Brachial plexus
Reading File
Finding Sources
Searching Images
brachial plexus anatomy diagram
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a comprehensive overview of the brachial plexus.
Brachial Plexus
Formation
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5–C8 and T1 (occasionally with contributions from C4 or T2 in prefixed/postfixed variants). It originates in the neck, passes laterally and inferiorly over rib I, and enters the axilla. It is approximately 15 cm long in adults.
Mnemonic for the components (proximal → distal): Robert Taylor Drinks Cold Beer → Roots, Trunks, Divisions, Cords, Branches
Components
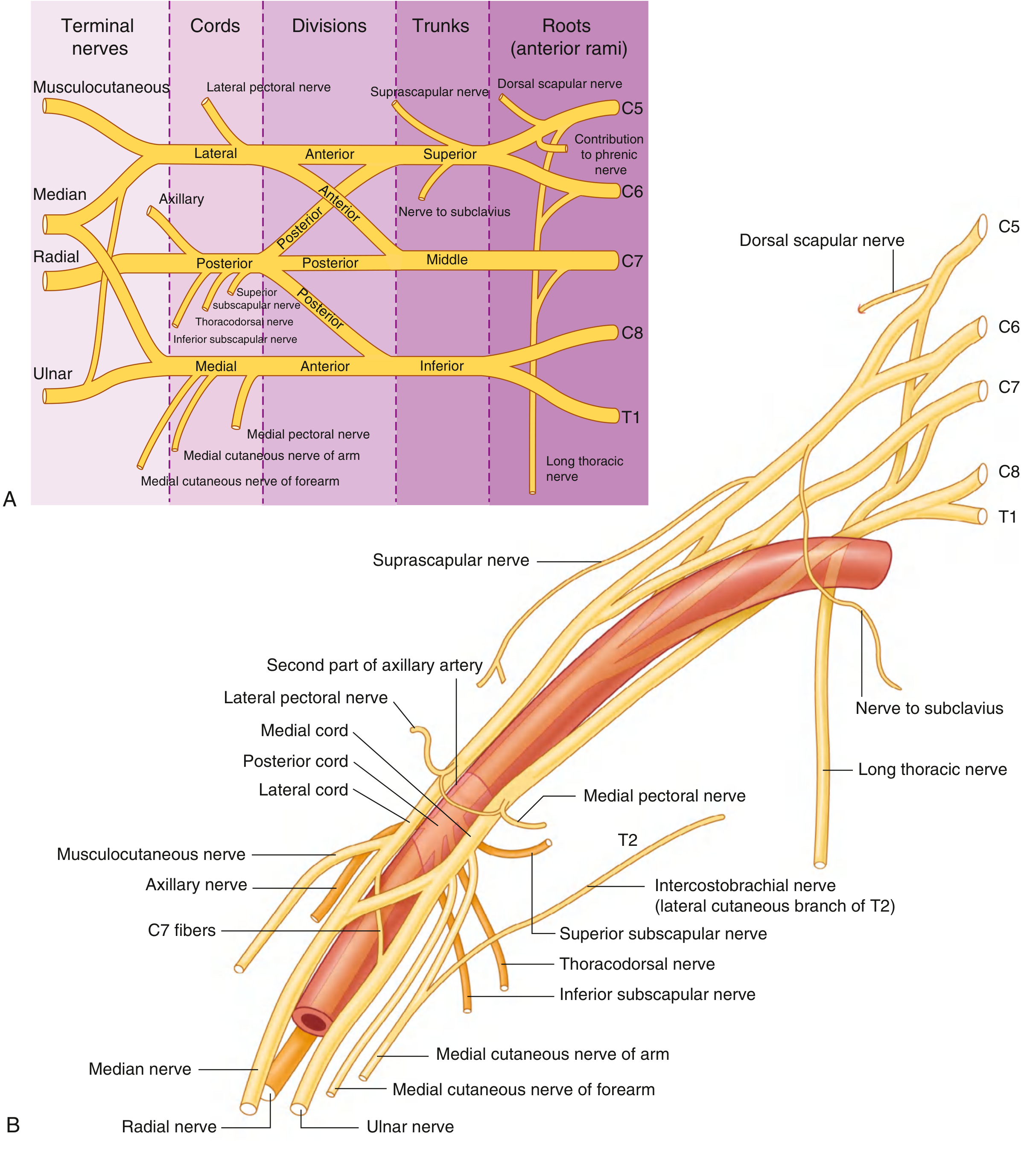

1. Roots
- Anterior rami of C5, C6, C7, C8, T1
- Pass between the anterior and middle scalene muscles
- Receive gray rami communicantes from the sympathetic trunk
- Lie superior and posterior to the subclavian artery
2. Trunks (3)
| Trunk | Roots |
|---|---|
| Superior (upper) | C5 + C6 |
| Middle | C7 |
| Inferior (lower) | C8 + T1 |
The inferior trunk lies on rib I, posterior to the subclavian artery. The trunks cross the base of the posterior triangle of the neck.
