Briefly discuss salient pelvic floor muscles and nerves with respect to ano-rectum and measures taken to prevent their injury during low anterior resection for carcinoma rectum. (Bailey 28th edn: chap. 80 Pg no: 1417)
Pelvic Floor Muscles and Nerves in Relation to the Ano-rectum, and Their Preservation during Low Anterior Resection
Part I: Salient Pelvic Floor Muscles
1. Levator Ani Complex
| Component | Origin | Insertion / Course | Function |
|---|---|---|---|
| Puborectalis | Posterior surface of pubis | Passes posteriorly around the anorectal junction as a U-shaped sling | Creates and maintains the anorectal angle (~120°); its sustained contraction is the principal mechanism of faecal continence |
| Pubococcygeus | Pubis | Coccyx and anococcygeal raphe | Elevates the pelvic floor; supports the rectum |
| Iliococcygeus | Ischial spine and arcus tendineus | Coccyx and anococcygeal raphe | Closes the pelvic outlet |
2. External Anal Sphincter (EAS)
3. Internal Anal Sphincter (IAS)
4. Obturator Internus
Part II: Salient Pelvic Nerves
A. Sympathetic Innervation
- Formed by convergence of the right and left lumbar sympathetic trunks and the aortic plexus, at the level of the aortic bifurcation and anterior to the sacral promontory (L5/S1)
- Divides into the right and left hypogastric nerves which descend into the pelvis along either side of the rectum (posterior to its fascia)
- Injury here causes loss of ejaculation (failure of seminal emission) in males and altered bladder neck function
- Descend from the superior hypogastric plexus along the posterolateral aspects of the rectum
- Lie on the posterior surface of the mesorectum - at risk during posterior rectal mobilisation if dissection strays into an incorrect plane
- Join the pelvic plexuses laterally
B. Parasympathetic Innervation
- Arise from S2, S3, and S4 sacral nerve roots
- Exit the sacral foramina and travel anterolaterally to join the pelvic (inferior hypogastric) plexus
- They are the erection nerves - injury causes erectile dysfunction in males
C. The Pelvic (Inferior Hypogastric) Plexus
- A paired autonomic plexus located on the lateral pelvic sidewall, at the level of the lateral stalks/lateral ligaments of the rectum
- Receives both sympathetic (from hypogastric nerves) and parasympathetic (from nervi erigentes) inputs
- Sends branches to bladder, prostate/seminal vesicles, urethra, uterus/vagina, and rectum
- Contains the neurovascular bundle of Walsh (the cavernous nerves) which run alongside Denonvilliers' fascia anterolaterally
- Injury leads to bladder dysfunction (retention or incontinence) and sexual dysfunction
D. Pudendal Nerve (S2, S3, S4)
- Exits the pelvis through the greater sciatic foramen, wraps around the ischial spine, and re-enters through the lesser sciatic foramen into Alcock's canal
- Gives the inferior rectal nerve (to external anal sphincter and perianal skin), perineal nerve, and dorsal nerve of the penis/clitoris
