Here are detailed answers to all seven SDL reflection questions on Infections of the Hand and Foot, drawn from textbooks, clinical guidelines (Malaysia and UK), and peer-reviewed literature.
SDL Reflection: Infections of the Hand and Foot
Question 1: What were the learning outcomes for this SDL session?
By the end of this SDL session, students should be able to:
- Classify infections of the hand and foot into spreading (lymphangitis, cellulitis) and localised (paronychia, felon, web space, deep space, suppurative tenosynovitis, necrotizing fasciitis) types.
- Describe the relevant anatomy of fascial spaces of the hand (thenar, midpalmar, hypothenar), flexor tendon sheaths (radial and ulnar bursae), and the pulp space of the finger, explaining how these anatomical boundaries influence the spread and containment of infection.
- Identify the clinical features of each type of infection, including the Kanavel signs of suppurative flexor tenosynovitis.
- List appropriate investigations including FBC, CRP, blood cultures, wound swabs, plain X-ray, and MRI.
- Outline basic management - both non-surgical (antibiotics, elevation, splinting) and surgical (incision and drainage, debridement, tendon sheath irrigation).
- Recognise diabetic foot infection as a limb- and life-threatening emergency requiring multidisciplinary care, in line with the Malaysia CPG on Management of Diabetic Foot (2nd Edition, 2018) and IWGDF/IDSA 2023 Guidelines.
- Identify red flags for necrotizing fasciitis and understand the LRINEC score as a risk-stratification tool.
Question 2: What did you already know about this topic before the session?
(Student self-reflection - examples of likely prior knowledge)
- Basic knowledge that cellulitis is a bacterial skin infection causing redness, warmth, and swelling.
- Awareness that diabetic patients are at higher risk of foot infections due to neuropathy and poor circulation.
- General understanding that abscesses require incision and drainage.
- Familiarity with common pathogens such as Staphylococcus aureus and Streptococcus species.
- Knowledge that antibiotics (e.g., flucloxacillin) are used to treat bacterial skin infections.
- Some awareness that hand injuries can become infected, especially after puncture wounds.
Question 3: What new knowledge or skills did you gain today?
A. Clinical Features by Infection Type
1. Lymphangitis
Organisms enter through minor abrasions, often forgotten by the patient. The hand becomes swollen and painful with high fever and constitutional disturbance. Red streaks along lymphatic channels are visible in fair-skinned individuals. Regional lymphadenopathy follows - the axillary nodes enlarge for lateral hand infections; the supratrochlear nodes enlarge for medial hand infections.
- S Das, Manual on Clinical Surgery, 13th ed.
2. Cellulitis
A diffuse spreading infection of the dermis and subcutaneous tissue. Clinically: erythema, warmth, swelling, and tenderness. In the foot, it commonly arises near the toes in the context of athlete's foot (tinea pedis). Most cases are caused by Group A Streptococcus or Staphylococcus aureus.
- NICE NG141, Cellulitis and Erysipelas Antimicrobial Prescribing Guidelines (2019)
3. Paronychia (Acute)
Infection beneath the eponychium (nail fold), caused by careless nail paring or contaminated manicure instruments. Pus may burrow beneath the nail base. Presents with excruciating pain and redness of the nail fold. In severe cases, subungual extension of pus can occur.
Chronic paronychia differs: affects women who do frequent washing; insidious onset; glazed, pink (not angry red) eponychium; nail becomes cross-ridged and pigmented; often multiple fingers.
- S Das, Manual on Clinical Surgery, 13th ed.
