateral testis too
- US is unreliable for non-palpable testes; laparoscopy is gold standard
Torsion vs epididymitis radiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive data from all key sources. Let me compile the full structured answer.
Testicular Torsion vs. Epididymitis: Radiological Differentiation
1. Clinical Context and Why Imaging Matters
Clinical examination can differentiate the two conditions in only ~50% of cases. Both present with acute scrotal pain and scrotal swelling, making radiology - primarily colour Doppler ultrasound (CDUS) - the cornerstone of differentiation. The stakes are high: testicular salvage in torsion drops from 80% at 6 hours to 20% if surgery is delayed beyond 24 hours.
Key principle: Surgery must NOT be delayed for imaging if torsion is clinically certain.
2. Ultrasound: The First-Line Modality
A high-resolution linear array transducer is used. The examination assesses:
- B-mode (grey-scale): testicular echotexture, size, epididymal appearance, hydrocele, scrotal wall
- Colour/power Doppler: intratesticular and epididymal blood flow
- High-resolution cord imaging (10-20 MHz): spermatic cord morphology
3. Comparative Radiological Features
A. Blood Flow on Colour Doppler (Most Critical Finding)
| Feature | Testicular Torsion | Epididymo-orchitis |
|---|---|---|
| Intratesticular flow | Absent or markedly reduced | Increased (hyperaemia) |
| Epididymal flow | Absent/reduced or occasionally increased (reactive) | Markedly increased - primary site |
| Comparison with contralateral testis | Asymmetrically reduced | Asymmetrically increased |
- Absent intratesticular flow on CDUS: 86% sensitive, 100% specific, 97% accurate for torsion and ischaemia
- Hyperaemia of epididymis +/- testis is the hallmark of epididymo-orchitis
- Caution: False negatives occur with CDUS in torsion - newer equipment may detect residual/collateral flow even in early torsion, and partial/intermittent torsion can show preserved flow
B. Spermatic Cord Signs (Pathognomonic of Torsion)
| Sign | Description | Performance |
|---|---|---|
| Whirlpool sign | Cord twist visible as a spiralling/snail-shaped mass (1-3 cm) on HRUS | Sensitivity 96%, specificity 99% |
| Snail sign | Hyperechoic central body with coiling of blood in the distal spermatic cord on CDUS | Pathognomonic of torsion |
| Linear cord | Normal linear cord on HRUS | 99% specificity for excluding torsion |
- In epididymitis, the cord appears normal with no twisting
- The whirlpool sign increases sensitivity from 76% (CDUS alone) to 96%
C. B-Mode Grey-Scale Appearances
| Feature | Testicular Torsion | Epididymo-orchitis |
|---|---|---|
| Testicular echogenicity | Enlarged, heterogeneous (late/necrotic) or normal (early) | Enlarged, uniformly hypoechoic (oedematous) or normal |
| Epididymis | Enlarged, altered echogenicity | Markedly enlarged, hyperechoic or hypoechoic, tender on probe pressure |
| Hydrocele | Reactive, may be present | Reactive hydrocele, common |
| Scrotal wall | Oedematous | Oedematous, thickened |
| Testicular position | May be high-riding, horizontal lie | Normal or low-lying |
- Heterogeneous parenchymal echogenicity = 100% necrosis at surgical exploration
- Homogeneous echogenicity predicts lower orchiectomy risk even with absent flow
- A hypoechoic, swollen testis with absent flow = likely non-salvageable
D. Epididymal Findings
| Feature | Torsion | Epididymitis |
|---|---|---|
| Epididymal size | Enlarged (secondarily) | Primarily enlarged - up to 2x normal |
| Epididymal vascularity | Absent/reduced (or occasionally increased due to reactive hyperaemia) | Markedly increased flow - earliest and most prominent sign |
| Pattern | Global changes | Starts at tail; may spread to body/head |
4. Scintigraphy (Radionuclide Scan)
Though largely superseded by CDUS, radionuclide imaging carries ~90% sensitivity and specificity:
- Torsion: Central photopenic ("cold") area with peripheral rim of increased activity
- Epididymitis: Diffuse increased ("hot") uptake throughout the scrotum
Drawbacks: lengthy, not readily available in emergencies, uses ionizing radiation.
5. MRI
Reserved for difficult diagnostic cases where CDUS is equivocal:
- Dynamic contrast-enhanced MRI: Shows absent perfusion in torsion
- Diffusion-weighted imaging (DWI): Torsed testis shows lower apparent diffusion coefficient (ADC) vs. normal (does not require gadolinium)
- Epididymitis on MRI: Enlarged, T2-hyperintense epididymis with enhancement on contrast sequences
6. Contrast-Enhanced Ultrasound (CEUS)
A newer modality showing promise:
- CDUS sensitivity/specificity: 76%/45%
- CEUS sensitivity/specificity: 96%/100% for testicular torsion
- Detects microvascular perfusion not visible on standard Doppler
- Useful when CDUS is inconclusive in the emergency setting
7. Torsion of Testicular Appendages (Important Differential)
The most common cause of acute scrotal pain in children:
- US: hypoechoic/avascular nodule at the upper pole or epididymis
- Surrounding reactive hyperaemia of normal epididymis/testis - can mimic epididymitis
- Testis and epididymis themselves show normal flow
- Kremasteric reflex is usually intact
8. Decision Rule Summary
Acute Scrotum
│
├─ Clinical suspicion of TORSION (high-riding testis, absent cremasteric reflex,
│ sudden onset, nausea/vomiting, horizontal lie)
│ │
│ ├─ HIGH suspicion → Immediate surgical exploration (do not delay for imaging)
│ │
│ └─ EQUIVOCAL → CDUS +/- HRUS cord imaging
│ │
│ ├─ Absent flow + whirlpool/snail sign → TORSION → OR
│ ├─ Normal flow + linear cord → NOT torsion
│ └─ Heterogeneous parenchyma + absent flow → Non-viable
│
└─ Gradual onset, fever, dysuria, intact cremasteric reflex → EPIDIDYMITIS
│
└─ CDUS: Increased epididymal flow → Epididymo-orchitis
Consider renal US in prepubertal boys (urinary anomaly screen)
9. Key Numbers to Remember
| Parameter | Value |
|---|---|
| Absent intratesticular flow (CDUS) for torsion | Sensitivity 86%, Specificity 100% |
| Whirlpool sign (HRUS) for torsion | Sensitivity 96%, Specificity 99% |
| CDUS alone (colour Doppler) | Sensitivity 76% |
| Salvage rate <6 hrs | 80% |
| Salvage rate >24 hrs | 20% |
| Salvage rate >48 hrs | ~10% |
| Radionuclide scan | Sensitivity/Specificity ~90% |
| CEUS for torsion | Sensitivity 96%, Specificity 100% |
10. Summary Comparison Table
| Radiological Feature | Torsion | Epididymitis |
|---|---|---|
| Intratesticular blood flow | Absent/reduced | Increased |
| Epididymal blood flow | Absent/reduced | Markedly increased |
| Cord morphology (HRUS) | Whirlpool/snail sign | Normal/linear |
| Testicular echogenicity | Heterogeneous (late) | Hypoechoic (uniform) |
| Epididymal size | Enlarged (secondary) | Primarily enlarged |
| Radionuclide scan | Cold (photopenic) | Hot (increased uptake) |
| MRI perfusion | Absent | Present, enhanced |
| DWI-ADC | Low (restricted diffusion) | Normal/high |
(Sources: Grainger & Allison's Diagnostic Radiology; Campbell-Walsh-Wein Urology)
This is a shared conversation. Sign in to Orris to start your own chat.