Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content to answer all 11 objectives. Let me compile the full, detailed answer.
Beta-Lactam Antibiotics - Complete Group Discussion Notes
Department of Pharmacology, Subharti Medical College, Meerut | 14.07.2026
Sources: Katzung's Basic & Clinical Pharmacology 16th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics
Objective 1: Classification of Beta-Lactam Antibiotics
Beta-lactam antibiotics share a core four-membered beta-lactam ring. They are classified into four major groups:
A. Penicillins
Classified by antimicrobial spectrum:
| Group | Drugs | Key Feature |
|---|---|---|
| Natural penicillins | Penicillin G (benzylpenicillin), Penicillin V | Highly active against Gram-positive cocci; hydrolyzed by penicillinase |
| Penicillinase-resistant | Nafcillin, Oxacillin, Dicloxacillin, Cloxacillin | Active against MSSA; resistant to S. aureus beta-lactamase |
| Aminopenicillins | Ampicillin, Amoxicillin | Extended to some Gram-negatives (H. influenzae, E. coli, Proteus mirabilis) |
| Extended-spectrum (antipseudomonal) | Piperacillin, Piperacillin/Tazobactam | Active against Pseudomonas, Klebsiella, Enterobacter |
B. Cephalosporins (5 generations)
| Generation | Examples | Spectrum |
|---|---|---|
| 1st | Cefazolin, Cephalexin | Gram-positive cocci, basic Gram-negatives |
| 2nd | Cefuroxime, Cefaclor, Cefoxitin (cephamycin) | Broader Gram-negative coverage |
| 3rd | Ceftriaxone, Cefotaxime, Ceftazidime, Cefixime | Extended Gram-negative; CSF penetration |
| 4th | Cefepime | Anti-pseudomonal + Gram-positive |
| 5th | Ceftaroline | Active against MRSA |
| Siderophore | Cefiderocol | Carbapenem-resistant organisms |