3. Divisions (6)
- Each trunk splits into an anterior and a posterior division
- Anterior divisions → nerves supplying anterior (flexor) compartments
- Posterior divisions → nerves supplying posterior (extensor) compartments
- No peripheral nerves arise directly from divisions
4. Cords (3)
Named by their relationship to the second part of the axillary artery:
| Cord | Origin | Contents | Position |
|---|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5–C7 | Lateral to axillary artery |
| Medial | Anterior division of inferior trunk | C8–T1 | Medial to axillary artery |
| Posterior | All three posterior divisions | C5–T1 | Posterior to axillary artery |
Branches
From the Roots
| Nerve | Roots | Target |
|---|---|---|
| Dorsal scapular nerve | C5 (±C4) | Rhomboid major & minor, levator scapulae |
| Long thoracic nerve | C5–C7 | Serratus anterior |
| Contribution to phrenic nerve | C5 | Diaphragm |
From the Trunks
| Nerve | Origin | Target |
|---|---|---|
| Suprascapular nerve | Superior trunk (C5–C6) | Supraspinatus, infraspinatus |
| Nerve to subclavius | Superior trunk (C5–C6) | Subclavius |
From the Cords
| Cord | Branches |
|---|---|
| Lateral | Lateral pectoral nerve (C5–C7); musculocutaneous nerve (C5–C7); lateral root of median nerve |
| Medial | Medial pectoral nerve (C8–T1); medial cutaneous nerve of arm (C8–T1); medial cutaneous nerve of forearm (C8–T1); ulnar nerve (C7–T1); medial root of median nerve |
| Posterior | Superior & inferior subscapular nerves (C5–C7); thoracodorsal nerve (C6–C8); axillary nerve (C5–C6); radial nerve (C5–C8) |
The median nerve is formed by contributions from both lateral (C5–C7) and medial (C8–T1) cords.
Anatomical Variations
- Prefixed plexus (3–5% of individuals): contribution shifted up; strong C4, minimal/no T1
- Postfixed plexus (3–5%): shifted down; minimal C5, contribution from T2
- These variations must be considered when the clinical deficit doesn't fit the expected pattern of a plexopathy
Lesions of the Brachial Plexus
Upper Trunk (C5–C6) — Erb–Duchenne Palsy
- Caused by: birth trauma (shoulder dystocia), forceful separation of neck and shoulder
- Paralysis of: deltoid, biceps, brachialis, brachioradialis
- Posture: arm hangs adducted, internally rotated, forearm pronated ("waiter's tip")
- Sensory loss: lateral arm/forearm
Lower Trunk (C8–T1) — Klumpke Palsy
- Caused by: Pancoast tumor, forced abduction of arm, birth trauma (breech delivery)
- Paralysis of: intrinsic hand muscles (interossei, hypothenar, thenar)
- "Claw hand" deformity
- Sensory loss: medial arm/forearm and medial two fingers
- May include Horner syndrome (ptosis, miosis, anhidrosis) if T1 sympathetic fibers involved
Traumatic Plexopathy
- Most common cause: traction injuries in motor vehicle accidents (especially motorcyclists propelled from the vehicle)
- Other causes: gunshot wounds, fracture-dislocations of shoulder/humerus, radiation (delayed), Pancoast tumors, neuralgic amyotrophy (Parsonage–Turner syndrome)
Clinical Pearls
- Serratus anterior weakness (long thoracic nerve, C5–C7) → winged scapula — tested by asking patient to push against a wall
- Suprascapular nerve is the only branch from a trunk; it exits at Erb's point (junction of C5 + C6)
- The posterior cord contains fibers from all five roots (C5–T1) — posterior cord lesions affect the entire posterior compartment of the upper limb
- The intercostobrachial nerve (lateral cutaneous branch of T2) is not part of the brachial plexus but often co-injured in axillary dissection
Sources: Gray's Anatomy for Students (9780323934237); Localization in Clinical Neurology, 8e (9781975160241)
Temporomandibular joint
Finding Sources
Searching Images
temporomandibular joint anatomy diagram
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive information from multiple textbooks. Here is a thorough overview of the Temporomandibular Joint (TMJ).