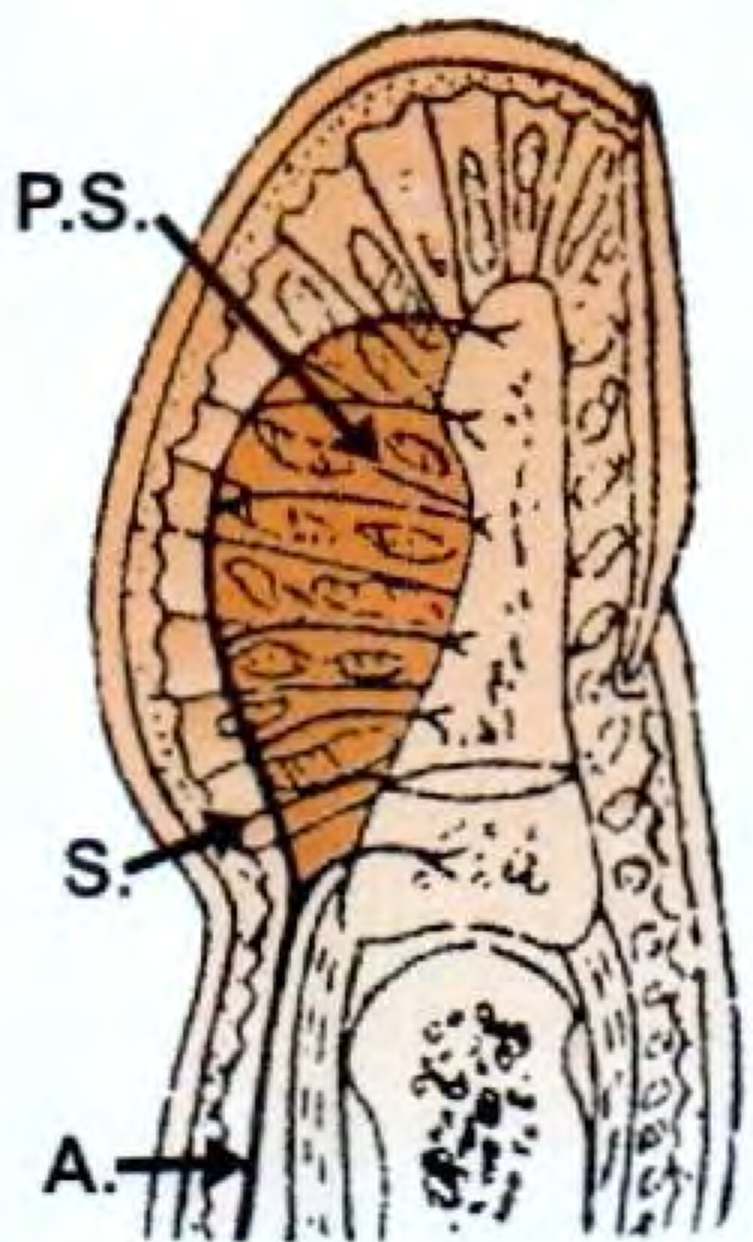
4. Felon (Pulp Space Infection)
A subcutaneous infection of the terminal finger pulp. The pulp space is divided into 15-20 compartments by fibrous septa running from the periosteum of the distal phalanx to the dermis. A transverse septum anchors the space proximally at the epiphyseal line.
Clinical features: Starts with increasing, throbbing pain; maximum swelling at the centre where the abscess develops.
Anatomical significance: The closed compartment architecture raises the tissue pressure dramatically, compressing blood vessels and causing necrosis of the distal 4/5ths of the distal phalanx. Only the epiphysis (supplied by a vessel arising below the septum) remains viable.
Complications: (i) Osteomyelitis of the terminal phalanx; (ii) Pyogenic arthritis of the DIP joint; (iii) Spread to the flexor tendon sheath if incision is wrongly extended proximally.
- Gray's Anatomy for Students, 4th ed.; S Das, Manual on Clinical Surgery
5. Suppurative Flexor Tenosynovitis (Intrathecal Whitlow)
Infection of the flexor tendon sheath, usually from a direct puncture wound through a digital flexion crease (where skin is closest to the sheath). Can also arise from spread from adjacent pulp space infection.
Kanavel's Four Cardinal Signs (Miller's Review of Orthopaedics, 9th ed.):
- Flexed resting posture of the digit
- Fusiform (uniform) swelling of the entire digit
- Tenderness along the flexor tendon sheath
- Pain on passive extension of the digit
Tenderness over the flexor sheath is considered the most significant sign.
Causative organisms: S. aureus (penetrating injury), Streptococcus, Eikenella corrodens (human bites), Pasteurella multocida (animal bites).
Complications: Necrosis of the tendon and permanent stiffness in flexion; spread to the palm (the little finger sheath communicates with the ulnar bursa; the thumb sheath communicates with the radial bursa, creating the "horseshoe abscess" when both communicate).
- Campbell's Operative Orthopaedics, 15th ed. 2026; S Das, 13th ed.