C. Carbapenems
Imipenem/Cilastatin, Meropenem, Ertapenem, Doripenem - broadest spectrum of all beta-lactams
D. Monobactams
Aztreonam - monocyclic ring; active only against aerobic Gram-negative rods; safe in penicillin allergy
E. Beta-Lactamase Inhibitors (combined with beta-lactams)
Clavulanic acid, Sulbactam, Tazobactam (older generation); Avibactam, Vaborbactam, Relebactam (newer generation)
Objective 2: Mechanism of Action of Beta-Lactams
Beta-lactams inhibit bacterial cell wall synthesis - they are bactericidal.
Step-by-step mechanism:
-
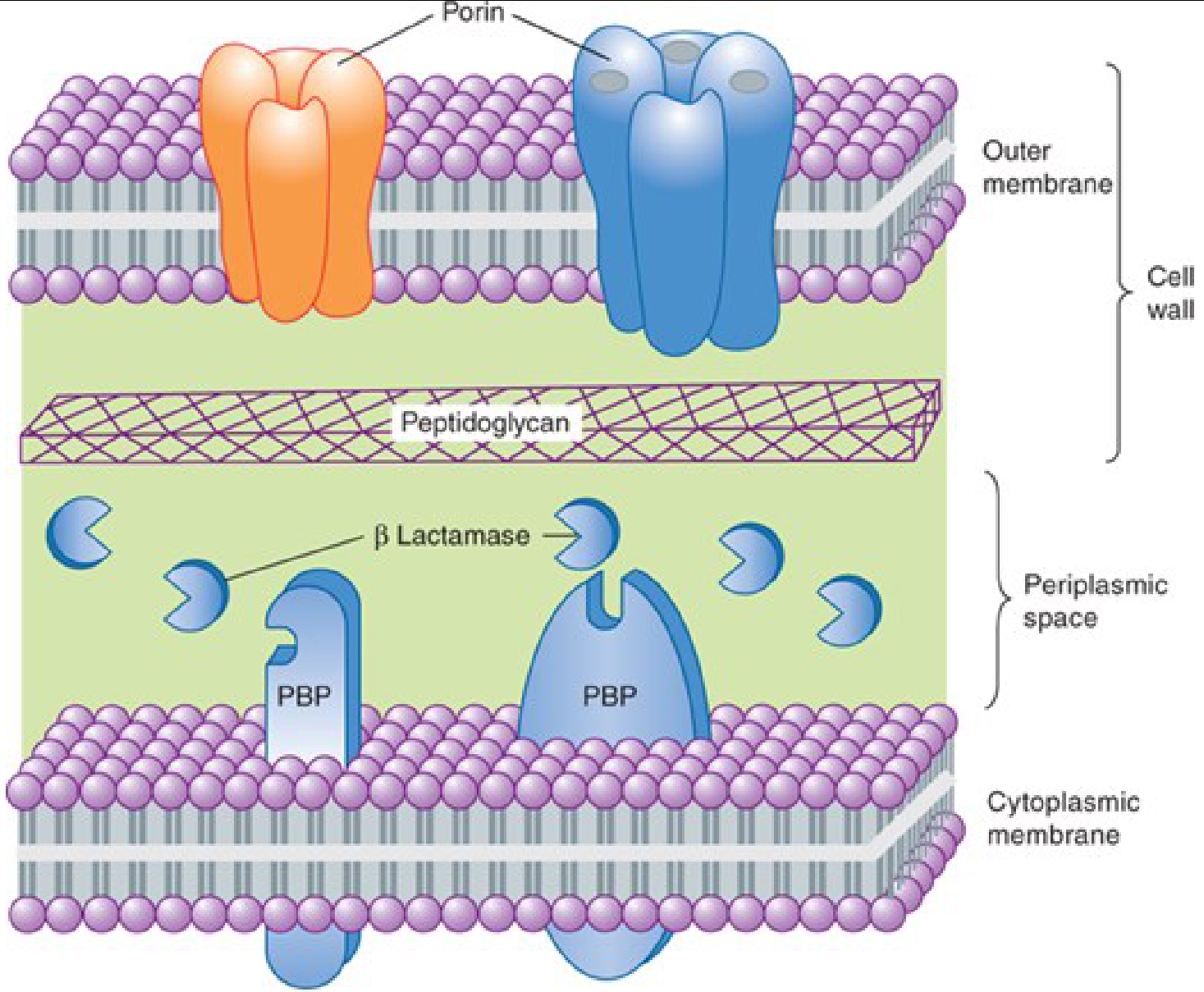
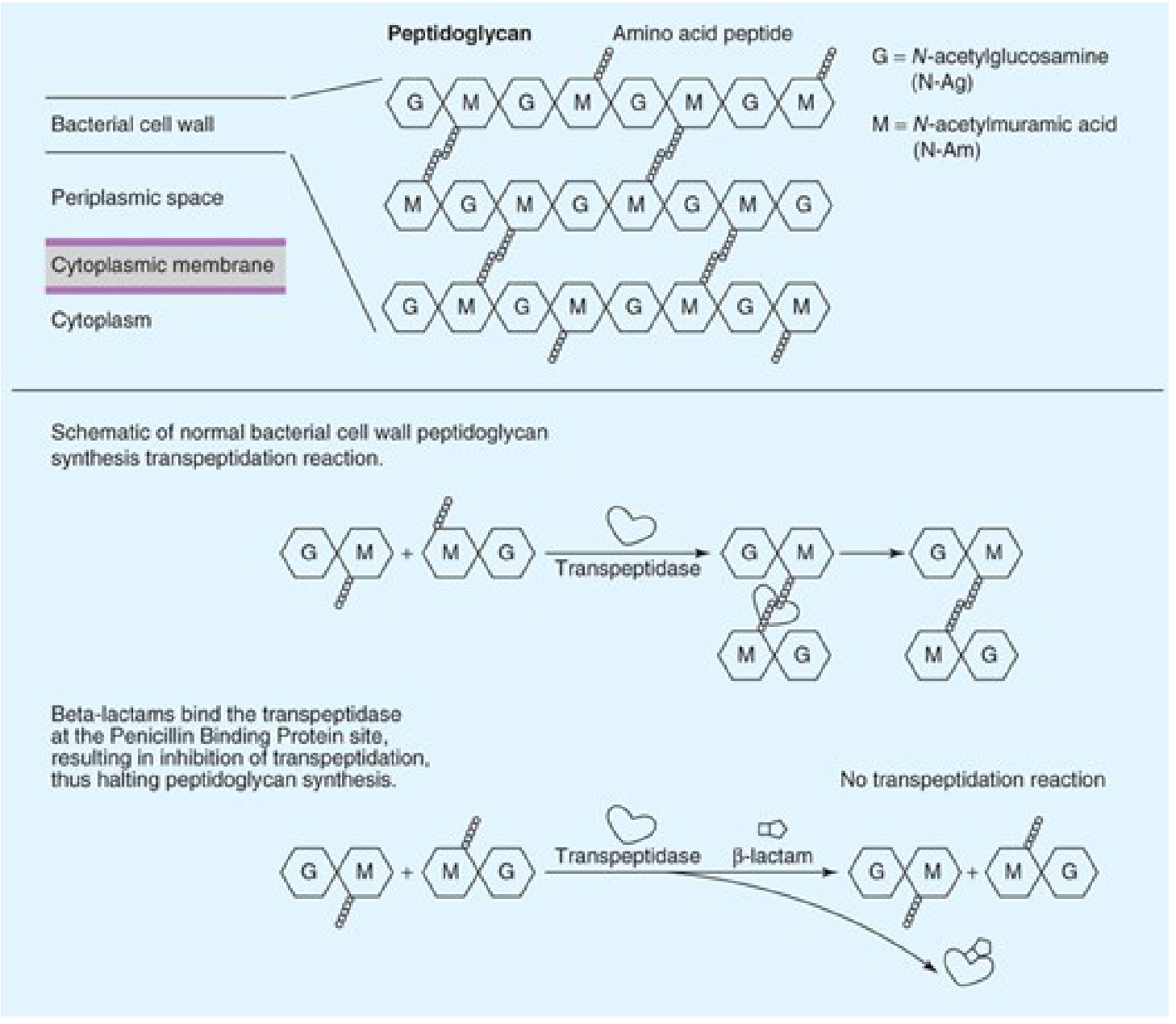
Target structure: Bacterial cell walls are made of peptidoglycan - long polymer chains of alternating N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) cross-linked by short peptides.
-
Normal synthesis: The enzyme transpeptidase (also called Penicillin-Binding Protein, or PBP) cross-links the peptide side chains of adjacent peptidoglycan strands - a process called transpeptidation. This cross-linking gives the cell wall its structural strength.
-
Beta-lactam action: Beta-lactam drugs are structural analogues of the D-Ala-D-Ala terminus of the peptide substrate. They bind covalently and irreversibly to the active site of PBPs (transpeptidases), inhibiting transpeptidation and halting peptidoglycan cross-linking.
-
Consequence: Incomplete cell wall formation leads to:
- Accumulation of cell wall precursors
- Activation of autolytic enzymes
- Osmotic lysis and cell death
Key point: Different beta-lactams have different binding affinities for different PBP subtypes, explaining differences in spectrum. Cephalosporins, for example, do NOT bind essential PBPs in Enterococcus spp., which is why the entire class lacks useful activity against enterococci. - Goodman & Gilman, p.1169
