Systemic lupus erytamatous notes pathology by robbins mbbs notes by mbbs pathology in flow chart and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content and images needed. Let me compile the comprehensive MBBS pathology notes on SLE from Robbins.
🔬 Systemic Lupus Erythematosus (SLE) - Pathology Notes
Based on Robbins & Cotran Pathologic Basis of Disease + Robbins & Kumar Basic Pathology
📌 DEFINITION
SLE is a chronic, relapsing-remitting, multisystem autoimmune disease characterized by:
- Production of autoantibodies (especially antinuclear antibodies - ANAs)
- Injury caused by immune complex deposition and antibody binding to cells and tissues
- Involvement of skin, joints, kidneys, serosal membranes, and virtually any organ
📊 EPIDEMIOLOGY - Quick Flow
Prevalence: ~1 in 2500 (up to 400/100,000 in some populations)
↓
Female : Male = 9:1 (reproductive age 17-55 years)
↓
Female : Male = 2:1 (childhood or >65 years)
↓
Peak age: 20s-30s (but can occur at any age)
↓
More severe in: African-Americans > Hispanic > European-Americans
🔬 PATHOGENESIS DIAGRAM (Robbins Fig. 6.25)
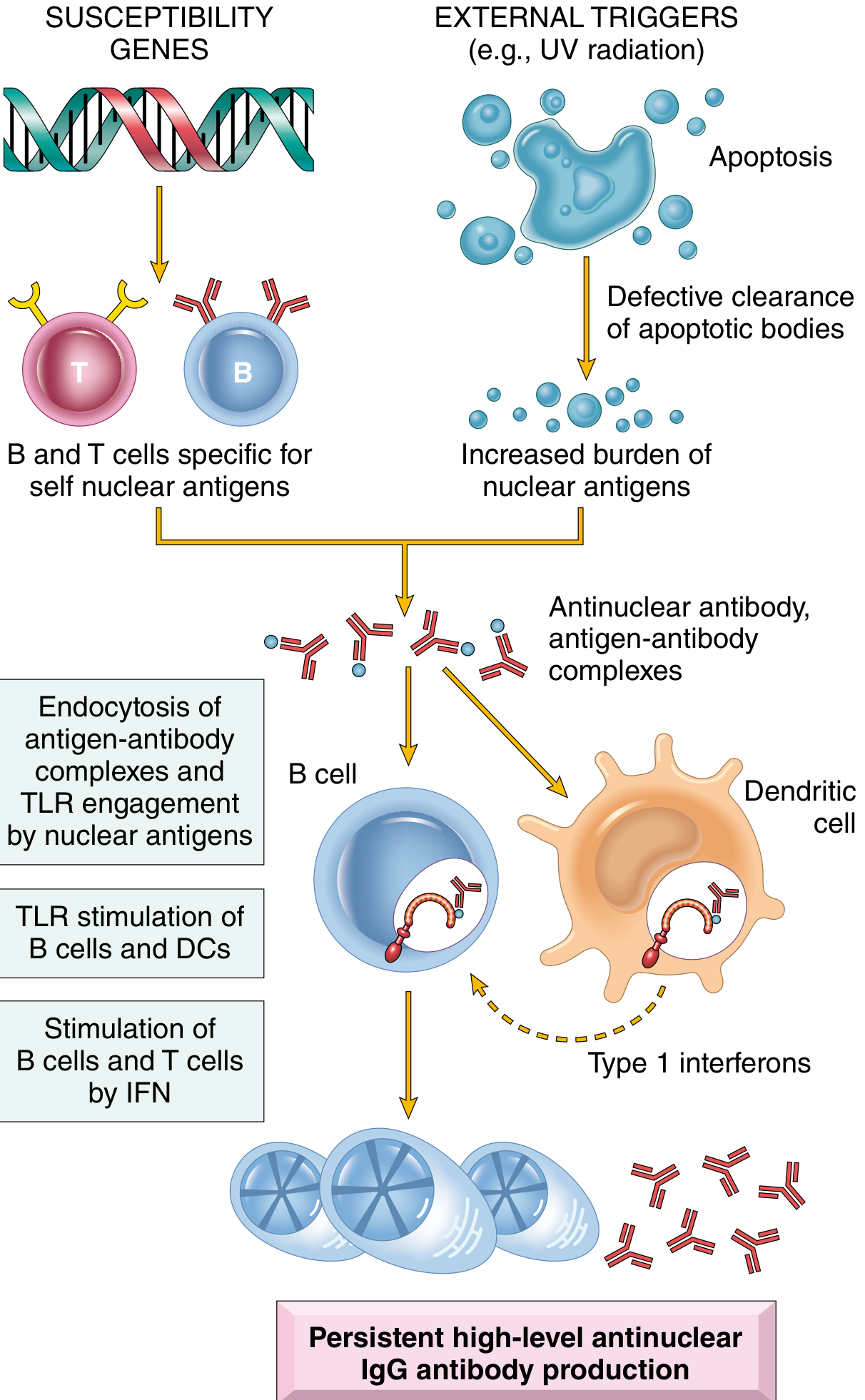
Pathogenesis Flowchart
SUSCEPTIBILITY GENES + EXTERNAL TRIGGERS (UV, drugs, viruses)
↓
Defective clearance of apoptotic cells
↓
Increased burden of nuclear antigens (DNA, RNA, histones)
↓
┌─────────────────────────┐
│ Self-reactive B cells │ + CD4+ helper T cells specific for nuclear antigens
│ escape tolerance │
└──────────┬──────────────┘
↓
Antinuclear antibodies (ANAs) produced
↓
Immune complexes formed
↙ ↘
TLR engagement Dendritic cells activated
by nuclear → Type I Interferons produced
antigens → Amplifies B & T cell activation
↘ ↙
PERSISTENT HIGH-LEVEL ANA IgG PRODUCTION
↓
Tissue injury via:
├── Immune complex deposition → Type III hypersensitivity
├── Antibody to cells → Type II hypersensitivity (cytopenias)
└── Antiphospholipid antibodies → Thrombosis
