Biphasic isophane insulin injection I.p
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a thorough overview of Biphasic Isophane Insulin Injection (I.P.) drawn from authoritative pharmacology textbooks:
Biphasic Isophane Insulin Injection I.P.
What It Is
Biphasic isophane insulin is a premixed combination of:
- Soluble (regular) insulin - the short-acting component
- Isophane (NPH) insulin - the intermediate-acting component
The most common formulations are 70% NPH + 30% regular insulin (e.g., Humulin 70/30, Mixtard 30/70) and 50% NPH + 50% regular insulin. The "I.P." designation refers to the Indian Pharmacopoeia standard.
Composition and Rationale
| Component | Role | Onset | Peak | Duration |
|---|---|---|---|---|
| Soluble (regular) insulin (30%) | Prandial/bolus control - covers post-meal glucose rise | 30-60 min | ~2 h | 6-8 h |
| Isophane/NPH insulin (70%) | Basal control - fasting glucose between meals | 2-4 h | 6-7 h | 10-20 h |
| Biphasic combination | Dual-phase action | 30 min | Biphasic peaks | Up to ~24 h |
The combination gives a bimodal insulin action - an initial rapid peak from the soluble component followed by a sustained plateau/peak from the NPH component.
Mechanism of Action
Both components act via the same mechanism: binding to insulin receptors (receptor tyrosine kinase), which triggers:
- Increased glucose uptake by skeletal muscle and adipose tissue (via GLUT-4 translocation)
- Inhibition of hepatic glucose production (gluconeogenesis and glycogenolysis)
- Promotion of glycogen synthesis, lipogenesis, and protein synthesis
Pharmacokinetics
The "biphasic" profile arises because the two insulin types absorb at different rates from the subcutaneous injection site:
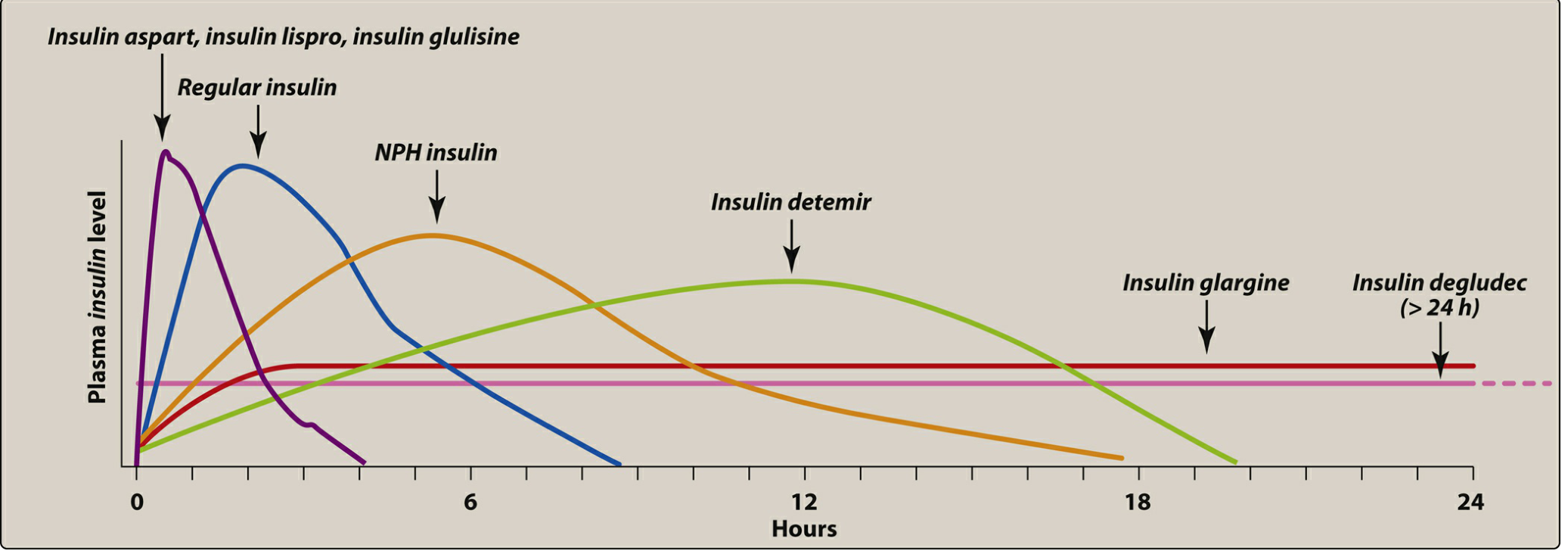
Figure: Plasma insulin levels over 24 hours for various insulin types (from Lippincott Pharmacology). NPH (isophane) is the orange curve peaking at ~5 h; regular insulin peaks earlier.
