Hi I want to be a gastroenterologist I want you to teach me each and everything from scratch
Asking for Preferences
Reading File
Finding Sources
Searching the Web
gastroenterology full curriculum MBBS medical student learning roadmap 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have enough to now give you a thorough, well-structured response. Let me build your complete gastroenterology learning roadmap.
🏥 Your Complete Gastroenterology Learning Roadmap
Welcome! Since you're an MBBS/MD student wanting a full curriculum from scratch, here is your structured, progressive pathway. Think of this as your personal gastroenterology residency curriculum - we'll go through every domain systematically.
📚 Your Primary Textbooks (Available in Our Library)
| Textbook | Purpose |
|---|---|
| Yamada's Textbook of Gastroenterology, 7th ed (3 volumes) | The gold-standard comprehensive GI reference |
| Sleisenger & Fordtran's GI and Liver Disease | Clinical disease management bible |
| Clinical Gastrointestinal Endoscopy, 3rd ed | Procedures and endoscopy techniques |
| Harrison's Principles of Internal Medicine 22E (2025) | GI sections + systemic disease connections |
| Robbins & Cotran Pathologic Basis of Disease | GI pathology |
| Gray's Anatomy for Students | GI anatomy foundations |
🗺️ The Full Curriculum - 10 Modules
We will go through each of these modules one by one, in sessions. Each module builds on the previous one.
MODULE 1 - Foundations (Start Here)
GI Anatomy & Embryology
- Embryological development of the GI tract (foregut, midgut, hindgut)
- Gross anatomy: esophagus, stomach, small intestine, large intestine, liver, biliary system, pancreas
- Histological layers of the GI wall (mucosa, submucosa, muscularis, serosa)
- Blood supply, lymphatics, and innervation (enteric nervous system)
- Peritoneum and mesentery
GI Physiology
- Motility: peristalsis, migrating motor complex, sphincter function
- Secretion: gastric acid, pepsin, bile, pancreatic enzymes
- Digestion and absorption: carbohydrates, proteins, fats, vitamins, minerals
- Gut-brain axis and enteric nervous system (the "second brain")
- Gut microbiome basics
MODULE 2 - Esophageal Diseases
- GERD (Gastroesophageal Reflux Disease) - most common GI complaint worldwide
- Barrett's Esophagus and surveillance
- Achalasia and motility disorders
- Esophageal cancer (squamous cell vs. adenocarcinoma)
- Eosinophilic esophagitis
- Esophageal varices (portal hypertension)
- Boerhaave syndrome, Mallory-Weiss tear
MODULE 3 - Gastric & Duodenal Diseases
- Peptic ulcer disease (H. pylori, NSAIDs)
- H. pylori: diagnosis and eradication regimens
- Gastric cancer
- Gastritis (acute, chronic, autoimmune)
- Gastroparesis
- Functional dyspepsia
- Zollinger-Ellison syndrome (gastrinoma)
MODULE 4 - Small Intestinal Diseases
- Celiac disease (pathophysiology, serological markers, biopsy findings)
- Crohn's disease (vs. UC - key differences)
- Small intestinal bacterial overgrowth (SIBO)
- Carcinoid tumors / neuroendocrine tumors
- Malabsorption syndromes (tropical sprue, short bowel, Whipple disease)
- Intestinal obstruction, volvulus, intussusception
MODULE 5 - Colorectal Diseases
- Ulcerative colitis (vs. Crohn's - know this comparison cold)
- Colorectal cancer - screening, staging, molecular pathways (APC, KRAS, TP53)
- Colorectal polyps: adenomatous, hyperplastic, serrated
- Diverticular disease (diverticulosis vs. diverticulitis)
- Irritable bowel syndrome (Rome IV criteria)
- Microscopic colitis
- Anorectal disorders: hemorrhoids, fissures, fistulas, abscesses
MODULE 6 - Liver Diseases (Hepatology)
- Liver anatomy, function tests interpretation (ALT, AST, ALP, GGT, bilirubin)