Temporomandibular Joint (TMJ)
Anatomy
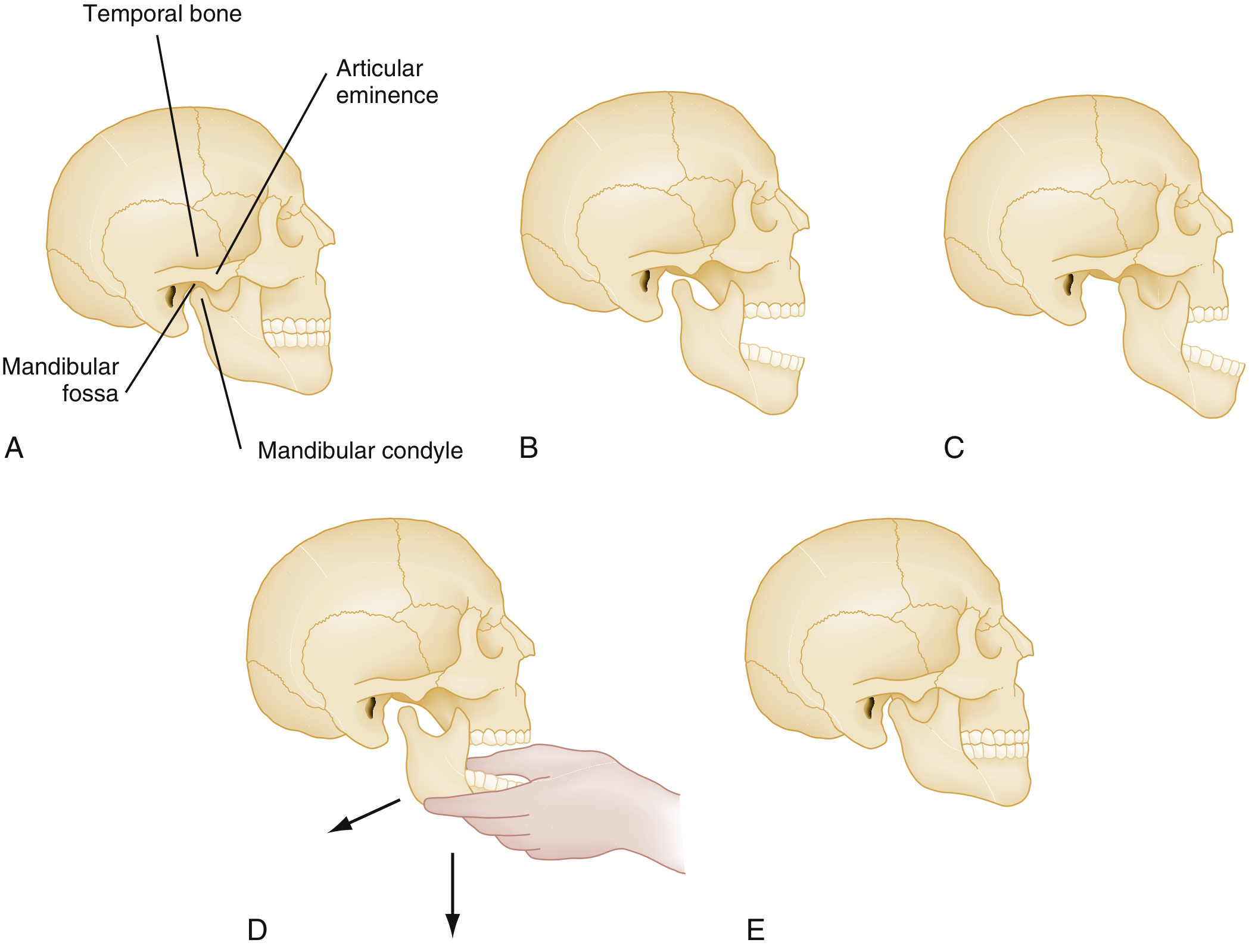
The TMJ is the articulation between the condyle (head) of the mandible and the squamous part of the temporal bone — specifically the mandibular (glenoid) fossa and the articular eminence (articular tubercle) in front of it.