Three Main Factors in Pathogenesis
| Factor | Details |
|---|---|
| Genetic | HLA-DQ alleles; C1q, C2, C4 deficiency; GWAS loci (lymphocyte signaling, IFN response genes) |
| Immunologic | Failure of B-cell tolerance; activated autoreactive CD4+ T cells; TLR activation by self-nucleic acids; Type I IFN excess |
| Environmental | UV light (induces apoptosis, enhances TLR recognition of DNA); Drugs (hydralazine, procainamide, D-penicillamine); Sex hormones (estrogen effect) |
🧬 AUTOANTIBODIES IN SLE
Key Table: Autoantibodies and Their Significance
| Autoantibody | % Positive | Clinical Significance |
|---|---|---|
| Anti-dsDNA (double-stranded DNA) | 40-60% | Specific for SLE; correlates with nephritis & disease activity |
| Anti-Smith (Sm) | 20-30% | Virtually diagnostic of SLE (most specific) |
| Anti-U1-RNP | 30-40% | Specific for SLE; mixed connective tissue disease |
| Anti-Ro (SS-A) | 30-50% | Neonatal lupus; congenital heart block; Sjögren syndrome overlap |
| Antiphospholipid (anti-PL) | 30-40% | Antiphospholipid syndrome → thrombosis, recurrent miscarriage |
| Generic ANAs | 95-100% | Screening test; NOT specific (found in other autoimmune diseases) |
| Anti-histone | ~70% | Drug-induced lupus |
ANA Patterns (Immunofluorescence)
ANA Staining Pattern:
├── Homogeneous/Diffuse → anti-dsDNA, anti-histones, anti-nucleosomes → SLE
├── Speckled (coarse) → anti-Sm, anti-RNP → SLE / MCTD
├── Rim/Peripheral → anti-dsDNA → SLE (highly specific)
├── Nucleolar → anti-RNA polymerase → Systemic Sclerosis
└── Centromeric → anti-CENP → Systemic Sclerosis (CREST)
Key Exam Fact: False positive VDRL/syphilis test in SLE is due to antiphospholipid antibodies cross-reacting with cardiolipin antigen used in the test.
Lupus anticoagulant paradox: Despite prolonging PTT in vitro, antiphospholipid antibodies cause a hypercoagulable state in vivo (thrombosis, not bleeding).