- Viral hepatitis: A, B, C, D, E - complete understanding
- Cirrhosis: causes, Child-Pugh and MELD scoring
- Complications of cirrhosis: ascites, SBP, hepatic encephalopathy, HRS, esophageal varices
- Alcoholic liver disease and MASLD (formerly NAFLD)
- Autoimmune hepatitis
- Primary biliary cholangitis (PBC) and PSC
- Hepatocellular carcinoma (HCC)
- Acute liver failure
- Wilson disease, hemochromatosis, alpha-1 antitrypsin deficiency
MODULE 7 - Biliary System Diseases
- Cholelithiasis (gallstones) - types, risk factors, complications
- Cholecystitis (acute and chronic)
- Choledocholithiasis and cholangitis (Charcot's triad, Reynolds pentad)
- Primary sclerosing cholangitis (PSC)
- Cholangiocarcinoma
- ERCP - indications, technique, complications
MODULE 8 - Pancreatic Diseases
- Acute pancreatitis - causes, Ranson/Atlanta criteria, management
- Chronic pancreatitis - etiology, complications
- Pancreatic cancer (ductal adenocarcinoma) - very poor prognosis
- Pancreatic cystic lesions (IPMN, mucinous cystadenoma, serous)
- Autoimmune pancreatitis
MODULE 9 - GI Procedures & Endoscopy
- Upper GI endoscopy (EGD) - indications, technique, findings
- Colonoscopy - prep, technique, polyp removal
- ERCP - biliary and pancreatic interventions
- Endoscopic ultrasound (EUS)
- Capsule endoscopy
- Liver biopsy
- Paracentesis and hepatic procedures
- GI bleeding management (upper vs. lower)
MODULE 10 - GI Pharmacology & Clinical Skills
- PPIs, H2 blockers, antacids
- Antibiotics for H. pylori (triple/quadruple therapy)
- Antivirals for Hepatitis B and C (DAAs)
- IBD medications (aminosalicylates, corticosteroids, thiopurines, biologics)
- Laxatives and prokinetics
- Anti-diarrheals
- Reading GI imaging: CT abdomen, MRCP, abdominal X-ray
- Interpreting liver function tests, stool studies, breath tests
- Clinical approach to: GI bleeding, jaundice, ascites, dysphagia, diarrhea, constipation
🎯 How We Will Work Together
Here is the plan for our sessions:
- Tell me which module you want to start with (I recommend Module 1 - Foundations)
- Each session, I will teach you the topic with:
- Core concepts explained clearly
- Diagrams and visual aids where available
- Key clinical pearls and mnemonics
- High-yield exam points
- Case-based examples
- After each topic, I can quiz you to check your understanding
- We will reference Yamada's, Sleisenger's, and other authoritative textbooks directly from our library
✅ Recommended Starting Order
For an MBBS student, I recommend this sequence:
Week 1-2: Module 1 (Anatomy + Physiology - your foundation)
Week 3-4: Modules 2-3 (Esophagus + Stomach)
Week 5-6: Modules 4-5 (Small intestine + Colon)
Week 7-8: Module 6 (Hepatology - large topic, needs dedicated time)
Week 9: Modules 7-8 (Biliary + Pancreas)
Week 10+: Modules 9-10 (Procedures + Pharmacology + Clinical integration)
Where would you like to begin? Just say "Start Module 1" or pick any module/topic that interests you, and I will dive deep into that topic using our textbooks, with detailed explanations, images, and clinical cases.
I am pursuing BAMS And i am in 3rd prof So please teach me all type of diseases of gastroenterolist I want to be that
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I have rich content from Harrison's and Goldman-Cecil. Let me now deliver your first complete lesson.
🩺 Gastroenterology Course for BAMS 3rd Prof
Welcome - Your Personal GI Masterclass
Since you're in BAMS 3rd Proficiency, you already know Sanskrit medical terminology, Ayurvedic physiology (Agni, Koshtha, Mahasrotas), and basic anatomy. We will bridge modern gastroenterology with your existing foundation - when helpful, I'll show you how modern diseases map to Ayurvedic concepts you already know.