- Injury causes faecal incontinence, urinary incontinence, and impaired perineal sensation
Part III: Measures to Prevent Nerve Injury during Low Anterior Resection (LAR)
1. High Ligation of the Inferior Mesenteric Artery - Identifying the Superior Hypogastric Plexus
- During sigmoid/left colon mobilisation, the superior hypogastric plexus lies just inferior to the aortic bifurcation and the sacral promontory, slightly to the left of the midline
- The IMA is ligated below the left colic artery origin where possible, or just at its origin from the aorta
- Dissection is kept in the correct retroperitoneal plane to avoid sweeping the plexus anteriorly; the plexus should be left adherent to the posterior presacral fascia
2. TME in the "Holy Plane" - Preserving Hypogastric Nerves
- Posterior rectal dissection is performed in the avascular plane between the mesorectal fascia (visceral layer) and the presacral fascia (parietal layer)
- This plane passes anterior to the hypogastric nerves, keeping them against the presacral fascia/sacrum
- Waldeyer's recto-sacral fascia is divided at the level of S4 as the dissection reaches the pelvic floor, taking care to remain anterior to the sacral fascia
- Sharp dissection rather than blunt avulsion prevents nerve traction injury
3. Lateral Dissection - Sparing the Pelvic Plexus
- The lateral ligaments (which contain the middle rectal artery and part of the pelvic plexus) are divided close to the rectal wall to minimise plexus injury
- The neurovascular bundles course on the lateral surface of the mesorectal fascia; the dissection stays medial to them
- Avoiding excessive traction or diathermy near the lateral stalks is important
4. Anterior Dissection - Preserving Nerves of Denonvilliers
- Anteriorly, the dissection enters the plane between the anterior mesorectal fascia and Denonvilliers' fascia (for posterior tumours) or between Denonvilliers' fascia and the prostate/seminal vesicles (for anterior tumours)
- The cavernous nerves (from pelvic plexus) run posterolaterally to the prostate in the neurovascular bundle - staying in the correct plane of Denonvilliers' fascia prevents erectile nerve injury
- In females, the rectovaginal septum is entered with care to protect the pelvic plexus branches coursing along the vaginal wall
5. Avoiding Excessive Lateral Traction
- Medialisation of the rectum with excessive tension can stretch and avulse the pelvic plexuses and nervi erigentes - gentle retraction is essential
6. Nerve Stimulation (Intraoperative Neuromonitoring)
- Intraoperative nerve stimulation with recording of bladder/urethral sphincter responses can help identify the pelvic plexus and nervi erigentes, especially in difficult re-operative or post-radiotherapy cases
7. Correct Patient Positioning and Lighting
