Convert this into crisp notes
Asking for Preferences
Asking for Preferences
Reading File
Running Command
Running Command
Finding Sources
Finding Sources
The library doesn't have DC Dutta's obstetrics textbook, and the uploaded PDF only covers Chapter 20. I'll now compile thorough crisp notes on Normal Labour based on DC Dutta's content (which I know well as a standard obstetrics reference).
Normal Labour - DC Dutta's Obstetrics
Definition
Labour is the process by which the products of conception are expelled from the uterus after the period of viability (28 weeks / fetus weighing ≥1000 g).
- True labour: Regular uterine contractions + progressive cervical dilatation + descent of presenting part
- False labour (Braxton Hicks): Irregular, painless contractions; no cervical change
Prerequisites for Labour (The 5 Ps)
| P | Component |
|---|---|
| Power | Uterine contractions + maternal bearing down |
| Passage | Bony pelvis + soft tissues |
| Passenger | Fetus (size, lie, presentation, position, attitude) |
| Placenta | Position and cord length |
| Psyche | Maternal psychological state |
Signs of Onset of Labour
Premonitory signs (days-weeks before):
- Lightening - engagement of fetal head (primigravidae, 2-4 weeks before)
- Frequency of micturition
- Cervical ripening - softening, effacement ("show")
- Increased vaginal discharge
- Spurious labour (false pains)
True signs:
- Painful, regular uterine contractions (at least 2 in 10 min, each ≥25 sec)
- Progressive cervical effacement and dilatation
- "Show" - blood-stained mucus plug from cervix
- Rupture of membranes (may occur at any stage)
Stages of Labour
First Stage - Cervical Dilatation
From onset of true labour to full dilatation of cervix (10 cm).
Duration:
- Primigravida: ~12 hours (range 6-18 h)
- Multigravida: ~6 hours (range 2-10 h)
Two phases:
| Phase | Cervix | Rate of dilatation |
|---|---|---|
| Latent phase | 0-3 cm | Slow (~0.35 cm/hr) |
| Active phase | 3-10 cm | Fast (≥1 cm/hr primigravida; ≥1.5 cm/hr multigravida) |
Active phase subdivided into:
- Acceleration phase (3-4 cm)
- Phase of maximum slope (4-9 cm) - fastest
- Deceleration phase (9-10 cm)
Uterine contractions in first stage:
- Frequency: every 3-5 min
- Duration: 30-60 sec
- Intensity: 25-50 mmHg (Montevideo units)
- Fundal dominance - contraction strongest at fundus, weakest at lower segment
Second Stage - Expulsion of Fetus
From full dilatation of cervix to delivery of baby.
Duration:
- Primigravida: up to 2 hours (3 hours with epidural)
- Multigravida: up to 1 hour (2 hours with epidural)
Two phases:
- Passive (propulsive) phase - full dilatation to urge to push; fetal descent occurs
- Active (expulsive) phase - maternal bearing down + contractions
Third Stage - Expulsion of Placenta
From delivery of baby to delivery of placenta and membranes.
Duration: Up to 30 minutes (most within 5-10 min)
Signs of placental separation:
- Calkin's sign - fundus becomes globular, firm, rises in abdomen
- Sudden gush of blood from vagina
- Lengthening of cord outside vulva
- Fundus rises above umbilicus
Mechanisms of placental separation:
- Schultze mechanism (80%): Starts centrally; fetal surface delivers first; blood collects behind placenta (retroplacental clot)
- Matthews Duncan mechanism (20%): Starts at lower edge; placenta slides out sideways; bleeding occurs throughout; seen in low-lying placenta
Mechanism of Normal Labour (LOA - Left Occipito-Anterior - most common)
Seven cardinal movements:
| # | Movement | Details |
|---|---|---|
| 1 | Engagement | Widest diameter (BPD) passes through pelvic inlet; in LOA, sagittal suture in right oblique diameter |
| 2 | Descent | Continuous throughout labour |
| 3 | Flexion | Chin onto chest; reduces presenting diameter from occipitofrontal (11 cm) to suboccipitobregmatic (9.5 cm) |
| 4 | Internal rotation | Occiput rotates anteriorly to lie under symphysis pubis; sagittal suture in AP diameter at outlet |
| 5 | Extension | Head extends around symphysis pubis; occiput, bregma, face, chin delivered in sequence |
| 6 | Restitution | Head turns back 45° to align with fetal shoulders (LOA → occiput to left) |
| 7 | External rotation | Further 45° turn as shoulders rotate internally; shoulders now in AP diameter |
Then lateral flexion delivers anterior then posterior shoulder, followed by rest of body.