Route of Administration
Subcutaneous (SC) injection ONLY - NOT intravenous, NOT intramuscular
- NPH/isophane insulin forms a precipitate (a complex of insulin + zinc + protamine) at the injection site that slowly dissolves - this depot mechanism is destroyed if given IV.
- Regular insulin alone can be given IV (e.g., in DKA), but the premixed biphasic formulation must never be given IV.
- Inject SC in the abdomen, thigh, upper arm, or buttock; rotate injection sites.
- The vial must be gently rolled/mixed before injection as NPH settles - visible turbidity/cloudiness is normal.
Dosing and Administration
- Typically given twice daily: before breakfast and before the evening meal (dinner).
- The dose is individualized based on blood glucose monitoring.
- Inject 30 minutes before a meal (to allow the soluble component time to act on post-meal glucose).
- Dose intensification may be stepwise: once daily → twice daily → three times daily to achieve HbA1c targets.
Clinical trial data (INITIATE trial): In patients with T2DM not achieving targets on oral agents, premixed biphasic insulin given in a stepwise escalation protocol achieved HbA1c <7.0% in 77% of patients at 48 weeks. (Textbook of Family Medicine 9e)
Indications
- Type 2 diabetes mellitus (T2DM) - most common use, especially when patients need simplification of a basal + bolus regimen into twice-daily injections
- Type 1 diabetes - can be used but requires careful timing with meals
- Patients requiring fewer daily injections for adherence
Advantages
- Convenience - single injection delivers both prandial and basal coverage
- Fewer injections than a full basal-bolus regimen
- Useful in patients who cannot reliably draw up and mix their own insulins
Disadvantages
- Less flexible - cannot adjust the soluble and NPH components independently
- Fixed ratio may not suit all patients (e.g., those with variable meal sizes/times)
- Higher risk of hypoglycemia compared to basal-only regimens (especially if a meal is skipped)
- Should not be mixed with other insulins in the same syringe (especially long-acting analogs like glargine or detemir)
Precautions and Contraindications
| Situation | Note |
|---|---|
| Vial shows frosting/crystallization on sides | Do NOT use - insulin may be denatured |
| Renal impairment | Reduce dose by ~10%, monitor carefully (insulin cleared by kidneys) |
| Hypoglycemia unawareness | Intensive regimens not recommended |
| Diabetic ketoacidosis | Use IV regular insulin, NOT biphasic isophane |
| Pregnancy | Individual components (regular + NPH) preferred for tighter control |
Storage
- Unopened vials: refrigerate (2-8°C)
- In-use vials: can be kept at room temperature (up to 25-30°C) for up to 28-30 days
- Never freeze; avoid direct sunlight
Comparison with Analog Premixes
| Preparation | Components | Onset |
|---|---|---|
| Biphasic isophane 70/30 (I.P.) | 70% NPH + 30% regular | ~30 min |
| Biphasic insulin aspart 70/30 | 70% NPH aspart + 30% aspart | ~10-15 min (faster) |
| Biphasic insulin lispro 75/25 | 75% NPH lispro + 25% lispro | ~10-15 min (faster) |
Analog premixes (aspart, lispro-based) have a faster onset and can be injected closer to meals or even just after starting a meal, whereas human biphasic isophane requires a 30-minute pre-meal window.
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Section on Insulin Preparations (pp. 804-807)
- Katzung's Basic and Clinical Pharmacology 16th Edition, Chapter 41 - Pancreatic Hormones
- Textbook of Family Medicine 9e, Chapter 34 - Diabetes Management
Used for what mainly
Biphasic isophane insulin injection is used mainly for Type 2 Diabetes Mellitus (T2DM).
Specifically, it is chosen when:
- A patient with T2DM is not achieving adequate glucose control on oral antidiabetic drugs alone and needs insulin to be started
- The goal is simplicity - one injection covers both the meal-time (prandial) glucose spike AND the background (basal) glucose, instead of needing separate injections for each
- The patient needs twice-daily dosing (before breakfast + before dinner) rather than a more complex 3-4 injection basal-bolus regimen
In simple terms:
| Need | Component that covers it |
|---|---|
| Post-meal glucose spike | Soluble (regular) insulin - 30% |
| Fasting/between-meal glucose | Isophane (NPH) insulin - 70% |
Both are delivered in one injection, twice a day.
