Acute gastritis
Reading File
Finding Sources
Searching PubMed
"acute gastritis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough overview of acute gastritis drawn from Sleisenger & Fordtran, Robbins & Kumar Basic Pathology, Harrison's Principles (22nd Ed, 2025), and Tintinalli's Emergency Medicine.
Acute Gastritis
Definition
Acute gastritis is histologically documented inflammation of the gastric mucosa characterized by a neutrophilic infiltrate. It must be distinguished from "gastropathy," where mucosal injury and regeneration occur without significant inflammation, and from the endoscopic finding of mucosal erythema (which does not equal gastritis). - Harrison's Principles of Internal Medicine 22E, p. 2581
Note: The correlation between histologic findings, endoscopic appearance, and clinical symptoms is poor - there is no "typical" clinical picture.
Etiology and Classification (Harrison's Table 335-10)
I. Acute Gastritis
| Type | Examples |
|---|---|
| Acute H. pylori infection | Most common infectious cause; presents with sudden epigastric pain, nausea, vomiting |
| Bacterial (phlegmonous) | Group A Streptococci, gram-negative bacilli, anaerobes, Clostridium |
| Emphysematous (gas-forming) | C. perfringens, E. coli, S. aureus |
| Viral | CMV, HSV, norovirus |
| Fungal | Mucormycosis (immunocompromised) |
| Chemical/Toxic | NSAIDs, alcohol, corrosives (acids/bases) |
| Stress-related | Shock, trauma, burns, organ failure |
Pathogenesis
The gastric mucosa normally defends itself through:
- A mucus layer with neutral pH (bicarbonate secretion by foveolar cells)
- Rich mucosal blood supply to buffer back-diffusing protons
- Prostaglandin E2 and I2 (stimulated by COX enzymes) promoting mucus and bicarbonate secretion
Acute gastritis occurs when these defenses are overwhelmed:
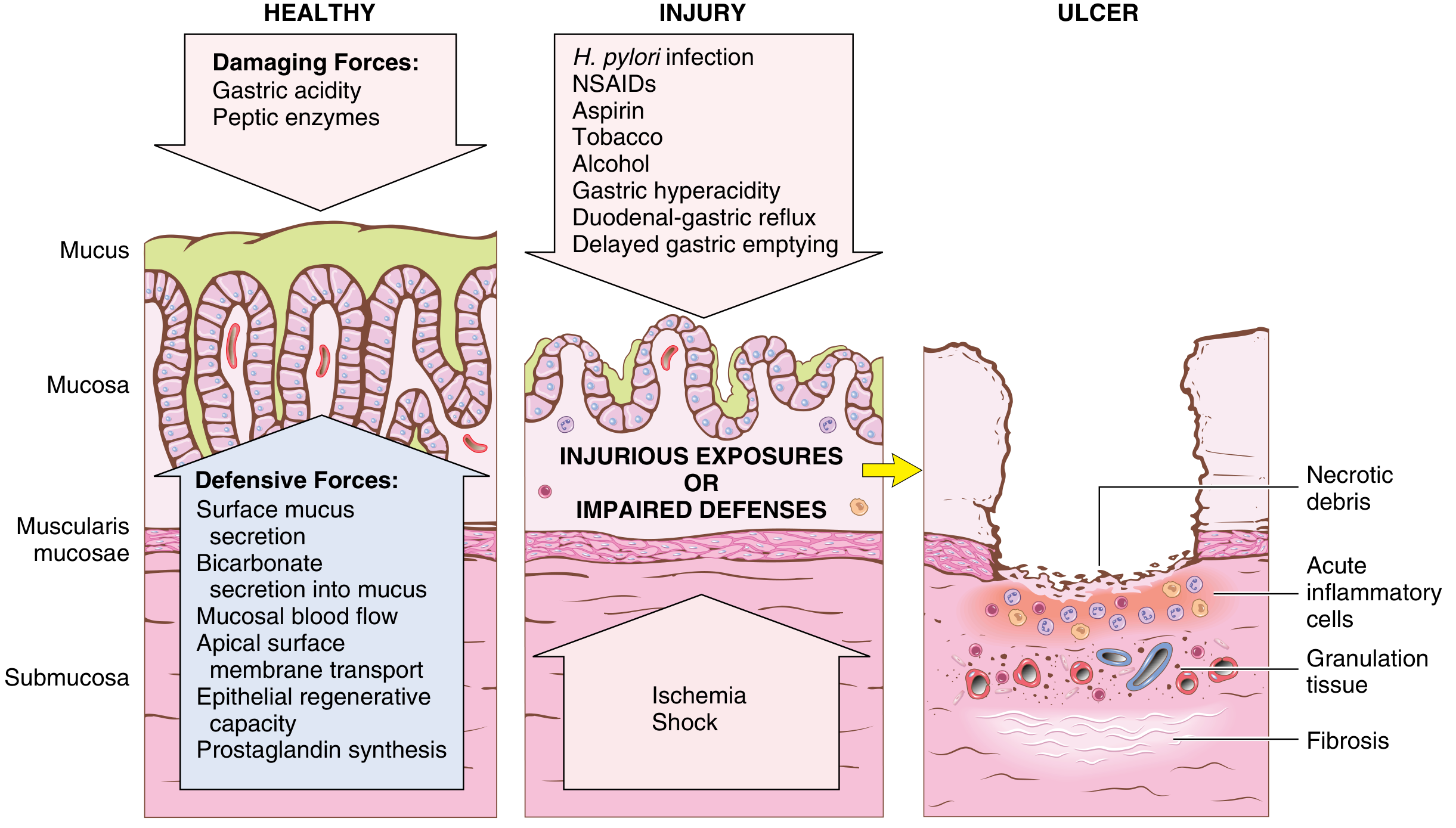
Mechanisms of gastric injury and protection (Robbins & Kumar Basic Pathology)
Key mechanisms:
- NSAIDs - inhibit COX-dependent prostaglandin synthesis, reducing mucosal blood flow and bicarbonate secretion
- H. pylori - urease generates ammonia, which inhibits gastric bicarbonate transporters and triggers neutrophil chemokine release
- Ischemia/stress - splanchnic vasoconstriction in critical illness reduces bicarbonate secretion; systemic acidosis lowers intracellular pH of mucosal cells
- Alcohol, radiation, chemotherapy - direct epithelial/stromal cell toxicity
- Ingestion of caustics - direct chemical injury
- Robbins & Kumar Basic Pathology, p. 553
Morphology (Histology)
- Mild/Gastropathy: Lamina propria edema, vascular congestion; surface epithelium intact, foveolar cell hyperplasia; neutrophils absent or sparse
- Active inflammation (acute gastritis proper): Neutrophils above the basement membrane in contact with epithelial cells - this is the hallmark
- Severe: Erosions, hemorrhage, or "acute erosive hemorrhagic gastritis" (concurrent erosion + hemorrhage)
Phlegmonous/suppurative gastritis (rare):