6. Deep Space Infections of the Palm
The palm contains three main fascial spaces:
| Space | Boundaries | Contents |
|---|
| Thenar space | Lateral - first metacarpal; Medial - oblique head of adductor pollicis | Index finger flexor tendons |
| Midpalmar space | Anterior - synovial sheaths of digits 3-5; Posterior - dorsal interossei; Lateral - lateral fibrous septum; Medial - 5th metacarpal | Communicates with forearm via carpal tunnel |
| Hypothenar space | Between hypothenar muscles and 5th metacarpal | Little finger structures |
The midpalmar space is the most clinically important - infection here causes loss of the normal palmar concavity and swelling on both palmar and dorsal surfaces (dorsal oedema via lymphatic tracking).
- Gray's Anatomy for Students, 4th ed.
7. Web Space Infection (Collar-Stud Abscess)
Loose fat in the web space allows pus to collect. A "collar-stud abscess" forms when an intracutaneous abscess communicates with a deeper subcutaneous abscess through a small hole. Characteristic sign: separation of adjacent fingers due to web space swelling. Pus points on the dorsum (thinner skin).
- S Das, Manual on Clinical Surgery, 13th ed.
8. Necrotizing Fasciitis
A rapidly progressive, life-threatening infection of the fascia and subcutaneous tissue. Most commonly caused by Group A beta-haemolytic Streptococcus (S. pyogenes), though polymicrobial (Type I) and monomicrobial (Type II) forms exist. Risk groups: immunocompromised, IV drug users, diabetes, alcohol use disorder.
Clinical features: Disproportionate pain (greater than the clinical appearance suggests), skin necrosis, bullae, crepitus, rapid systemic deterioration (fever, hypotension, shock).
- Harrison's Principles of Internal Medicine, 22nd ed.; Miller's Review of Orthopaedics, 9th ed.
LRINEC Score (Laboratory Risk Indicator for Necrotizing Fasciitis) - from Wong et al., 2004:
| Parameter | Score |
|---|
| CRP ≥150 mg/L | 4 |
| WBC 15-25 × 10³/mm³ | 1; >25 = 2 |
| Haemoglobin <11 g/dL | 2 |
| Sodium <135 mmol/L | 2 |
| Creatinine >141 µmol/L | 2 |
| Glucose >10 mmol/L | 1 |
Score: ≤5 = low risk; 6-7 = intermediate; ≥8 = high risk
- Fischer's Mastery of Surgery, 8th ed.; Campbell's Operative Orthopaedics, 15th ed.
9. Diabetic Foot Infection
A major cause of hospital admission worldwide. Caused by the combined effects of:
- Peripheral neuropathy (loss of protective sensation)
- Peripheral arterial disease (impaired tissue oxygenation)
- Immune defects (impaired neutrophil function)
- Autonomic neuropathy (dry skin, fissures, Charcot foot)
Pathogens: S. aureus, beta-haemolytic streptococci, aerobic Gram-negative bacilli, Pseudomonas (over-represented), and anaerobes.
Severity classification (PEDIS/IWGDF):
- Grade 1: No infection
- Grade 2: Mild (superficial, cellulitis <2 cm)
- Grade 3: Moderate (deeper tissues, >2 cm cellulitis, or lymphangitis)
- Grade 4: Severe (systemic inflammatory response syndrome)
Complications: Osteomyelitis (detected by "probe-to-bone" test), Charcot neuroarthropathy, amputation (in up to 20% of ulcerated cases).
- Bailey & Love's Short Practice of Surgery, 28th ed.
B. Relevant Anatomy
- The midpalmar space communicates with the anterior forearm via the carpal tunnel, explaining how untreated palmar infections can spread to the forearm.
- The felon is anatomically confined by fibrous septa tethering the dermis to the distal phalanx - infections cannot spread dorsally or proximally unless the fascial architecture is disrupted.
- The flexor tendon sheaths of the little finger and thumb communicate with the ulnar and radial bursae respectively, which themselves may communicate at the wrist, creating the "horseshoe abscess" pattern.
- Gray's Anatomy for Students, 4th ed.
C. Investigations
| Investigation | Rationale |
|---|
| FBC | Leukocytosis in bacterial infection; anaemia in severe/chronic infection |
| CRP / ESR / Procalcitonin | Markers of systemic inflammation; used in LRINEC score; relevant for diagnosing DFI (IWGDF 2023) |
| Blood cultures | Positive in bacteraemia/sepsis |
| Wound swab / tissue biopsy | Culture and sensitivity - tissue biopsy preferred over swab for deep infections (IWGDF 2023 Recommendation 5) |
| Plain X-ray | Detect gas in soft tissues (necrotizing fasciitis), osteomyelitis, foreign body |
| MRI | Most sensitive for osteomyelitis in diabetic foot; delineates soft tissue involvement |
| Ultrasound | Fluid in tendon sheath, joint effusion; increased Doppler flow in tenosynovitis (Grainger & Allison's Diagnostic Radiology) |
| Probe-to-bone test | Positive result + elevated CRP + abnormal X-ray = confirmed osteomyelitis in DFI |
- Bailey & Love's, 28th ed.; IWGDF/IDSA Guidelines 2023
Question 4: What resources did you use to learn?