Secondary uses:
- Type 1 diabetes - less commonly, where flexibility is less critical
- Patients transitioning from oral drugs to insulin for the first time
- Elderly or non-adherent patients where fewer injections improve compliance
The primary target condition is always diabetes mellitus - it is not used for any other disease. It does not cure diabetes; it controls blood glucose levels to prevent long-term complications like retinopathy, nephropathy, and neuropathy.
Is used for fast or slow glucose
Biphasic isophane insulin is used for BOTH - that is exactly why it is called "biphasic" (two phases).
Two phases of action:
Phase 1 - FAST (Soluble/Regular insulin - 30%)
- Kicks in within 30 minutes
- Covers the quick rise in blood glucose after eating (post-meal spike)
- This is the "fast" component
Phase 2 - SLOW (Isophane/NPH insulin - 70%)
- Starts working at 2-4 hours
- Covers background glucose between meals and overnight (fasting glucose)
- This is the "slow/sustained" component
Simple analogy:
Think of it like a two-stage rocket:
| Stage | Insulin | When it works | What it controls |
|---|---|---|---|
| 1st stage (fast) | Regular (30%) | 30 min - 6 h | Post-meal glucose |
| 2nd stage (slow) | NPH/Isophane (70%) | 2 h - 20 h | Fasting/basal glucose |
Important point:
- If you need only fast glucose control (e.g., DKA emergency) - you use plain regular insulin IV, NOT biphasic isophane
- Biphasic isophane is specifically designed for routine twice-daily use where both fast and slow control are needed together in one injection
So the answer is: both fast AND slow, combined in a single injection.
Why we use this drugs in detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Here is a detailed explanation of why we use biphasic isophane insulin, from the ground up:
WHY WE USE BIPHASIC ISOPHANE INSULIN - In Detail
STEP 1: Understand the Disease First - Diabetes Mellitus
The human body normally produces insulin from beta cells in the pancreas. Insulin's job is to act like a "key" - it unlocks cells to let glucose (sugar from food) enter them. Cells then use glucose for energy.
In diabetes, this system breaks down:
| Type | What goes wrong |
|---|---|
| Type 1 DM | Immune system destroys all beta cells - zero insulin produced |
| Type 2 DM | Beta cells produce less and less insulin over time + body cells become resistant to insulin's action |
Result in both cases: Glucose cannot enter cells properly → Blood glucose rises dangerously high → Hyperglycemia
STEP 2: Why High Blood Glucose is Dangerous
Persistent hyperglycemia causes damage throughout the body:
Microvascular (small vessel) damage:
- Retinopathy - blindness from damage to eye blood vessels
- Nephropathy - kidney failure from damage to kidney filtration vessels
- Neuropathy - nerve damage causing pain, numbness, foot ulcers, amputation
Macrovascular (large vessel) damage:
- Coronary heart disease - heart attacks (leading cause of death in T2DM)
- Cerebrovascular disease - strokes
- Peripheral artery disease - poor circulation to legs
The goal of insulin therapy is to bring blood glucose back to normal range to PREVENT all these complications.
STEP 3: Why Can't We Just Use Tablets/Oral Drugs?
Oral drugs (metformin, sulfonylureas, etc.) work by:
- Stimulating the remaining beta cells to produce more insulin, OR
- Making body cells more sensitive to whatever insulin is present
But they only work if there are still functioning beta cells producing some insulin.
We need to START insulin when:
- Type 1 DM - no beta cells at all, oral drugs are completely useless
- Type 2 DM where oral drugs have failed - beta cells have become exhausted after years of overwork
- HbA1c remains above target (>7-8%) despite maximum doses of oral drugs
- Acute situations - surgery, severe infections, pregnancy, DKA, HHS
- Very high initial blood glucose (>300 mg/dL) at diagnosis
STEP 4: Why Specifically Biphasic Isophane (and not just any insulin)?