Objective 3: Antimicrobial Spectrum of Different Penicillins
| Penicillin | Gram-positive | Gram-negative | Anaerobes | Notes |
|---|---|---|---|---|
| Penicillin G/V | Streptococci, Pneumococci, Neisseria meningitidis, Treponema pallidum, Clostridium, Listeria | Limited | Good | Inactive against penicillinase-producing Staph |
| Nafcillin, Oxacillin, Dicloxacillin | MSSA, Streptococci | Minimal | No | "Antistaphylococcal" penicillins; NOT for MRSA |
| Ampicillin | Streptococci, Listeria | H. influenzae (non-BLPAR), E. coli, Proteus mirabilis, Salmonella, Shigella | Moderate | Inactivated by beta-lactamases |
| Amoxicillin | Similar to ampicillin | Similar | Moderate | Better oral bioavailability than ampicillin |
| Piperacillin | Streptococci | Pseudomonas aeruginosa, Klebsiella, E. coli, Enterobacter | Good (+ Bacteroides) | Broadest penicillin spectrum |
| Amoxicillin/Clavulanate | Staph (MSSA), Streptococci | H. influenzae, Moraxella, E. coli, Klebsiella | Bacteroides | Addition of clavulanate restores activity against beta-lactamase producers |
| Piperacillin/Tazobactam | Staph (MSSA), Streptococci | Pseudomonas, Klebsiella, E. coli, Enterobacter | Bacteroides | The broadest combination penicillin |
Objective 4: Mechanisms of Development of Resistance to Penicillins
Four general mechanisms of resistance to penicillins (and all beta-lactams):
1. Beta-Lactamase Production (Most Common)
- Bacteria produce beta-lactamase enzymes that hydrolyze the beta-lactam ring, inactivating the drug before it reaches its target PBP.
