Differnet between cirumciliary conjection and afornical conjection
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I have enough information to give a thorough answer from the textbook findings combined with my ophthalmology knowledge. The textbook from Family Medicine clearly describes circumciliary (ciliary) injection vs conjunctival congestion. Let me now provide a comprehensive answer.
Circumciliary Congestion vs Fornical (Conjunctival) Congestion
These are two distinct patterns of red eye that point to very different underlying pathologies. Differentiating them is one of the most important clinical skills in ophthalmology.
1. Circumciliary Congestion (Ciliary Injection / Perilimbal Flush)
Also called ciliary injection or pericorneal flush.
| Feature | Details |
|---|---|
| Location | Ring of redness around the limbus (corneoscleral junction), maximum at the corneal margin |
| Distribution | Pericorneal - deepest near the cornea, fades toward the fornices |
| Vessels involved | Deep anterior ciliary vessels (branches of anterior ciliary arteries supplying iris, ciliary body, cornea) |
| Color | Violaceous/brick-red - deeper, darker hue |
| Individual vessels | Vessels not individually distinguishable - appear as a diffuse flush |
| Movement with conjunctiva | Vessels do NOT move when conjunctiva is displaced - they are deep |
| Response to topical adrenaline | Does NOT blanch significantly (deep vessels) |
| Response to phenylephrine 2.5% | Minimal or no blanching |
| Clinical significance | Serious - indicates intraocular disease |
| Causes | Iritis/uveitis, acute angle-closure glaucoma, corneal ulcer, keratitis, endophthalmitis, scleritis |
As noted in the Textbook of Family Medicine: "ciliary infection appears as a red ring surrounding the cornea in which individual vessels are not clearly visible. The significance of ciliary infection is that the deep ciliary vessels are involved, indicating a much more serious inflammatory condition of the eye, such as a deep corneal infection, iritis, or iridocyclitis."
2. Fornical (Conjunctival) Congestion
Also called conjunctival injection or superficial congestion.
| Feature | Details |
|---|---|
| Location | Maximum in the fornices (peripheral, away from the limbus), fades toward the cornea |
| Distribution | Diffuse over the bulbar and palpebral conjunctiva - more prominent peripherally |
| Vessels involved | Superficial posterior conjunctival vessels |
| Color | Bright red |
| Individual vessels | Vessels individually visible, branching from fornix toward limbus |
| Movement with conjunctiva | Vessels move when conjunctiva is shifted (they are superficial, within the conjunctiva) |
| Response to topical adrenaline | Blanches readily (superficial vessels respond to vasoconstrictors) |
| Response to phenylephrine 2.5% | Blanches completely |
| Clinical significance | Usually indicates surface/external eye disease |
| Causes | Conjunctivitis (bacterial, viral, allergic), subconjunctival hemorrhage, dry eye, foreign body, chemical irritation |
Quick Comparison Table
| Feature | Circumciliary Congestion | Fornical/Conjunctival Congestion |
|---|---|---|
| Maximum redness | Around the cornea (limbus) | In the fornices (periphery) |
| Vessels | Deep, not individually visible | Superficial, individually visible |
| Color | Violaceous/deep red | Bright scarlet red |
| Conjunctival movement | Vessels stay fixed | Vessels move with conjunctiva |
| Topical vasoconstrictors | Does NOT blanch | Blanches readily |
| Associated symptoms | Pain, photophobia, visual blurring | Discharge, grittiness, itching |
| Diseases | Uveitis, glaucoma, keratitis, scleritis | Conjunctivitis, allergic reaction |
| Urgency | HIGH - refer to ophthalmologist | Usually can be managed in primary care |
Clinical Pearl
The key diagnostic point: if a patient has redness maximum around the cornea with pain, photophobia, and visual change - think circumciliary injection and intraocular pathology. If redness is maximum in the fornices with discharge and no visual change - think simple conjunctivitis (fornical/conjunctival congestion).
The rule is simple: fornical = benign, circumciliary = dangerous.
- Textbook of Family Medicine, 9e - Red Eye chapter
Sign of bells palsy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete overview of the signs of Bell's palsy, drawn from Harrison's, Adams & Victor's Neurology, and Rosen's Emergency Medicine.
Signs of Bell's Palsy
Bell's palsy is an idiopathic lower motor neuron (LMN) paralysis of the facial nerve (CN VII), most likely caused by HSV-1 reactivation in the geniculate ganglion.
Key Clinical Signs
1. Motor Signs (CN VII - All Branches Involved)
Since it is a peripheral (LMN) lesion, ALL branches of CN VII on the affected side are involved - this is the single most important differentiating feature from central (UMN) lesions.
| Sign | Description |
|---|---|
| Forehead paralysis | Patient cannot wrinkle the forehead or raise the eyebrow on the affected side - HALLMARK of LMN lesion |
| Lagophthalmos | Inability to close the eye completely on the affected side |
| Bell's phenomenon | When the patient tries to close the eye, the eyeball reflexively rolls upward - the white sclera becomes visible. This is a protective reflex |
| Epiphora | Overflow of tears on the cheek due to loss of orbicularis tone and disrupted lacrimal pump |
| Drooping of mouth | Angle of mouth droops; patient cannot smile, show teeth, or puff cheeks on the affected side |
| Loss of nasolabial fold | The nasolabial fold becomes flattened or absent on the affected side |
| Platysma sign | Inability to contract the platysma on the affected side |
| Crocodile tears (later) | Aberrant regeneration may cause tearing during eating (gustatory lacrimation) |
Critical rule: Both upper AND lower facial muscles must be involved to diagnose Bell's palsy. If only lower face is affected, suspect a central (stroke) lesion.