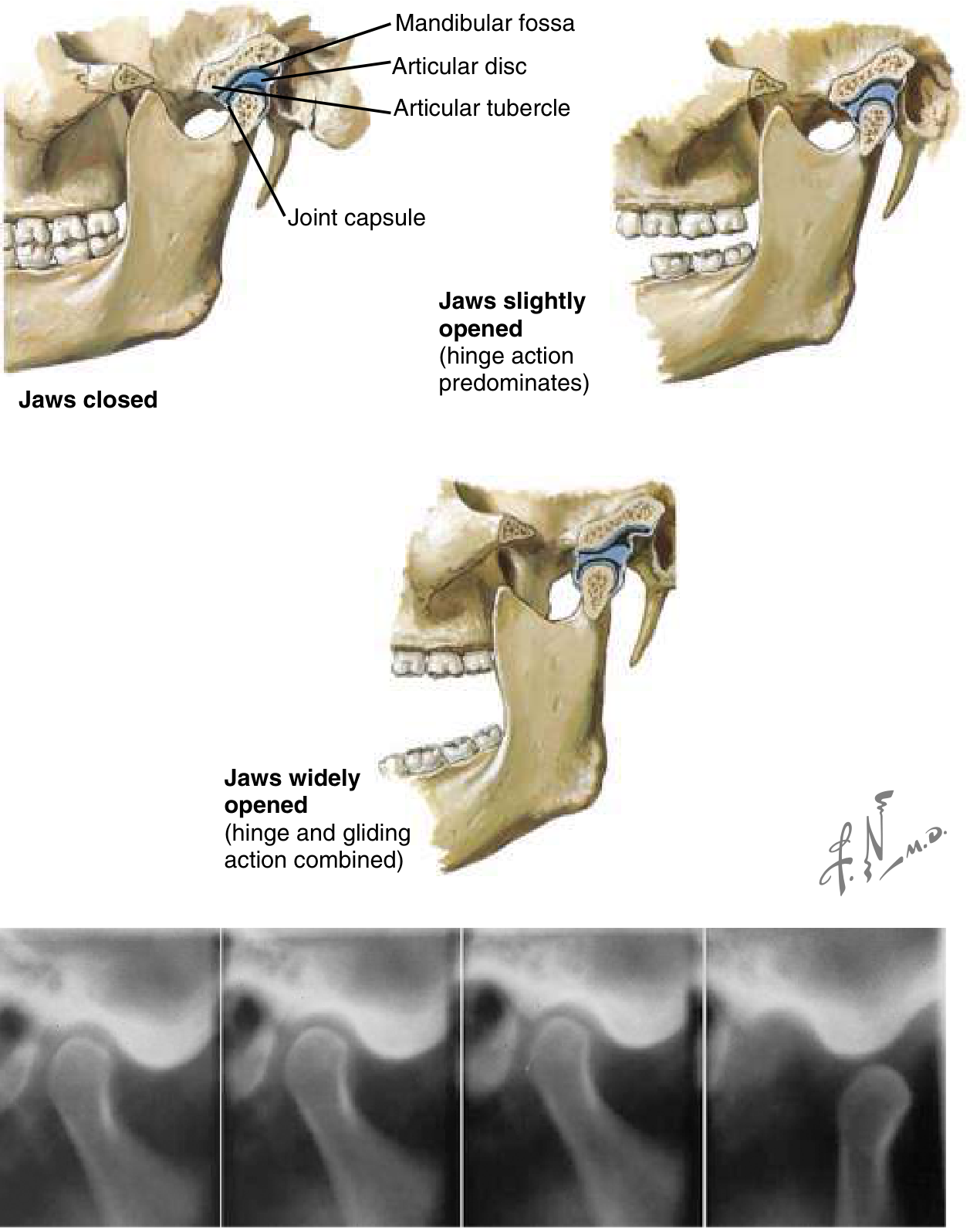
It is classified as a synovial joint but is unique in having two distinct joint types combined:
| Action | Joint type | Occurs when |
|---|---|---|
| Rotation (hinge) | Ginglymoid | Slight/normal mouth opening |
| Translation (gliding) | Arthrodial | Wide mouth opening |
During wide opening, the articular disc and condyle complex slide anteriorly and inferiorly along the articular eminence. Dislocation occurs when the condyle moves anterior to the articular eminence.