Partograph (WHO)
Used to monitor progress of labour graphically.
Components:
- Fetal heart rate (FHR) - every 30 min
- Membranes and liquor
- Moulding
- Cervical dilatation plotted against time
- Descent of head (in fifths palpable abdominally)
- Uterine contractions (frequency, duration, strength)
- Oxytocin/drugs
- Maternal pulse, BP, temperature
- Urine output
Alert line: Rate of 1 cm/hr dilatation from 4 cm
Action line: 4 hours to the right of alert line
Active Management of Third Stage (AMTSL)
WHO-recommended routine for all deliveries:
- Oxytocin 10 IU IM within 1 minute of delivery (drug of choice)
- Controlled cord traction (CCT) - Brandt-Andrews method
- Uterine massage after placenta delivery (controversial - not routine per recent WHO)
Misoprostol 600 mcg oral/sublingual - used where oxytocin unavailable
Brandt-Andrews method: Suprapubic counter-pressure on lower uterus while traction on cord - prevents uterine inversion.
Monitoring During Normal Labour
Maternal
- BP and pulse every 30 min (active phase) / 1 hour (latent)
- Temperature every 4 hours
- Urine - output, protein, ketones
- State of uterine contractions
Fetal
- FHR - auscultate every 15-30 min in first stage; every 5 min in second stage
- Colour of liquor - clear (normal), meconium-stained (fetal distress)
- Moulding - excessive moulding suggests CPD
Normal FHR: 110-160 bpm
Analgesia in Labour
| Method | Details |
|---|---|
| Inhalational | Entonox (50% O₂ + 50% N₂O) - self-administered |
| Systemic opioids | Pethidine 50-100 mg IM / Morphine - causes neonatal respiratory depression |
| Epidural | Gold standard; bupivacaine ± fentanyl; avoid bearing down reflex impairment |
| Pudendal block | For second stage/instrumental delivery |
| Paracervical block | Rarely used; risk of fetal bradycardia |
Normal Puerperium (Post-Delivery)
- Lochia rubra (red, days 1-4) → lochia serosa (pink/brown, days 4-9) → lochia alba (white, day 10+)
- Uterine involution: Returns to non-pregnant size by 6 weeks
- Afterpains: More common in multiparae; due to uterine contractions
- Breastfeeding: Encouraged immediately; stimulates oxytocin → uterine involution
Key Numbers to Remember
| Parameter | Value |
|---|---|
| Period of viability | 28 weeks / 1000 g |
| Full cervical dilatation | 10 cm |
| Normal FHR | 110-160 bpm |
| 1st stage duration (primi) | ~12 hours |
| 1st stage duration (multi) | ~6 hours |
| 2nd stage duration (primi) | Up to 2 hours |
| 3rd stage duration | Up to 30 minutes |
| Engagement (primi) | 36-38 weeks |
| Oxytocin (AMTSL) | 10 IU IM |
| Suboccipitobregmatic diameter | 9.5 cm |
| Occipitofrontal diameter | 11 cm |
| Biparietal diameter | 9.5 cm |
Note: The uploaded PDF only contains Chapter 20 (Medical & Surgical Illnesses Complicating Pregnancy, pages 246-286). It does not include the Normal Labour chapter. These notes are compiled from DC Dutta's Textbook of Obstetrics (standard content across editions). If you have the correct pages/chapter, share that file and I'll extract notes directly from the text.