🏥 DIAGNOSTIC CRITERIA (ACR 1997 Revised)
| Clinical Criteria | Definition |
|---|---|
| Malar (butterfly) rash | Fixed erythema over malar eminences ("butterfly" pattern) |
| Discoid rash | Erythematous raised patches with keratotic scaling |
| Photosensitivity | Skin rash on UV exposure |
| Oral ulcers | Usually painless oral/nasopharyngeal ulceration |
| Non-scarring alopecia | Diffuse thinning without scarring |
| Joint disease | Nonerosive synovitis in ≥2 peripheral joints |
| Serositis | Pleuritis or pericarditis |
| Renal disorder | Proteinuria >0.5g/24h or red cell casts |
| Neurologic disorder | Seizures, psychosis, myelitis, neuropathy |
| Hemolytic anemia | Coombs-positive hemolytic anemia |
| Leukopenia/lymphopenia | WBC <4000 or lymphocytes <1500 on 2+ occasions |
| Thrombocytopenia | Platelets <100,000 on 2+ occasions |
Immunologic Criteria: anti-dsDNA, anti-Sm, antiphospholipid antibodies, low complement, direct Coombs test
Diagnosis: ≥4 criteria (sensitivity 85%, specificity 95%)
🔬 MORPHOLOGY / ORGAN PATHOLOGY
Overview Flowchart
IMMUNE COMPLEX DEPOSITION
↓
┌────┴──────────────────────────────────────┐
↓ ↓ ↓ ↓ ↓
SKIN KIDNEY JOINTS HEART BLOOD
(50%) (40-70%) VESSELS VESSELS
1. SKIN
The "Butterfly Rash" - malar erythema in ~50% of patients
Microscopic (Histology):
EPIDERMIS:
└── Vacuolar degeneration of basal layer (liquefactive degeneration)
└── Edema at dermoepidermal junction
DERMIS:
└── Perivascular lymphocytic inflammation
└── Vasculitis with fibrinoid necrosis
IMMUNOFLUORESCENCE (Lupus Band Test):
└── IgG + Complement deposits at dermoepidermal junction
→ Present in BOTH involved AND uninvolved skin
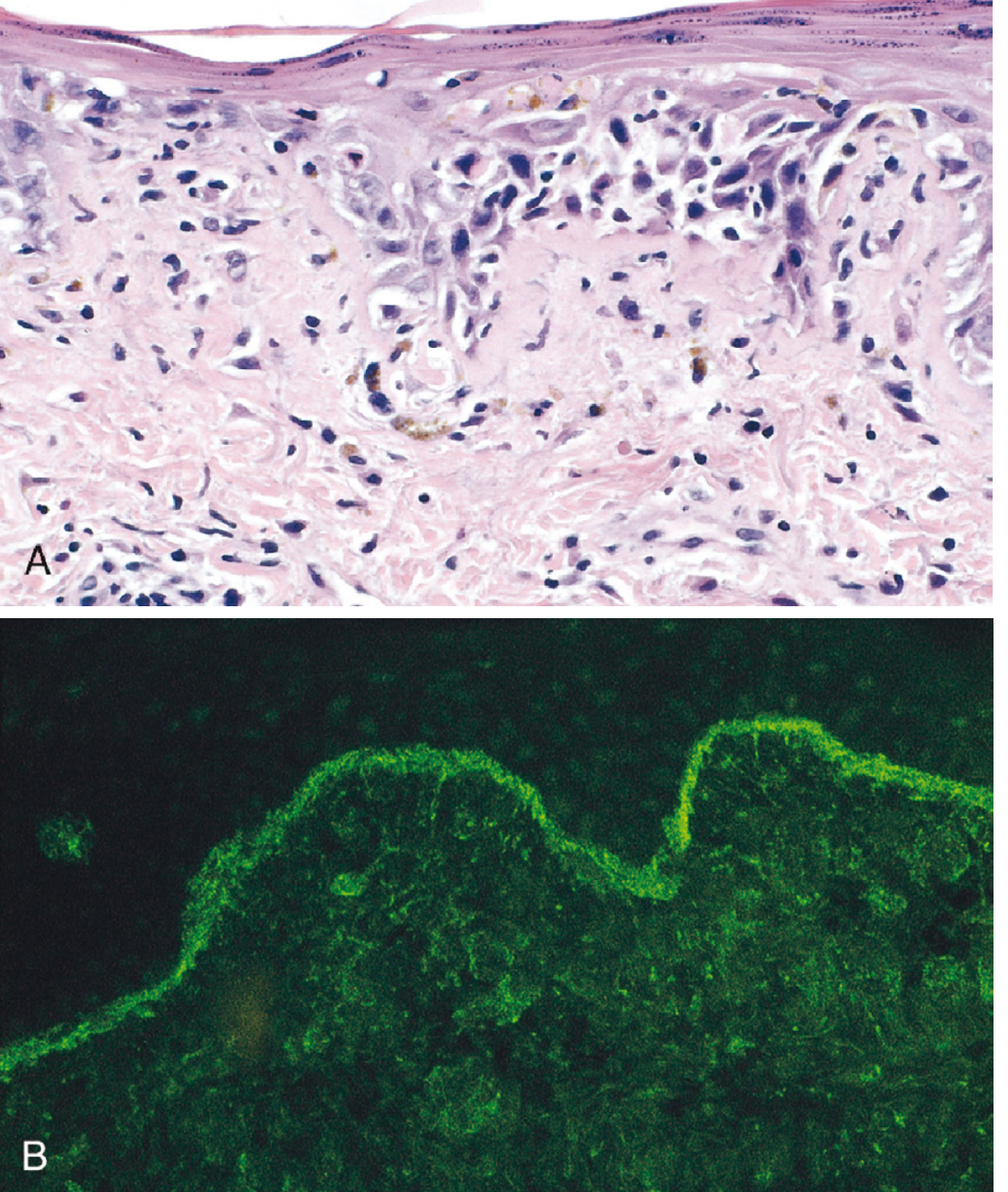
- (A) H&E: vacuolar degeneration of basal epidermis + dermal edema
- (B) Immunofluorescence: bright IgG deposits along the dermoepidermal junction (the "lupus band")
2. KIDNEY (Lupus Nephritis)
Up to 40-70% of SLE patients have clinically significant renal disease.
WHO/ISN Classification of Lupus Nephritis
| Class | Name | Pattern | Key Feature |
|---|---|---|---|
| I | Minimal mesangial | LM normal, IF positive | Mesangial immune deposits only |