Textbooks
- Gray's Anatomy for Students, 4th ed. (Elsevier) - Anatomy of palmar fascial spaces and felon
- S Das, A Manual on Clinical Surgery, 13th ed. - Comprehensive classification and clinical details of hand infections
- Bailey & Love's Short Practice of Surgery, 28th ed. - Diabetic foot infection; surgical management
- Miller's Review of Orthopaedics, 9th ed. - Kanavel signs; hand infection summary
- Campbell's Operative Orthopaedics, 15th ed. (2026) - Tenosynovitis; necrotizing fasciitis; LRINEC score
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Necrotizing fasciitis; streptococcal infections
- Fischer's Mastery of Surgery, 8th ed. - LRINEC score; cellulitis management
Clinical Guidelines
- Malaysia CPG: Management of Diabetic Foot, 2nd Edition (Ministry of Health Malaysia, 2018) - Diabetic foot ulcer classification; antibiotics; surgery
- IWGDF/IDSA Guidelines on the Diagnosis and Treatment of Diabetes-related Foot Infections (2023) - Gold standard international guidelines, endorsed for use in Malaysia
- NICE NG141: Cellulitis and Erysipelas - Antimicrobial Prescribing (UK, 2019) - Evidence-based antibiotic recommendations
Academic Websites
- NICE Guidance (ng141) - UK cellulitis antimicrobial prescribing
- IWGDF Guidelines 2023 - International diabetic foot infection guidelines
- IDSA Practice Guidelines - Diabetic Foot
- NHS UK (cellulitis page) - Patient-accessible clinical information
Question 5: How did your group work together to learn?
(This question is for student self-reflection, but here is a model framework)
- Role distribution: Each group member took a specific infection type (e.g., one covered superficial infections - paronychia/felon; another covered deep hand infections and tenosynovitis; one covered foot infections including diabetic foot and cellulitis).
- Communication: Groups used shared documents or whiteboards to compile a master table of infections with their pathology, features, and management.
- Anatomy integration: One member focused on anatomical spaces and their boundaries, explaining to the group how they dictate the spread of infection.
- Guideline synthesis: One member compared the Malaysia CPG and IWGDF guidelines to highlight differences/priorities for the local context.
- Challenges: Distinguishing clinical features of closely related conditions (e.g., felon vs. volar space infection vs. suppurative tenosynovitis) required careful comparison and discussion.
Question 6: What key clinical take-home messages did you learn?
1. Anatomy determines the spread and severity of hand infections
The unique compartmentalisation of the hand (fascial spaces, tendon sheaths) means that infections do not spread freely but follow predictable anatomical pathways. A midpalmar infection can track to the forearm via the carpal tunnel if untreated. A felon is confined by fibrous septa but raises tissue pressure enough to cause avascular necrosis of bone. Understanding the anatomy predicts the clinical presentation and guides surgical drainage.
- Gray's Anatomy for Students, 4th ed.
2. Kanavel's four signs are the clinical hallmark of suppurative flexor tenosynovitis - early diagnosis and treatment prevent catastrophic loss of function
All four signs (flexed posture, fusiform swelling, tenderness over the sheath, pain on passive extension) must be actively sought. If fewer than four signs are present and symptoms have been present < 48 hours, a trial of IV antibiotics and splinting is appropriate. If all four signs are present, or symptoms exceed 48 hours, immediate surgical drainage is required. Delayed treatment leads to tendon necrosis, adhesion, permanent stiffness, and possible amputation.
- Campbell's Operative Orthopaedics, 15th ed.; Miller's Review of Orthopaedics, 9th ed.; [PMID: 35081807]
3. Necrotizing fasciitis is a surgical emergency - time to debridement saves lives
Survival is approximately 90% if debridement is performed within 24 hours, falling to 75% at 48 hours. Do not delay surgery to obtain imaging when clinical suspicion is high. The LRINEC score (≥6 = intermediate risk, ≥8 = high risk) can help stratify but must not replace clinical judgment. Treatment requires: aggressive surgical debridement of all necrotic tissue, broad-spectrum IV antibiotics (including penicillin + clindamycin for GAS - clindamycin inhibits toxin production via protein synthesis inhibition), and ICU-level supportive care.