- Hundreds of different beta-lactamases are known:
- Narrow-spectrum: TEM-1, SHV-1 (plasmid-encoded, common in E. coli, Klebsiella)
- Extended-Spectrum Beta-Lactamases (ESBLs): Resistant to all penicillins and most cephalosporins
- AmpC beta-lactamases: Chromosomally encoded in Enterobacter, Citrobacter, Pseudomonas; resistant to cephamycins
- Carbapenemases (KPC, NDM, OXA): Hydrolyze even carbapenems
2. Modification of Target PBPs
- Altered PBPs with reduced affinity for beta-lactams; drug can no longer bind effectively.
- Classic example: MRSA - the mecA gene encodes a modified PBP (PBP2a) with very low affinity for all beta-lactams. This is why MRSA is resistant to ALL penicillins and most other beta-lactams.
3. Impaired Penetration to Target PBPs
- Gram-negative bacteria have an outer membrane that acts as a permeability barrier.
- Loss or mutation of porin proteins (e.g., OmpF, OmpC in E. coli) reduces drug entry into the periplasmic space, preventing access to PBPs.
4. Antibiotic Efflux
- Active efflux pumps expel beta-lactam molecules out of the bacterial cell before they can bind PBPs.
- Common in Pseudomonas aeruginosa (MexAB-OprM efflux system).
Katzung's Basic & Clinical Pharmacology 16th Ed., p.1240
Objective 5: Pharmacokinetics of Different Penicillins
Absorption
- Penicillin G: Destroyed by gastric acid - must be given parenterally (IV/IM). IV preferred as large IM doses cause irritation.
- Penicillin V: Acid-stable - can be given orally.
- Nafcillin: Erratic GI absorption - not suitable orally. Given IV.
- Dicloxacillin, Ampicillin, Amoxicillin: Acid-stable; well absorbed orally. Serum levels ~4-8 mcg/mL after 500 mg oral dose.
- Amoxicillin: Uniquely, absorption is NOT impaired by food; others should be given 1-2 hours before or after meals.
- Depot forms: Benzathine penicillin G (IM) - maintains levels >0.02 mcg/mL for 10 days (used for streptococcal infections, syphilis). Procaine penicillin - useful concentrations for 12-24 hours.
Distribution
- Penicillins are polar molecules - good extracellular distribution, poor intracellular penetration.
- Protein binding varies: Nafcillin (highly bound) vs. Penicillin G/Ampicillin (less bound). Higher binding = lower free drug concentration.
- CNS penetration: Poor in normal conditions. With inflamed meninges (meningitis), penicillin G at high doses (18-24 million units/day IV) achieves CSF levels of 1-5 mcg/mL - sufficient against pneumococci and meningococci.
- Also excreted into sputum and breast milk (3-15% of serum levels).
- Poor penetration: eye, prostate.
Elimination
- Primarily renal: ~90% via tubular secretion, ~10% glomerular filtration.
- Half-life: Penicillin G - ~30 minutes (normal); up to 10 hours in renal failure.