| II | Mesangial proliferative | Mesangial expansion | Mesangial hypercellularity |
| III | Focal proliferative | <50% glomeruli | Focal segmental lesions |
| IV | Diffuse proliferative | >50% glomeruli | Most severe; "wire loop" lesions |
| V | Membranous | Diffuse thickening | Sub-epithelial deposits, nephrotic syndrome |
| VI | Advanced sclerosis | >90% glomeruli sclerosed | End-stage |
Class IV - Diffuse Proliferative GN (Most Important):
Massive subendothelial immune complex deposits
↓
"Wire loop" lesion on LM (GBM thickening)
↓
Endothelial swelling + neutrophil infiltration
↓
Complement activation → fibrinoid necrosis
↓
Hematuria + Proteinuria + Hypertension
↓
If untreated → Renal failure
Immunofluorescence in Lupus Nephritis:
- "Full house" pattern: IgG, IgA, IgM + C3, C1q all positive
- C1q deposition is characteristic of lupus nephritis
3. HEART
Libman-Sacks Endocarditis - the hallmark cardiac lesion of SLE
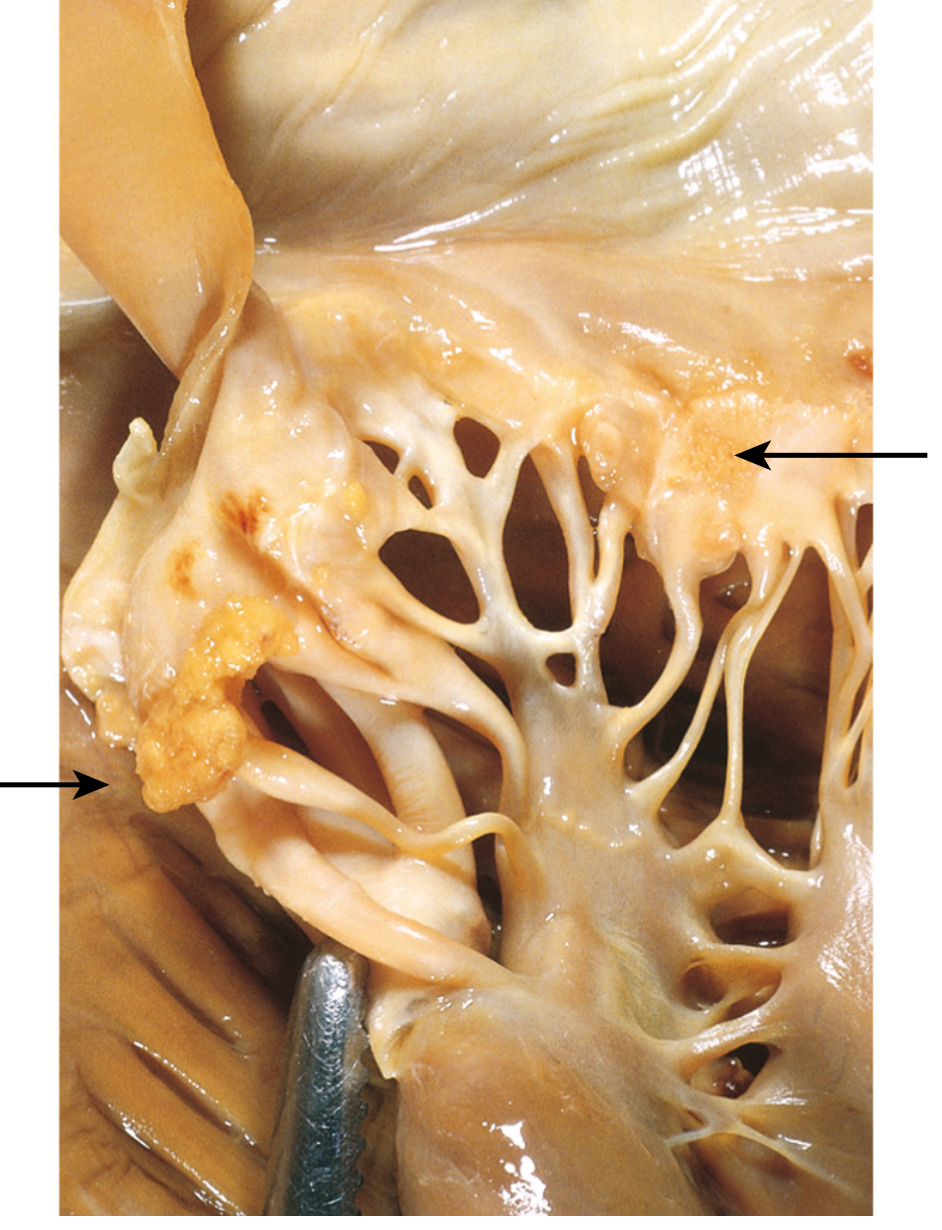
Gross specimen: irregular warty vegetations on BOTH surfaces of valve leaflets (arrows) - unlike infective endocarditis which is on atrial surface only
Libman-Sacks Endocarditis:
├── Small (1-4mm), sterile, warty vegetations
├── Located on BOTH surfaces of valve leaflets
│ (atrial AND ventricular surface - distinguishes from RF)
├── Most common: Mitral valve > Tricuspid
├── Mechanism: immune complex deposition + inflammation
└── Complications: embolism, valve dysfunction, secondary infection
Other cardiac features:
- Fibrinous pericarditis (serositis) - most common cardiac manifestation
- Myocarditis
- Accelerated coronary artery disease (from chronic inflammation)
4. BLOOD VESSELS
Acute phase:
└── Necrotizing vasculitis
├── Capillaries, small arteries, arterioles affected
├── Fibrinoid necrosis of vessel walls
└── Can affect ANY tissue
Chronic phase:
└── Fibrous thickening of vessel wall
└── Luminal narrowing → ischemia
"Onion skin" lesion in spleen - concentric perivascular fibrosis of splenic central arteries (pathognomonic finding in spleen in SLE)
5. JOINTS
- Nonerosive synovitis in 2+ peripheral joints
- Synovial inflammation without cartilage/bone destruction