- Harrison's Principles, 22nd ed.; Campbell's Operative Orthopaedics, 15th ed.
4. (Bonus) Diabetic foot infection requires a multidisciplinary approach: classify severity, investigate for osteomyelitis, and escalate antibiotic cover for Pseudomonas and anaerobes
The probe-to-bone test, combined with elevated inflammatory markers and abnormal plain X-ray, confirms osteomyelitis. MRI is the most sensitive imaging modality. Empiric therapy for severe DFI should cover Pseudomonas and anaerobes (e.g., piperacillin-tazobactam ± metronidazole). Early surgery (within 24-48 hours) is recommended for moderate-severe infections (IWGDF 2023).
- Bailey & Love's, 28th ed.; Malaysia CPG Diabetic Foot 2018; IWGDF/IDSA 2023
Question 7: What do you plan to improve in your future SDL learning approach?
(Model self-reflection points)
-
Critical appraisal skills: I will practice appraising the quality and relevance of different sources - recognising that international guidelines (IWGDF 2023) may need to be contextualised for the Malaysian healthcare setting (e.g., MRSA prevalence, antibiotic availability, local antibiograms).
-
Integration of anatomy with pathology: I tended to study anatomy and clinical medicine separately. In future sessions, I will actively link anatomical knowledge to clinical features (e.g., "why does a midpalmar infection cause dorsal swelling?").
-
Time management: I will allocate time at the start to clarify learning objectives before reading widely, ensuring I address all learning outcomes within the session.
-
Deeper reading on investigations: I focused mainly on clinical features but was less confident on investigations. I will practice constructing investigation plans for each infection type and understanding the diagnostic utility (sensitivity/specificity) of each test.
-
Using clinical guidelines proactively: I will access the Malaysia CPG and NICE guidelines at the beginning of each SDL topic, rather than relying solely on textbooks, to understand current evidence-based practice standards.
Summary Table: Key Hand and Foot Infections
| Infection | Location | Key Features | Organism | Management |
|---|
| Paronychia | Nail fold | Red, swollen, painful nail fold | S. aureus, Candida (chronic) | Drainage; antibiotics |
| Felon | Finger pulp | Throbbing pain; risk of osteomyelitis | S. aureus | I&D (not extending proximally to sheath) |
| Suppurative tenosynovitis | Flexor sheath | Kanavel's 4 signs | S. aureus, Streptococcus | IV antibiotics ± sheath irrigation/drainage |
| Midpalmar space | Deep palm | Loss of palmar concavity; dorsal oedema | Mixed | I&D + IV antibiotics |
| Web space | Digital web | Collar-stud abscess; finger separation | S. aureus | I&D |
| Cellulitis | Dermis/subcutis | Erythema, warmth, swelling | Streptococcus, S. aureus | Flucloxacillin PO (mild) or IV (severe) |
| Necrotizing fasciitis | Fascia/subcutis | Rapid progression; disproportionate pain; crepitus | GAS, polymicrobial | EMERGENCY: surgical debridement + broad-spectrum IV antibiotics |
| Diabetic foot | Foot ulcer ± deep | Neuropathy, ischaemia, osteomyelitis | S. aureus, GNB, anaerobes, Pseudomonas | Multidisciplinary; debridement; IV antibiotics; offloading |
Key References
- S Das, A Manual on Clinical Surgery, 13th Edition
- Gray's Anatomy for Students, 4th Edition (Elsevier)
- Bailey & Love's Short Practice of Surgery, 28th Edition
- Miller's Review of Orthopaedics, 9th Edition
- Campbell's Operative Orthopaedics, 15th Edition (2026)
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- Fischer's Mastery of Surgery, 8th Edition
- Malaysia CPG: Management of Diabetic Foot, 2nd Ed. (MOH Malaysia, 2018)
- IWGDF/IDSA Guidelines on Diabetic Foot Infections, 2023
- NICE NG141: Cellulitis and Erysipelas, 2019
- Latario et al. (2023). Antibiotics Versus Surgery in Treatment of Early Flexor Tenosynovitis. Hand (NY). [PMID: 35081807]