- The steep Trendelenburg position and adequate lighting/laparoscopic magnification (particularly with robotic/laparoscopic approaches) enhance visualisation of the nerve structures; robotic surgery may reduce nerve injury by virtue of improved pelvic visibility
8. Avoiding Diathermy Near Nerves
- The nervi erigentes are at greatest risk near the sacral foramina; diathermy or clips here can cause thermal injury even when the anatomical plane seems correct
Summary
| Structure at Risk | Surgical Step at Risk | Consequence of Injury |
|---|---|---|
| Superior hypogastric plexus | High IMA ligation / sacral promontory dissection | Ejaculatory failure, bladder dysfunction |
| Hypogastric nerves | Posterior rectal mobilisation | Ejaculatory failure |
| Nervi erigentes (S2-S4) | Lateral rectal dissection at sacrum | Erectile dysfunction, bladder dysfunction |
| Pelvic (inferior hypogastric) plexus | Lateral ligament division | Mixed bladder + sexual dysfunction |
| Pudendal nerve | Deep pelvic floor dissection, Alcock's canal | Faecal/urinary incontinence, perineal anaesthesia |
| Neurovascular bundle (cavernous) | Anterior dissection at Denonvilliers' | Erectile dysfunction |
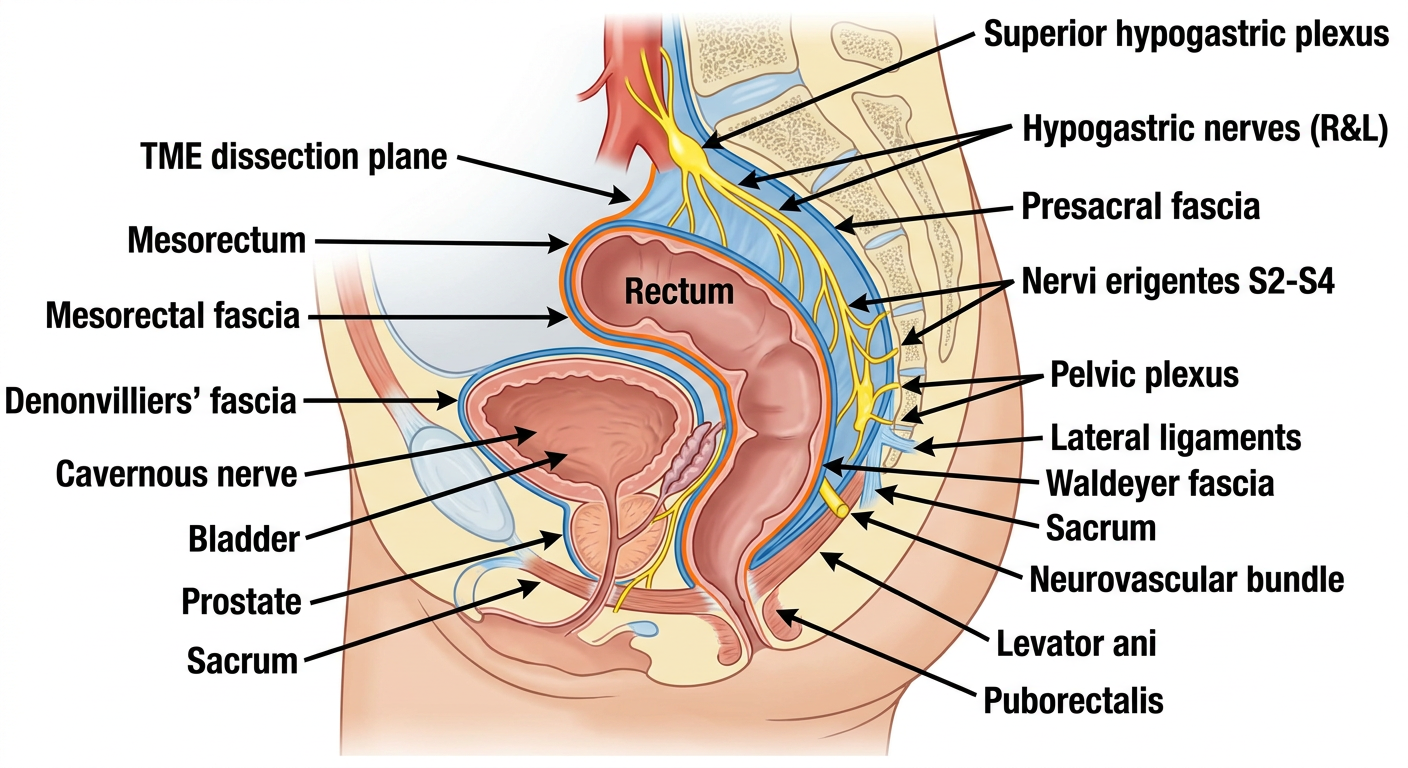
Create a visual diagram showing the nerve preservation planes in TME and LAR
Detailed anatomical surgical diagram showing nerve preservation planes in Total Mesorectal Excision (TME) and Low Anterior Resection (LAR) for rectal cancer. Sagittal cross-section view of the male pelvis showing: 1. POSTERIOR plane: The "Holy Plane" between mesorectal fascia (visceral) and presacral fascia (parietal), with hypogastric nerves labeled running posterior to the mesorectum along the sacrum. Waldeyer's recto-sacral fascia labeled at S4 level. 2. LATERAL plane: Pelvic (inferior hypogastric) plexus on lateral pelvic sidewall, nervi erigentes (S2, S3, S4 pelvic splanchnic nerves) coming from sacral foramina, lateral ligaments/stalks labeled, neurovascular bundle labeled. 3. ANTERIOR plane: Denonvilliers' fascia between anterior mesorectum and prostate/seminal vesicles, cavernous nerves (neurovascular bundle of Walsh) running posterolateral to prostate. 4. Superior: Superior hypogastric plexus (presacral nerve) at aortic bifurcation/L5-S1, splitting into right and left hypogastric nerves. 5. Rectum and mesorectum in center with mesorectal fascia envelope clearly shown. 6. TME dissection plane highlighted as a colored boundary line around the entire mesorectum. 7. Color coding: Red for arteries, yellow for nerves, blue for fascia planes, orange for dissection plane. 8. Clear anatomical labels for: Rectum, Mesorectum, Mesorectal fascia, Presacral fascia, Superior hypogastric plexus, Hypogastric nerves (R&L), Nervi erigentes S2-S4, Pelvic plexus, Denonvilliers fascia, Waldeyer fascia, Neurovascular bundle, Bladder, Prostate, Sacrum, Levator ani, Puborectalis. Style: Clean medical illustration, white background, anatomically accurate, surgical textbook quality with bold labels and arrows.