- Jaccoud arthropathy (chronic deformity without erosion) in some
6. SPLEEN
- Splenomegaly
- Follicular hyperplasia
- "Onion skin" lesion: perivascular fibrosis of central arterioles (characteristic/pathognomonic)
7. BLOOD (Cytopenias)
Mechanism: Type II Hypersensitivity - autoantibodies opsonize cells → phagocytosis
Anti-RBC antibodies → Coombs-positive hemolytic anemia (~50%)
Anti-platelet antibodies → Thrombocytopenia (~10%)
Anti-lymphocyte antibodies → Lymphopenia
8. LUNGS
- Pleuritis + pleural effusion (serositis)
- Interstitial pneumonitis
- Pulmonary hypertension
9. CNS
- Neuropsychiatric SLE
- Mechanism: antibodies cross the blood-brain barrier, react with neurons/neurotransmitter receptors
- Cognitive dysfunction, psychosis, seizures
⚡ MECHANISMS OF TISSUE INJURY - Summary
MECHANISM MANIFESTATION
──────────────────────────────────────────────────
Type II Hypersensitivity → Hemolytic anemia
(Ab against cell surface) Thrombocytopenia
Lymphopenia
Type III Hypersensitivity → Glomerulonephritis
(Immune complex → Vasculitis
deposition) → Skin rash
→ Synovitis
→ Serositis
Antiphospholipid Ab → Thrombosis (arterial & venous)
→ Recurrent miscarriages
→ Stroke, DVT, PE
📈 CLINICAL FEATURES - Memory Aid: "SOAP BRAIN MD"
| Letter | Feature |
|---|---|
| S | Serositis (pleuritis/pericarditis) |
| O | Oral ulcers |
| A | Arthritis (nonerosive) |
| P | Photosensitivity |
| B | Blood disorders (anemia, leukopenia, thrombocytopenia) |
| R | Renal disorder (proteinuria, RBC casts) |
| A | ANA positive |
| I | Immunologic (anti-dsDNA, anti-Sm, antiphospholipid) |
| N | Neurologic (seizures, psychosis) |
| M | Malar rash |
| D | Discoid rash |
💊 DRUG-INDUCED LUPUS
Causative drugs:
├── Hydralazine
├── Procainamide ← Most common
├── D-penicillamine
├── Isoniazid
└── Methyldopa
Key features:
├── Anti-HISTONE antibodies (not anti-dsDNA)
├── No renal/CNS involvement (usually)
├── REVERSIBLE on stopping drug
└── ANA positive
🔬 SPECIAL HISTOLOGICAL FINDINGS IN SLE
| Finding | Location | Significance |
|---|---|---|
| Vacuolar degeneration of basal layer | Skin | Characteristic histology |
| Lupus band (IgG at DEJ) | Skin | On immunofluorescence |