Generate a visual flowchart of labour stages and mechanisms
Generating Image
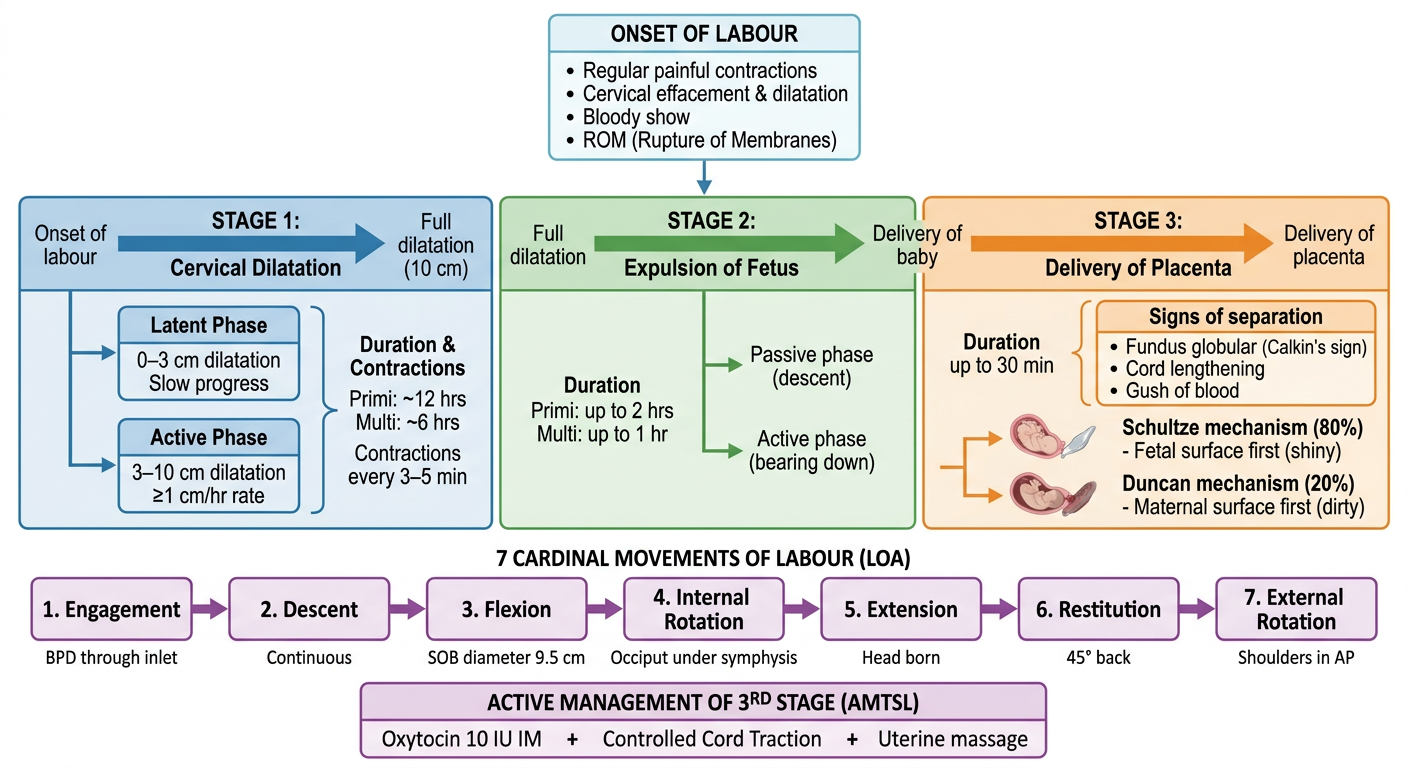
Here's your visual flowchart covering:
- Onset of Labour triggers at the top
- 3 Stages color-coded (blue → green → orange) with durations, key events, and sub-phases
- 7 Cardinal Movements as a sequential horizontal flow with one-line descriptors for each
- AMTSL summary at the bottom
Key highlights shown:
- Latent vs. Active phase distinction in Stage 1
- Schultze (80%) vs. Duncan (20%) placental separation in Stage 3
- SOB diameter (9.5 cm) noted at the Flexion step
Let me know if you'd like a separate detailed diagram for any specific part - for example, the pelvic diameters, the partograph, or fetal head positions during rotation.
This is a shared conversation. Sign in to Orris to start your own chat.