- Ampicillin and extended-spectrum penicillins - half-life ~1 hour.
- Dose adjustment required in renal impairment: Give ~1/4 to 1/3 of normal dose if creatinine clearance ≤10 mL/min.
- Exception: Nafcillin - excreted primarily by the liver (biliary); NO dose adjustment needed for renal failure.
- Probenecid blocks tubular secretion, prolonging penicillin half-life (used historically to maintain higher serum levels).
Objective 6: Important Therapeutic Uses of Penicillins
| Drug | Key Indications |
|---|---|
| Penicillin G | Streptococcal pharyngitis, pneumococcal pneumonia (susceptible strains), meningococcal meningitis, syphilis (all stages - drug of choice), leptospirosis, gas gangrene (Clostridium), tetanus adjunct, actinomycosis, diphtheria |
| Benzathine Pen G | Strep throat (single IM dose), prophylaxis of rheumatic fever, primary/secondary syphilis |
| Procaine Pen G | Uncomplicated pneumonia |
| Penicillin V (oral) | Mild streptococcal infections, prophylaxis of rheumatic fever |
| Nafcillin/Oxacillin | MSSA bacteremia, endocarditis, osteomyelitis, skin/soft tissue infections due to S. aureus |
| Dicloxacillin | Oral therapy for mild-moderate MSSA infections |
| Ampicillin | Listeria monocytogenes meningitis (drug of choice), enterococcal infections (with aminoglycoside), urinary tract infections, typhoid (historically) |
| Amoxicillin | Community-acquired pneumonia (S. pneumoniae), H. pylori eradication (triple therapy), otitis media, sinusitis, dental prophylaxis |
| Amoxicillin/Clavulanate | Bite wounds, sinusitis, otitis media, UTI, diabetic foot infections |
| Piperacillin/Tazobactam | Hospital-acquired pneumonia, intra-abdominal infections, febrile neutropenia (empiric), sepsis |
Objective 7: Adverse Effects of Penicillins
1. Hypersensitivity Reactions (Most Important)
- Most common cause of drug allergy.
- The beta-lactam ring opens and binds to proteins, forming haptens that trigger immune responses.
- Spectrum:
- Immediate (Type I, IgE-mediated): Anaphylaxis (0.01-0.05%), urticaria, angioedema, bronchospasm - can be fatal. Occurs within minutes.
- Accelerated: Urticaria within 1-72 hours.
- Delayed (Type IV): Maculopapular rash (most common overall reaction), occurs days later. Ampicillin/amoxicillin cause rash in ~5-8% of patients; nearly 100% of patients with infectious mononucleosis develop rash.
- Serum sickness (Type III): Fever, arthralgia, lymphadenopathy - less common.
- Cross-reactivity: ~1-2% cross-reactivity between penicillins and cephalosporins (share the beta-lactam ring). Historical estimates were higher but are now considered overestimates.
- Management: Skin testing; desensitization if drug absolutely needed.
2. Neurological Toxicity
- Seizures: High CSF concentrations (from excessive doses or failure to adjust for renal failure) can be epileptogenic. Risk is higher in patients with prior CNS disease.
- Intrathecal/intraventricular injection causes severe arachnoiditis or fatal encephalopathy - must be avoided.
- Procaine penicillin - Hoigne syndrome: Accidental IV injection causes dizziness, tinnitus, headache, hallucinations, seizures (from rapid liberation of toxic procaine concentrations).
- Benzathine penicillin G: Accidental IV injection associated with cardiorespiratory arrest and death - must always be given IM.
3. GI Effects
- Nausea, diarrhea (especially ampicillin - up to 5-10%).
- Clostridium difficile pseudomembranous colitis - disruption of normal GI flora. Can follow both oral and parenteral penicillins.
4. Hematological Effects
- Neutropenia and granulocytopenia - particularly with high-dose nafcillin (monitor CBC).
- Hemolytic anemia - high-dose IV penicillin G can cause positive Coombs test and hemolysis.
- Platelet dysfunction - especially piperacillin at high doses (inhibits ADP-mediated platelet aggregation).