📖 LESSON 1 - Understanding the GI Tract (The Master System)
What is the GI Tract?
The gastrointestinal (GI) tract extends from the mouth to the anus. It is one continuous tube approximately 9 metres long in a living person. Every organ in this tube has a specific, unique job.
Think of it this way: the GI tract is like a sophisticated food processing factory with multiple assembly lines - each section receives the product, does its specific work, passes it on, and extracts what the body needs.
Ayurvedic parallel: In BAMS, you know this as Annavaha Srotas + Purishavaha Srotas. The same system, described from a different lens.
🔵 The GI Tract - Organ by Organ
1. MOUTH (Oral Cavity)
- Job: Mechanical breakdown (chewing) + chemical digestion begins
- Key secretion: Salivary amylase - breaks starch into maltose
- Clinical relevance: Oral ulcers may signal Crohn's disease, vitamin deficiencies, or autoimmune conditions
2. ESOPHAGUS
- Length: ~25 cm
- Job: Transport food from mouth to stomach - no digestion happens here
- Key structures:
- Upper Esophageal Sphincter (UES) - prevents food reflux into throat
- Lower Esophageal Sphincter (LES) - MOST IMPORTANT - prevents stomach acid from coming up
- Movement: Peristalsis (wave-like muscular contractions)
- Clinical relevance: When LES is weak → GERD (acid reflux) - one of the most common GI diseases worldwide
3. STOMACH
- Job: Storage + churning + chemical digestion
- Key secretions:
- Hydrochloric acid (HCl) - kills bacteria, activates pepsin
- Pepsin - digests proteins
- Intrinsic Factor - essential for Vitamin B12 absorption (loss = pernicious anemia)
- Mucus - protects stomach lining from its own acid
- Capacity: 1-1.5 litres after a meal
- Clinical relevance: When acid damages the mucus layer → Peptic Ulcer Disease
4. SMALL INTESTINE (The Absorption Powerhouse)
- Length: ~6-7 metres
- 3 Parts:
- Duodenum (25 cm) - receives bile and pancreatic juice; most active digestion
- Jejunum (2.5 m) - maximum nutrient absorption
- Ileum (3.5 m) - absorbs Vitamin B12 and bile salts
- Special structures: Villi + Microvilli (brush border) - increase surface area to the size of a tennis court (200 m²)!
- Key fact: 90% of all digestion and absorption happens here
- Clinical relevance: Damage to villi → Malabsorption (e.g., Celiac disease)
5. LARGE INTESTINE (Colon)
- Length: ~1.5 metres
- Parts: Cecum → Ascending → Transverse → Descending → Sigmoid → Rectum → Anus
- Job:
- Water and electrolyte absorption (turns liquid stool solid)
- Houses 100 trillion bacteria (gut microbiome)
- No significant nutrient absorption
- Daily volume: 1000-1500 mL enters, only 100-200 mL exits as stool
- Clinical relevance: Inflammation → Ulcerative Colitis; Cancer → Colorectal Cancer (3rd most common cancer worldwide)
6. LIVER
- Weight: 1.5 kg - largest internal organ
- Jobs (500+ functions!):
- Produces bile (for fat digestion)
- Metabolizes drugs, toxins, alcohol
- Produces clotting factors, albumin
- Stores glucose (as glycogen)
- Processes all nutrients absorbed from intestine (via portal vein)
- Clinical relevance: Viral hepatitis, cirrhosis, fatty liver disease, liver cancer
7. GALLBLADDER
- Job: Stores and concentrates bile made by the liver
- Releases bile when fatty food enters duodenum (CCK hormone triggers this)
- Clinical relevance: Bile + cholesterol → Gallstones (cholelithiasis) - extremely common, especially in women