The Articular Disc (Meniscus)
- A biconcave fibrocartilaginous disc that sits between the condyle and the temporal bone
- Divides the joint into two compartments:
- Superior (upper) joint space — between disc and temporal bone; allows gliding/translation
- Inferior (lower) joint space — between disc and condyle; allows rotation/hinging
- Anteriorly attached to the lateral pterygoid muscle (upper head)
- Posteriorly attached to the bilaminar zone (retrodiscal tissue) — richly vascularized and innervated
A formal thick capsule is absent at the anteromedial portion of the joint; this looser synovial tissue permits translation to occur.
Capsule & Ligaments
| Structure | Details |
|---|---|
| Joint capsule | Fibrous; encloses the entire joint |
| Lateral (temporomandibular) ligament | Primary intrinsic ligament; two parts (oblique and horizontal); limits posterior and inferior displacement of condyle |
| Sphenomandibular ligament | Accessory extrinsic ligament; spans from spine of sphenoid to lingula of mandible |
| Stylomandibular ligament | Thickening of parotid fascia; from styloid process to mandibular angle; limits excessive mouth protrusion |
Muscles of Mastication Acting on the TMJ
| Muscle | Nerve | Primary action |
|---|---|---|
| Masseter | V3 (masseteric n.) | Elevation (jaw closure) |
| Temporalis | V3 (deep temporal nn.) | Elevation + retraction |
| Medial pterygoid | V3 | Elevation + protrusion |
| Lateral pterygoid | V3 | Protrusion, depression, side-to-side; upper head attaches to disc |
Trismus (inability to open) results from spasm of the masseter, temporalis, and medial pterygoid.
Innervation & Blood Supply
- Innervation: Auriculotemporal nerve and masseteric nerve — both branches of V3 (mandibular division of trigeminal nerve)
- Blood supply: Superficial temporal artery and maxillary artery — branches of the external carotid artery
TMJ Disorders (TMD)
TMD is defined as "aching in the muscles of mastication, sometimes with occasional brief severe pain on chewing, often associated with restricted jaw movement and clicking or popping sounds."
Etiology
- Jaw clenching and grinding (bruxism) associated with stress — most common
- Parafunctional habits (microtrauma)
- Macrotrauma (single injury)
- Tooth malocclusion is rare as a standalone cause
Clinical Features
| Finding | Significance |
|---|---|
| Clicking/popping on opening | Disc displacement with reduction |
| Crepitus | Disc degeneration/perforation or OA |
| Limited mouth opening (≤25–30 mm interincisal) | Disc displacement without reduction (closed lock) |
| Pain anterior to auricular canal | Classic location |