5. Electrolyte Disturbances
- Large IV doses of sodium penicillin G or ticarcillin can cause hypernatremia, hypokalemia, and fluid overload.
6. Hepatotoxicity
- Nafcillin and oxacillin - cholestatic jaundice, elevated transaminases (monitor LFTs).
7. Nephrotoxicity (Interstitial Nephritis)
- Rare; most commonly associated with methicillin (now discontinued). Presents with hematuria, pyuria, eosinophilia, rising creatinine.
Objective 8: Spectrum of Activity and Uses of Different Cephalosporins
Cephalosporins are based on 7-aminocephalosporanic acid. Modifications at position 7 alter antibacterial activity; modifications at position 3 alter pharmacokinetics.
First-Generation
Drugs: Cefazolin (IV/IM), Cephalexin (oral), Cephradine
Spectrum:
- Excellent Gram-positive: MSSA, Streptococci
- Modest Gram-negative: E. coli, Klebsiella, Proteus mirabilis
- NOT: MRSA, Enterococcus, Pseudomonas, Anaerobes (Bacteroides)
Clinical uses:
- Surgical prophylaxis (drug of choice - cefazolin)
- Skin and soft tissue infections (MSSA)
- UTI
- NOT for empiric meningitis
Second-Generation
Drugs: Cefuroxime, Cefaclor, Cefprozil (oral); Cefoxitin, Cefotetan (cephamycins - have methoxy group at position 7)
Spectrum:
- Gram-positive coverage maintained (slightly less than 1st-gen)
- Extended Gram-negative: adds H. influenzae, Moraxella catarrhalis, Neisseria gonorrhoeae
- Cephamycins (Cefoxitin, Cefotetan): Good anaerobic coverage (Bacteroides fragilis) due to methoxy group
Clinical uses:
- Community-acquired respiratory infections, otitis media, sinusitis
- Cefoxitin/cefotetan: intra-abdominal and pelvic infections, surgical prophylaxis for colorectal surgery
Third-Generation
Drugs (IV): Ceftriaxone, Cefotaxime, Ceftazidime, Cefoperazone
Drugs (oral): Cefixime, Cefpodoxime, Ceftibuten, Cefdinir
Spectrum:
- Dramatically enhanced Gram-negative coverage including Enterobacterales
- Penetrates CSF well
- Ceftazidime: anti-pseudomonal activity; loses Gram-positive coverage
- Do NOT use for Enterobacter infections even if in vitro susceptible - risk of AmpC beta-lactamase induction and resistance emergence
Pharmacokinetics:
- IV infusion of 1 g produces serum levels 60-140 mcg/mL
- Ceftriaxone: Half-life 7-8 hours; once-daily dosing (1-2 g/day); biliary excretion - NO dose adjustment in renal failure
- Other 3rd-gen: renal excretion - require adjustment in renal insufficiency
Clinical uses:
- Meningitis (bacterial - pneumococcal, meningococcal, H. influenzae, Gram-negative rods) - ceftriaxone or cefotaxime
- Gonorrhea - IM ceftriaxone (drug of choice; cefixime no longer recommended due to resistance)
- Sepsis (empiric)
- Hospital-acquired infections
Fourth-Generation
Drug: Cefepime
Spectrum:
- Retains 3rd-gen Gram-negative coverage AND strong Gram-positive coverage
- Anti-pseudomonal
- More resistant to chromosomal AmpC beta-lactamases (vs. 3rd-gen)
- Half-life 2 hours; penetrates CSF; renal clearance
Fifth-Generation
Drug: Ceftaroline
- Active against MRSA (the key differentiator from all other cephalosporins)
- Good Gram-positive and Gram-negative coverage (except Pseudomonas)
- Used for: complicated skin/soft tissue infections, community-acquired pneumonia
Siderophore Cephalosporin
Drug: Cefiderocol
- Uses bacterial iron-transport systems (siderophore iron chelate) to penetrate outer membrane
- Active against carbapenem-resistant organisms including Pseudomonas, Acinetobacter, Klebsiella with KPC
Objective 9: Adverse Effects of Cephalosporins
-
Hypersensitivity reactions - Similar to penicillins but less frequent (~1-3%). Cross-reactivity with penicillin is ~1-2% (lower than previously believed). Anaphylaxis is rare. Maculopapular rash more common. Patients with penicillin allergy can generally receive cephalosporins with caution.