| "Wire loop" lesions | Kidney (GBM) | Class IV lupus nephritis |
| "Full house" immunofluorescence | Kidney | C1q, C3, IgG, IgA, IgM all positive |
| Libman-Sacks vegetations | Mitral/Tricuspid valve | Bilateral-surface warty vegetations |
| "Onion skin" lesion | Spleen (central arterioles) | Concentric perivascular fibrosis |
| LE cell | Blood/bone marrow | PMN engulfing hematoxylin body (denatured nucleus) |
| Hematoxylin bodies | Tissue | In vivo equivalent of LE cell; pathognomonic |
| Fibrinoid necrosis | Blood vessels | Acute vasculitis |
LE Cell - Classic Finding
Nuclear material (denatured DNA) + Antibody (anti-dsDNA)
↓
Opsonized nuclear material
↓
Phagocytosed by PMN (neutrophil)
↓
LE CELL = PMN containing a large homogeneous
nuclear inclusion (hematoxylin body)
📊 COURSE AND PROGNOSIS
CLINICAL COURSE:
Relapsing and Remitting over years/decades
↓
During flares: ↑ immune complexes → ↓ complement (hypocomplementemia)
↓
Treatment: Corticosteroids + Hydroxychloroquine + Immunosuppressives
PROGNOSIS:
├── 5-year survival: ~90%
├── 10-year survival: ~80%
└── Most common causes of death:
├── Renal failure (lupus nephritis)
├── Intercurrent infections (immunosuppression)
└── Cardiovascular disease (accelerated atherosclerosis)
🏁 QUICK REVISION BOX
SLE at a Glance:
┌─────────────────────────────────────────────────────────┐
│ TYPE: Autoimmune; Type III (+ Type II) hypersensitivity │
│ GENDER: F:M = 9:1 │
│ HALLMARK Ab: Anti-dsDNA (most specific), Anti-Sm │
│ BEST SCREENING TEST: ANA (95-100% sensitive) │
│ KIDNEY: Diffuse proliferative GN (Class IV) = most severe│
│ HEART: Libman-Sacks endocarditis (both valve surfaces) │
│ SKIN: Butterfly rash + Vacuolar degeneration (basal) │
│ SPLEEN: Onion skin lesion │
│ KEY FINDING: LE cell, Hematoxylin bodies │
│ DRUG-INDUCED: Anti-histone Ab, procainamide │
│ FALSE +ve VDRL due to: antiphospholipid Ab │
└─────────────────────────────────────────────────────────┘
Sources: Robbins & Cotran Pathologic Basis of Disease (10e), p. 213-219 | Robbins & Kumar Basic Pathology, p. 179-186
This is a shared conversation. Sign in to Orris to start your own chat.