Normal healthy pancreas releases insulin in two patterns every day:
| Pattern | When | Purpose |
|---|---|---|
| Basal insulin | Continuously, 24 hours | Keeps fasting blood glucose stable between meals and overnight |
| Bolus (prandial) insulin | Sharp spike after every meal | Handles the sudden surge of glucose absorbed from food |
To properly replace this, ideally you need both components. Options are:
Option A - Full Basal-Bolus Regimen:
- Long-acting insulin once/twice daily (basal) PLUS
- Rapid-acting insulin before EVERY meal (bolus)
- = 4-5 injections per day
- Very effective but complex, requires patient education, frequent glucose monitoring
Option B - Biphasic Isophane Insulin (Premixed):
- ONE injection contains BOTH the fast-acting (bolus) AND slow-acting (basal) components
- Given TWICE daily (before breakfast + before dinner)
- = Only 2 injections per day
- Simpler, more convenient, better compliance
STEP 5: The Specific Reasons We Choose Biphasic Isophane
1. To Mimic Natural Insulin Secretion (Simplified)
The body needs insulin working at multiple times. Biphasic gives:
- Soluble component (30%) - acts fast to cover the meal you are about to eat
- NPH component (70%) - works slowly to cover glucose between meals
2. To Achieve HbA1c Targets
HbA1c (glycated haemoglobin) reflects average blood glucose over 3 months. The target is <7% for most diabetic patients. Clinical trials show biphasic insulin effectively achieves this:
- The INITIATE trial showed 77% of patients achieved HbA1c <7% with premixed biphasic insulin in 48 weeks
3. To Prevent Long-Term Complications
Research (DCCT trial for T1DM, UKPDS for T2DM) proved that tight glucose control significantly reduces:
- Retinopathy by 76%
- Nephropathy by 50%
- Neuropathy by 60%
Biphasic insulin is one of the tools used to achieve this tight control.
4. Patient Convenience and Compliance
- Elderly patients, rural patients, or those with limited education find it hard to manage 4-5 injections
- Two injections daily = better real-world adherence
- Less chance of mixing errors (it comes pre-mixed)
5. When the Pancreas Can No Longer Help
In advanced T2DM, beta cells are so exhausted they produce almost no insulin. At this point, the body is entirely dependent on exogenous (injected) insulin to survive and prevent life-threatening hyperglycemia.
STEP 6: What Happens If We Do NOT Give Insulin When Needed?
| Short term | Long term |
|---|---|
| Blood glucose goes dangerously high | Blindness |
| Diabetic Ketoacidosis (DKA) in T1DM | Kidney failure requiring dialysis |
| Hyperosmolar Hyperglycemic State (HHS) in T2DM | Heart attacks and strokes |
| Coma and death | Amputations |
| Severe dehydration | Premature death |
Summary in One Sentence:
We use biphasic isophane insulin because the diabetic pancreas cannot produce enough insulin on its own, and without replacing it, blood glucose stays dangerously high, destroying the kidneys, eyes, nerves, and heart over time - biphasic isophane provides both fast and slow insulin coverage in just two daily injections, making life-saving glucose control practical for everyday patients.
(Sources: Lippincott Illustrated Reviews Pharmacology; Rosen's Emergency Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; Fuster & Hurst's The Heart)
Can it relate with drug abuser (ganja)
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
cannabis marijuana insulin glucose diabetes
Reading Article
PMID: 37526051
Finding Sources
Finding Sources
Finding Sources
This is a very interesting clinical question. Here is a detailed answer:
Biphasic Isophane Insulin and Ganja (Cannabis) Use - The Relationship
Direct Answer
Yes - there IS a clinically important relationship, but it is complex. Ganja (cannabis/marijuana) affects blood glucose, insulin sensitivity, appetite, and the pancreas - all of which directly impact how biphasic isophane insulin works in the body.