-
Cefazolin exception: Despite being a first-generation cephalosporin, cefazolin has very low cross-reactivity with penicillin allergy and is generally safe even in patients with documented penicillin allergy.
-
Nephrotoxicity: Older cephalosporins (cephaloridine, no longer available) were nephrotoxic. Current cephalosporins rarely cause direct nephrotoxicity, but can potentiate nephrotoxicity of aminoglycosides.
-
Bleeding diathesis (Hypoprothrombinemia): Cephalosporins with N-methylthiotetrazole (NMTT) side chain at position 3 (cefoperazone, cefamandole) - interfere with vitamin K metabolism, causing hypoprothrombinemia and potential bleeding. Also cause disulfiram-like reaction with alcohol.
-
Positive Coombs Test: High-dose cephalosporins can coat RBCs; hemolytic anemia is rare but reported.
-
Biliary sludge/pseudolithiasis: Ceftriaxone precipitates in bile as a calcium salt and can form biliary sludge or pseudolithiasis (especially in children, with high doses). Usually reversible on stopping drug.
-
GI effects: Diarrhea, C. difficile colitis (especially oral broad-spectrum cephalosporins; ceftriaxone is a known risk factor due to biliary excretion altering GI flora).
-
Neurotoxicity: Less common than with penicillins. High doses, especially with renal failure, can cause encephalopathy, myoclonus, seizures.
Objective 10: Carbapenems and Monobactams
Carbapenems
Structure: Modified beta-lactam with a bicyclic ring system; the 6-membered ring is unsaturated (unlike penicillins).
Drugs:
- Imipenem (given with cilastatin - a renal dehydropeptidase inhibitor that prevents renal tubular inactivation of imipenem)
- Meropenem - stable to renal dehydropeptidase; no need for cilastatin
- Ertapenem - once-daily dosing; NOT active against Pseudomonas or Acinetobacter
- Doripenem
Mechanism: Same as all beta-lactams - inhibition of transpeptidation via PBP binding. Carbapenems have exceptionally high affinity for multiple PBPs.
Spectrum: Broadest of all antibiotics. Cover:
- Gram-positive (including MSSA, Streptococci, Enterococcus - imipenem/meropenem)
- Gram-negative including Pseudomonas aeruginosa (imipenem, meropenem, doripenem - NOT ertapenem)
- Anaerobes (Bacteroides fragilis)
- Extended-spectrum beta-lactamase (ESBL)-producing organisms
- NOT active against: MRSA, VRE (generally), Stenotrophomonas maltophilia, fungi
Key resistance concern: Carbapenem-resistant organisms (CRE, CRKP) - producing carbapenemases (KPC, NDM, OXA-48)
Uses:
- Severe polymicrobial infections (intra-abdominal, pelvic)
- Hospital-acquired and ventilator-associated pneumonia
- Neutropenic fever (empiric therapy)
- ESBL-producing organism infections
- "Last resort" for multi-drug-resistant Gram-negatives
Adverse effects:
- Imipenem: Seizures (lowers seizure threshold - particularly at high doses/renal failure). Less common with meropenem.
- Nausea, vomiting (especially imipenem)
- Hypersensitivity (cross-reactivity with penicillin - use with caution)
Monobactams
Drug: Aztreonam
Structure: Monocyclic beta-lactam ring (no fused ring system) - unlike all other beta-lactams.