8. PANCREAS
- Has TWO completely different functions:
- Exocrine (digestive): Secretes amylase, lipase, protease into duodenum
- Endocrine (hormonal): Insulin and glucagon (blood sugar control) → diabetes
- Clinical relevance: Acute pancreatitis (5/10 very painful emergency), Pancreatic cancer (silent killer)
🔵 The 4 Layers of the GI Wall
Every organ in the GI tract (esophagus to rectum) has the same 4 layers:
| Layer | What It Does | Clinical Importance |
|---|---|---|
| Mucosa (innermost) | Absorption, secretion, protection | Ulcers, cancers start here |
| Submucosa | Blood vessels, nerves (Meissner's plexus), lymphatics | Tumors invade this layer |
| Muscularis | Circular + longitudinal muscle; Auerbach's plexus | Motility disorders |
| Serosa/Adventitia (outermost) | Protective covering | Perforation goes through all layers |
🔵 Symptoms - The GI Tract's "Language"
Despite being a complex system, the GI tract expresses disease through a limited set of symptoms. As a future gastroenterologist, these are your vocabulary:
| Symptom | What It Means |
|---|---|
| Heartburn / Pyrosis | Burning behind sternum - acid reflux |
| Dysphagia | Difficulty swallowing - esophageal disease |
| Odynophagia | Painful swallowing - esophageal ulcer/infection |
| Dyspepsia | Upper abdominal discomfort/bloating after eating |
| Nausea & Vomiting | Many causes - gastric, hepatic, pancreatic |
| Hematemesis | Vomiting blood - URGENT - upper GI bleed |
| Melena | Black tarry stools - digested blood from upper GI |
| Hematochezia | Fresh red blood in stool - lower GI bleed |
| Diarrhea | >3 loose stools/day |
| Constipation | <3 stools/week or straining |
| Jaundice | Yellow skin/eyes - liver or bile duct disease |
| Ascites | Fluid in abdomen - liver failure |
Mnemonics for GI bleeding: "MELENA = blood digested (UPPER GI)" | "HEMATOCHEZIA = FRESH blood (LOWER GI)"
🔵 The 4 Mechanisms of GI Disease
All GI diseases cause problems through one or more of these mechanisms:
- Structural damage - erosion, ulceration, perforation, obstruction
- Bleeding - from ulcers, varices, tumors, inflammation
- Inflammation - IBD, hepatitis, pancreatitis
- Motility/Functional disorder - IBS, gastroparesis, achalasia
🔵 How Gastroenterologists Approach Every Patient
The systematic approach used by every GI specialist:
Step 1: HISTORY
- Location of pain/symptom
- Onset, duration, severity
- Relation to food and bowel movements
- Alarm symptoms? (weight loss, bleeding, dysphagia, fever)
- Medications, alcohol, travel history
Step 2: PHYSICAL EXAM
- Abdominal inspection → auscultation → percussion → palpation
- Check for jaundice, pallor, clubbing (liver disease)
- Check for tenderness, guarding, masses
- Rectal exam (never skip!)
Step 3: INVESTIGATIONS
- Blood: CBC, LFT, LFT, amylase, lipase, H. pylori
- Stool: culture, occult blood, parasites
- Imaging: X-ray, USG abdomen, CT scan, MRCP
- Endoscopy: OGD (upper), Colonoscopy (lower)
- Biopsy when needed
Step 4: DIAGNOSIS & TREATMENT
📋 Master List of ALL GI Diseases (Your Full Syllabus)
Here is every disease we will study, organized by organ:
🔴 ESOPHAGUS
- GERD (Gastroesophageal Reflux Disease)
- Barrett's Esophagus
- Achalasia
- Esophageal Cancer
- Eosinophilic Esophagitis
- Esophageal Varices
- Mallory-Weiss Tear
- Boerhaave Syndrome
- Diffuse Esophageal Spasm
- Esophagitis (Candidal, Herpetic, CMV)
🟠 STOMACH & DUODENUM