1. HOW CANNABIS AFFECTS BLOOD GLUCOSE
Short-term (while high/intoxicated):
- THC (main active compound) activates cannabinoid receptors (CB1 and CB2) in the pancreas, liver, and brain
- This can cause acute hypoglycemia (low blood sugar) in people taking insulin
- The person may feel dizzy, confused, sweaty - but mistake it for being "high"
- This is DANGEROUS - a ganja user on insulin may not recognize hypoglycemia because symptoms overlap with cannabis intoxication
Long-term heavy use:
- Cannabis causes "munchies" - intense hunger and overeating, especially carbohydrates/sweets
- This causes unpredictable spikes in blood glucose
- Makes it very hard to control glucose with a fixed-ratio premixed insulin like biphasic isophane
2. CANNABIS AND INSULIN RESISTANCE
| Effect | Mechanism |
|---|---|
| Acute use - may INCREASE insulin sensitivity temporarily | CB1 receptor activation in muscle and fat cells |
| Chronic heavy use - associated with weight gain, increased appetite | Leads to insulin resistance over time |
| Cannabinoid hyperemesis syndrome - vomiting | Causes missed meals → dangerous hypoglycemia if insulin already injected |
3. LATEST RESEARCH FINDING (2023 Meta-Analysis)
A systematic review and meta-analysis (Mousavi et al., 2023) of 7 studies found:
Cannabis users had 52% LOWER odds of developing Type 2 DM compared to non-users (OR = 0.48, 95% CI: 0.39-0.59)
BUT - this does NOT mean ganja is beneficial for diabetics on insulin. This is a population-level association, not a treatment recommendation. The reasons are:
- Cannabis users tend to be younger and leaner
- Heavy chronic use carries many other harms
- Study heterogeneity was considerable
- Interaction with insulin is still dangerous
4. THE BIG DANGER: UNPREDICTABLE GLUCOSE SWINGS
Biphasic isophane insulin works on a fixed, predictable schedule:
- Inject at a set time
- Eat a meal at a set time
- Glucose rises and falls predictably
Ganja completely disrupts this:
| Cannabis Effect | Impact on Insulin Control |
|---|---|
| Causes hunger (munchies) → eats more carbs | Blood glucose spikes higher than insulin can cover |
| Causes nausea/vomiting (sometimes) | Glucose drops but insulin still active → hypoglycemia |
| Impairs judgement and memory | May forget to inject insulin, or inject twice by mistake |
| Alters perception of symptoms | Cannot feel/recognize hypoglycemia properly |
| Causes irregular sleep/wake cycles | Disrupts meal timing → unpredictable glucose |
| Increases heart rate | Mimics hypoglycemia symptoms - confusion about actual glucose level |
5. SPECIFIC RISKS IN A GANJA ABUSER ON BIPHASIC INSULIN
Risk 1 - Severe Hypoglycemia
- Person smokes ganja → gets hungry → eats a lot → takes extra insulin
- OR smokes ganja → falls asleep, misses meal → insulin is still working → blood glucose crashes
- Ganja masks the warning signs (sweating, trembling, confusion) that normally alert you to low glucose
Risk 2 - Diabetic Ketoacidosis (DKA)
- Heavy cannabis use causes nausea and vomiting (cannabinoid hyperemesis)
- Patient vomits meal but insulin is already injected and absorbed
- Patient also skips doses because of altered mental state
- Result: blood glucose rises dangerously, ketones build up → DKA
Risk 3 - Poor Medication Adherence
- Cannabis impairs memory and motivation
- Ganja abusers are significantly more likely to miss insulin doses
- Inconsistent injection timing with biphasic insulin causes complete loss of glucose control
Risk 4 - Drug Interaction with Symptoms
- Both cannabis intoxication AND hypoglycemia cause: dizziness, confusion, fast heart rate, sweating
- The user may not seek medical help because they think they are just "high"
- This can lead to coma or death from unrecognized hypoglycemia
6. BOTTOM LINE
| Question | Answer |
|---|---|
| Does ganja directly react chemically with insulin? | No direct pharmacological interaction |
| Does ganja affect glucose control? | YES - makes it highly unpredictable |
| Can a ganja abuser use biphasic insulin safely? | With great difficulty - very high risk |
| What is the main danger? | Unrecognized hypoglycemia (masked by cannabis high) |
| What should be done? | Glucose monitoring every time; ideally stop cannabis; switch to flexible basal-bolus regimen with close medical supervision |
Clinical Advice:
A ganja abuser on biphasic isophane insulin must:
- Monitor blood glucose frequently (cannot rely on symptoms)
- Never skip meals after injecting
- Carry glucose tablets at all times
- Inform their doctor about cannabis use for proper insulin dose adjustment
- Ideally, stop cannabis - it makes diabetes management extremely dangerous
(Source: Mousavi et al., Phytotherapy Research 2023, PMID: 37526051; Lippincott Illustrated Reviews: Pharmacology)
Can it will lead to death if I skip or high or low dose
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
YES - absolutely yes. All three scenarios (skipping, too high a dose, too low a dose) can lead to death. Here is the full medical explanation:
⚠️ Can Wrong Insulin Dosing Lead to Death?