| Headache, facial pain, earache | Common referral patterns |
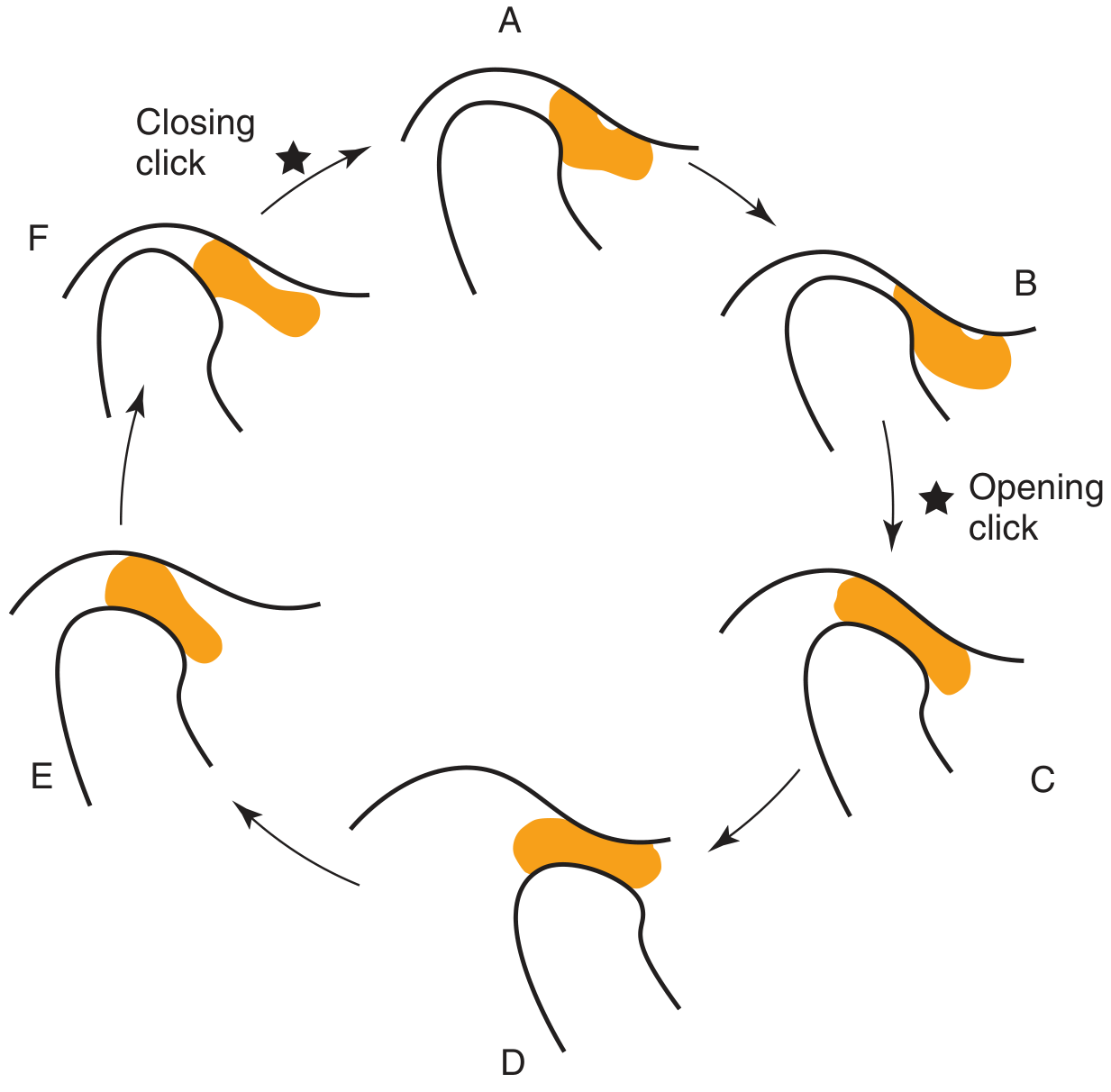
Disc Displacement (Internal Derangement)
With reduction — disc is anteriorly displaced at rest but reduces (recaptures) during mouth opening:
- Produces an audible click on opening (and sometimes a reciprocal click on closing)
- Normal range of motion
- Often asymptomatic and requires no treatment
Without reduction (closed lock) — disc remains anteriorly displaced:
- Acts as a physical barrier to condylar translation
- Maximum opening limited to 25–30 mm
- No click
- May be painful
TMJ Dislocation
Mechanism
- Condyle translates anterior to the articular eminence and becomes locked in the anterosuperior aspect of the eminence
- Masseter, temporalis, and medial pterygoid go into spasm — trismus prevents spontaneous reduction
- Caused by: extreme yawning, prolonged dental procedures, trauma, dystonic drug reactions
Clinical Features
- Mouth stuck open, unable to close
- Drooling, garbled speech
- Visible/palpable depression in the preauricular area
- Unilateral: jaw deviates to the opposite side
- Bilateral: symmetric jaw protrusion
Reduction Technique
- Procedural sedation and analgesia (masseter relaxation is essential)
- Patient seated upright, clinician in front
- Thumbs placed on the buccal sulcus lateral to the lower molars (wrap thumbs in gauze)
- Apply downward pressure on the molar ridge while rotating the chin upward and backward
- Condyle clears the eminence → masticatory muscles contract the jaw shut
Post-reduction imaging not required for atraumatic dislocation. If trauma is suspected, obtain Panorex or CT first to exclude fracture before manipulation.
Management of TMD
| Stage | Treatment |
|---|---|
| First-line | NSAIDs, soft diet, heat/ice (15 min, 4–6×/day), self-limitation of opening |
| Bruxism | Occlusal splint (bite guard) |
| Refractory | Diazepam (2–5 mg PO q8h PRN), physical therapy, TENS |
| Surgical (absolute indications) | Neoplasm, growth abnormality, ankylosis |
| Surgical (relative — refractory to conservative Rx) | Arthrocentesis (70–90% success), arthroscopy (80–90% success), open joint surgery |
Differential Diagnosis of TMJ Pain
- Pulpitis / odontogenic infection
- Otitis media
- Sinusitis
- Parotitis
- Trigeminal neuralgia
- Headache disorders
- Cervical spine disease
Sources: Rosen's Emergency Medicine (9780323757898); Cummings Otolaryngology Head and Neck Surgery (9780323612173); Localization in Clinical Neurology 8e (9781975160241)
This is a shared conversation. Sign in to Orris to start your own chat.