- Infection of submucosa and muscularis propria
- Edematous, thickened wall with polymorphonuclear infiltrate, gram-positive/gram-negative bacteria, vascular thrombosis, mucosal necrosis
Emphysematous gastritis (most severe):
- Gas-producing organisms (C. perfringens, E. coli, S. aureus)
- Gas visible in the stomach wall and portal venous system on CT
Stress-Related Mucosal Disease (Specific Type)
Occurs in critically ill patients:
- >75% of ICU patients develop endoscopically visible gastric lesions within 3 days
| Name | Location | Association |
|---|---|---|
| Stress ulcers | Stomach | Shock, sepsis, severe trauma |
| Curling ulcers | Proximal duodenum | Severe burns or trauma |
| Cushing ulcers | Stomach/duodenum/esophagus | CNS injury (stroke) - high perforation risk |
Pathogenesis: ischemia from hypotension/splanchnic vasoconstriction; Cushing ulcers additionally involve vagal stimulation causing acid hypersecretion. - Robbins & Kumar Basic Pathology, p. 553
Clinical Features
- Often asymptomatic
- Epigastric pain, nausea, vomiting, anorexia
- Hematemesis, melena, or massive hemorrhage (in erosive/hemorrhagic forms)
- Phlegmonous/emphysematous gastritis: septic appearance, acute upper abdominal pain, peritonitis, purulent ascitic fluid, fever, hypotension
Diagnosis
- Histology (endoscopic biopsy) is the gold standard - endoscopic appearance alone is insufficient
- H. pylori: urea breath test, stool antigen, or biopsy with urease test/culture
- Phlegmonous/emphysematous gastritis: CT scan (gas in stomach wall, portal vein gas), plain films, US; gastroscopy with biopsy/culture of gastric contents
- Acute H. pylori: histology shows marked neutrophilic infiltrate with edema and hyperemia
- Harrison's Principles of Internal Medicine 22E
Management
| Cause | Treatment |
|---|---|
| H. pylori | Triple or quadruple eradication therapy; if untreated, evolves into chronic active gastritis with lifelong infection |
| NSAIDs/alcohol | Discontinue offending agent; acid suppression (PPIs/H2 blockers) |
| Stress ulcers | PPIs or H2 antagonists for prophylaxis in ICU patients; treat underlying illness |
| Caustic ingestion | Supportive care; avoid emesis; urgent endoscopy within 12-24 hrs |
| Phlegmonous/emphysematous gastritis | Broad-spectrum IV antibiotics; surgical intervention may be required |
| CMV gastritis | Ganciclovir |
Complications and Progression
- Hypochlorhydria lasting up to 1 year after acute H. pylori infection
- Untreated H. pylori: chronic active gastritis → peptic ulcer disease → gastric adenocarcinoma or MALToma
- Phlegmonous gastritis can spread to liver/spleen, cause abscess; emphysematous gastritis can progress to gastric gas gangrene and death
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 909
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Robbins & Kumar Basic Pathology (Robbins Pathology) | Harrison's Principles of Internal Medicine 22E (2025) | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.