2. Sensory / Special Sense Signs
| Sign | Description |
|---|---|
| Loss of taste (ageusia) | Over the anterior 2/3 of the tongue on the ipsilateral side - due to involvement of the chorda tympani branch. Indicates the lesion is proximal to where chorda tympani joins CN VII |
| Hyperacusis | Abnormal sensitivity to loud sounds on the affected side - due to paralysis of the stapedius muscle (branch from CN VII). Indicates lesion proximal to the nerve to stapedius |
| Pain behind the ear | Periauricular/retroauricular pain (mastoid region) - may precede the paralysis by 1-2 days |
| Facial numbness/paresthesia | Patient may report subjective "fullness" or numbness, though true sensory loss is rare (some overlap from trigeminal nerve branches) |
3. Autonomic Signs
| Sign | Description |
|---|---|
| Decreased tearing (early) | Reduced lacrimation on the affected side if the lesion is proximal to the greater petrosal nerve (which carries parasympathetics to the lacrimal gland) |
| Decreased salivation | Loss of submandibular and sublingual gland secretion (chorda tympani involvement) |
Topographic Localization of Lesion by Signs
| Signs Present | Level of Lesion |
|---|---|
| Facial paralysis + hyperacusis + taste loss + decreased lacrimation | Above geniculate ganglion |
| Facial paralysis + hyperacusis + taste loss (no lacrimation problem) | Between geniculate ganglion and nerve to stapedius |
| Facial paralysis + taste loss (no hyperacusis) | Below stapedius, above chorda tympani |
| Facial paralysis only | Below chorda tympani (near stylomastoid foramen) |
Bell's Palsy vs Central (UMN) Facial Palsy
| Feature | Bell's Palsy (LMN) | Central (UMN) |
|---|---|---|
| Forehead | Paralyzed | Spared (bilateral cortical input) |
| Eye closure | Impaired | Preserved |
| Lower face | Weak | Weak |
| Taste/hyperacusis | May be present | Absent |
| Other CNS signs | Absent | Often present (arm/leg weakness) |
MRI Findings
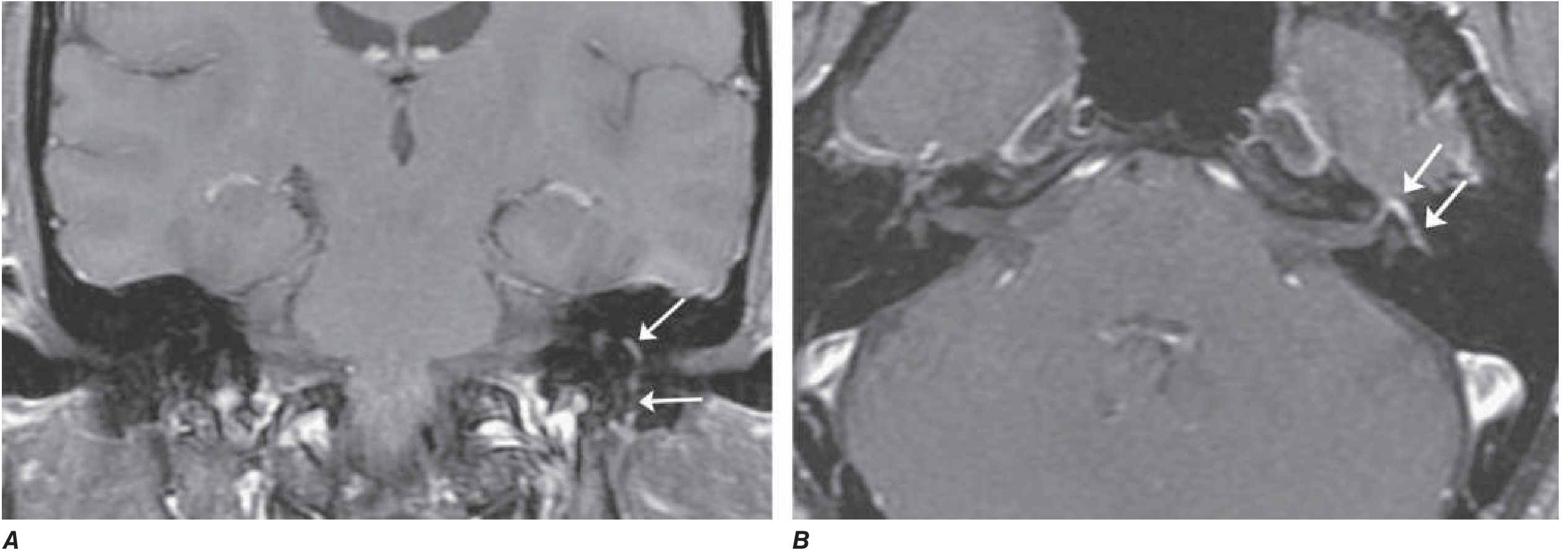
Gadolinium-enhanced MRI showing smooth linear enhancement of the facial nerve in the temporal bone - as seen in Bell's palsy. (Note: similar enhancement can occur in Lyme disease, sarcoidosis, and malignant spread.)
Prognosis Signs
- Favorable: Incomplete paralysis in the first week; early return of taste
- Unfavorable: Complete paralysis with EMG showing denervation after 10 days - indicates axonal degeneration and delayed recovery (3+ months)
- ~80% of patients recover within weeks to months - Harrison's Principles of Internal Medicine, 22e
- Adams and Victor's Principles of Neurology, 12th Ed
- Harrison's Principles of Internal Medicine, 22e
- Rosen's Emergency Medicine, Clinical Features
This is a shared conversation. Sign in to Orris to start your own chat.