Spectrum: Exclusively aerobic Gram-negative rods (Enterobacterales, Pseudomonas aeruginosa). NO activity against:
- Gram-positive organisms
- Anaerobes
Key clinical advantage:
- No cross-reactivity with penicillin allergy (monocyclic structure; no shared antigenic determinants with penicillins or cephalosporins)
- Can be safely used in patients with severe penicillin or cephalosporin allergy when a Gram-negative coverage is needed
Uses:
- Aerobic Gram-negative infections in penicillin-allergic patients
- Urinary tract infections
- Pseudomonal infections (alternative when other beta-lactams cannot be used)
- Often combined with agents covering Gram-positive organisms (e.g., vancomycin) for broad coverage in penicillin-allergic patients
Pharmacokinetics: IV/IM; renal excretion; penetrates CSF with meningeal inflammation
Objective 11: Beta-Lactamase Inhibitors
Beta-lactamase inhibitors bind to beta-lactamases and protect the co-administered beta-lactam from enzymatic destruction. They have little to no intrinsic antibacterial activity.
Older Generation (Inhibit Plasmid-Encoded Beta-Lactamases)
| Inhibitor | Co-formulation | Notes |
|---|---|---|
| Clavulanic acid | Amoxicillin/clavulanate (oral), Ticarcillin/clavulanate (IV, not in US) | Irreversible, mechanism-based inhibitor; active against wide range of Gram-positive and Gram-negative beta-lactamases; oral and parenteral forms |
| Sulbactam | Ampicillin/sulbactam (IV/IM) | Also has intrinsic activity against Acinetobacter spp. - used at high doses for MDR Acinetobacter |
| Tazobactam | Piperacillin/tazobactam (IV), Ceftolozane/tazobactam (IV) | Good against plasmid-mediated ESBLs |
Limitation of older generation: Do NOT inhibit:
- AmpC chromosomal beta-lactamases (Enterobacter, Citrobacter, Pseudomonas)
- Carbapenemases (KPC, metallo-beta-lactamases)
Newer Generation (Broader Spectrum Inhibition)
| Inhibitor | Co-formulation | Activity |
|---|---|---|
| Avibactam | Ceftazidime/avibactam (IV), Aztreonam/avibactam | Non-beta-lactam (diazabicyclooctane structure); inhibits ESBLs, AmpC, and KPCs; NOT metallo-beta-lactamases |
| Relebactam | Imipenem/cilastatin/relebactam | Similar spectrum to avibactam; restores imipenem activity against resistant organisms |
| Vaborbactam | Meropenem/vaborbactam | Boronic acid-based; broad beta-lactamase inhibition similar to avibactam |
Clinical importance: Newer combinations are used for carbapenem-resistant Klebsiella pneumoniae (CRKP) and other MDR Gram-negative organisms that cannot be treated with older antibiotics.
Quick Summary Table: Key "One-Liners" for Exam
| Topic | Key Point |
|---|---|
| MOA of beta-lactams | Inhibit transpeptidase (PBP) → block peptidoglycan cross-linking → cell lysis |
| Most common resistance mechanism | Beta-lactamase production (hydrolysis of the beta-lactam ring) |
| MRSA resistance mechanism | Modified PBP2a (mecA gene) - low affinity for all beta-lactams |
| Drug of choice for syphilis | Benzathine Penicillin G |
| Drug of choice for Listeria meningitis | Ampicillin |
| Beta-lactam safe in PCN allergy | Aztreonam (no cross-reactivity) |
| Cephalosporin active against MRSA | Ceftaroline |
| Carbapenem NOT covering Pseudomonas | Ertapenem |
| Why imipenem given with cilastatin | Cilastatin inhibits renal dehydropeptidase that inactivates imipenem |
| Penicillin requiring NO renal dose adjustment | Nafcillin (hepatic excretion) |
| Ceftriaxone renal dose adjustment? | NOT required - biliary excretion |
| Ceftriaxone unique adverse effect | Biliary sludge/pseudolithiasis |
| Cefoperazone/cefamandole adverse effect | Hypoprothrombinemia + disulfiram-like reaction (NMTT side chain) |
| Sulbactam unique property | Intrinsic anti-Acinetobacter activity |
Sources: Katzung's Basic & Clinical Pharmacology 16th Ed., pp. 1239-1290 | Goodman & Gilman's Pharmacological Basis of Therapeutics, pp. 1169-1200
This is a shared conversation. Sign in to Orris to start your own chat.