SCENARIO 1 - SKIPPING THE DOSE
What happens:
- No insulin in the body → glucose cannot enter cells
- Blood glucose rises rapidly → Hyperglycemia
- Body starts breaking down fat for energy → produces ketones (acid waste)
- Ketones build up in blood → blood becomes acidic → Diabetic Ketoacidosis (DKA)
The death pathway:
Skip insulin → Blood glucose >300 mg/dL
↓
Ketones build up → Blood pH drops (acidosis)
↓
Severe dehydration, vomiting, confusion
↓
Coma → Multi-organ failure → DEATH
Medical facts (Goldman-Cecil Medicine):
- DKA and Hyperosmolar Hyperglycemic State (HHS) are the most serious acute complications of diabetes
- The most common cause of DKA is "nonadherence with insulin therapy" (skipping doses)
- Untreated DKA has near 100% mortality
- Even with treatment, DKA mortality ranges 1-5%
SCENARIO 2 - TOO HIGH A DOSE (Overdose)
What happens:
- Excess insulin removes too much glucose from blood → Severe Hypoglycemia
- Brain has NO glucose to function (brain runs ONLY on glucose)
- Brain starts shutting down
The death pathway:
Too much insulin → Blood glucose <40 mg/dL
↓
Brain starved of glucose → Seizures
↓
Massive adrenaline surge → Ventricular arrhythmia (heart rhythm disturbance)
↓
Cardiac arrest → DEATH
Medical facts (Goldman-Cecil Medicine textbook, exact quote):
"An episode of severe hypoglycemia can be the immediate cause of death in people with type 1 diabetes, with reported mortality rates ranging from 4 to 10%. Prolonged episodes of very low glucose (<15 mg/dL) can themselves cause significant brain damage, but death due to fatal hypoglycemia may be the result of other mechanisms, such as ventricular arrhythmias precipitated by large catecholamine surges and concurrent electrolyte disturbances."
Glucose levels and brain effects:
| Blood Glucose Level | What Happens to the Brain |
|---|---|
| 70 mg/dL | Symptoms begin - sweating, trembling |
| 50 mg/dL | Confusion, inability to think clearly |
| 30-40 mg/dL | Seizures, loss of consciousness |
| <15 mg/dL | Permanent brain damage |
| Prolonged <15 mg/dL | Death |
SCENARIO 3 - TOO LOW A DOSE (Under-dosing)
What happens:
- Not enough insulin → blood glucose stays persistently high (chronic hyperglycemia)
- This is a slower death compared to the above two, but just as certain
Short-term danger:
- Glucose >600 mg/dL → Hyperosmolar Hyperglycemic State (HHS)
- Blood becomes very thick and concentrated
- Severe dehydration → clots form → strokes, heart attacks
- Coma and death, especially in elderly patients
Long-term (months to years) damage from under-dosing:
| Organ | Damage |
|---|---|
| Kidneys | Kidney failure → dialysis |
| Eyes | Retinopathy → blindness |
| Heart | Heart attack (leading cause of death in T2DM) |
| Brain | Stroke |
| Feet/Legs | Gangrene → amputation |
| Nerves | Painful neuropathy, loss of sensation |
Summary Table: All Three Scenarios
| Situation | Immediate Result | If Untreated | Death Risk |
|---|---|---|---|
| Skip dose | DKA / HHS | Coma, multi-organ failure | Very High - near 100% if untreated |
| Too high dose | Severe hypoglycemia | Brain damage, cardiac arrest | 4-10% per severe episode |
| Too low dose (chronic) | Persistent hyperglycemia | Organ failure, stroke, heart attack | Slow but certain - years |
Special Warning: Ganja + Wrong Insulin Dose = Maximum Danger
Combining cannabis with any of these three errors makes it far worse:
- Ganja masks the warning signs of hypoglycemia
- Ganja impairs judgement → more likely to get the dose wrong
- Ganja-induced vomiting → skipped meal after injection → severe hypoglycemia
- Person may be unconscious and family/friends think they are just "high" and do not call for help in time → fatal delay
The single most important rule:
Biphasic isophane insulin must ALWAYS be taken with food, at the right dose, at the right time. It is not optional. Missing or wrong dosing is a life-or-death matter.
(Source: Goldman-Cecil Medicine International Edition, Chapter 210 - Diabetes Mellitus)
This is a shared conversation. Sign in to Orris to start your own chat.