- Peptic Ulcer Disease (PUD)
- H. pylori infection
- Acute Gastritis
- Chronic Gastritis (Type A & B)
- Gastroparesis
- Gastric Cancer
- Zollinger-Ellison Syndrome (Gastrinoma)
- Autoimmune Gastritis (Pernicious Anemia)
- Functional Dyspepsia
- Gastric Outlet Obstruction
- Menetrier's Disease
🟡 SMALL INTESTINE
- Celiac Disease (Gluten Enteropathy)
- Crohn's Disease
- Small Intestinal Bacterial Overgrowth (SIBO)
- Whipple's Disease
- Tropical Sprue
- Short Bowel Syndrome
- Carcinoid Tumor / NET
- Small Bowel Obstruction
- Meckel's Diverticulum
- Intestinal Tuberculosis
- Giardiasis & Parasitic infections
🟢 LARGE INTESTINE & ANORECTAL
- Ulcerative Colitis (UC)
- Colorectal Cancer
- Colorectal Polyps (Adenomas, Hyperplastic, Serrated)
- Diverticulosis & Diverticulitis
- Irritable Bowel Syndrome (IBS)
- Microscopic Colitis
- Pseudomembranous Colitis (C. difficile)
- Ischemic Colitis
- Volvulus (Sigmoid & Cecal)
- Intussusception
- Hemorrhoids (Internal & External)
- Anal Fissure
- Perianal Fistula & Abscess
- Anal Cancer
🔵 LIVER
- Viral Hepatitis A, B, C, D, E
- Alcoholic Liver Disease
- MASLD / MASH (Fatty Liver Disease)
- Autoimmune Hepatitis
- Primary Biliary Cholangitis (PBC)
- Primary Sclerosing Cholangitis (PSC)
- Cirrhosis
- Portal Hypertension
- Ascites
- Spontaneous Bacterial Peritonitis (SBP)
- Hepatic Encephalopathy
- Hepatorenal Syndrome (HRS)
- Esophageal Varices & Variceal Bleeding
- Hepatocellular Carcinoma (HCC)
- Acute Liver Failure (ALF)
- Wilson's Disease
- Hemochromatosis
- Alpha-1 Antitrypsin Deficiency
- Drug-Induced Liver Injury (DILI)
- Budd-Chiari Syndrome
🟣 BILIARY SYSTEM
- Cholelithiasis (Gallstones)
- Acute Cholecystitis
- Chronic Cholecystitis
- Choledocholithiasis (CBD stones)
- Acute Cholangitis (Charcot's triad)
- Cholangiocarcinoma (Bile duct cancer)
- Primary Sclerosing Cholangitis
- Biliary Strictures
🟤 PANCREAS
- Acute Pancreatitis
- Chronic Pancreatitis
- Pancreatic Adenocarcinoma
- Pancreatic Cystic Lesions (IPMN, MCN)
- Autoimmune Pancreatitis
- Pancreatic Neuroendocrine Tumors (NETs)
- Pancreatic Exocrine Insufficiency
✅ Session Summary - What You Learned Today
- The GI tract: 8 organs, each with a specific job
- The 4 wall layers and their clinical significance
- The master symptom list of GI disease
- The 4 mechanisms of all GI disease
- The systematic clinical approach
- All 81 GI diseases organized by organ (your full syllabus!)
🎯 What's Coming in Lesson 2
We will dive deep into the most common GI disease in the world:
GERD - Gastroesophageal Reflux Disease
- Exact mechanism (why the acid goes up)
- Causes and risk factors
- Symptoms, complications
- How to diagnose it
- How to treat it (lifestyle + medicines)
- Barrett's esophagus - when GERD becomes dangerous
- Case studies
Just reply "Lesson 2" or "Next" and we begin immediately! You can also jump to any specific disease from the list above - just name it and I'll teach it in full detail. 🚀
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Goldman-Cecil Medicine | Yamada's Textbook of Gastroenterology 7E | Sleisenger & Fordtran's GI and Liver Disease
Next
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Excellent - I have textbook content from Fischer's Mastery of Surgery, Goldman-Cecil, Yamada's, and Harrison's. Now I'll deliver your full GERD lesson.
📖 LESSON 2 - GERD (Gastroesophageal Reflux Disease)
The Most Common GI Disease in the World
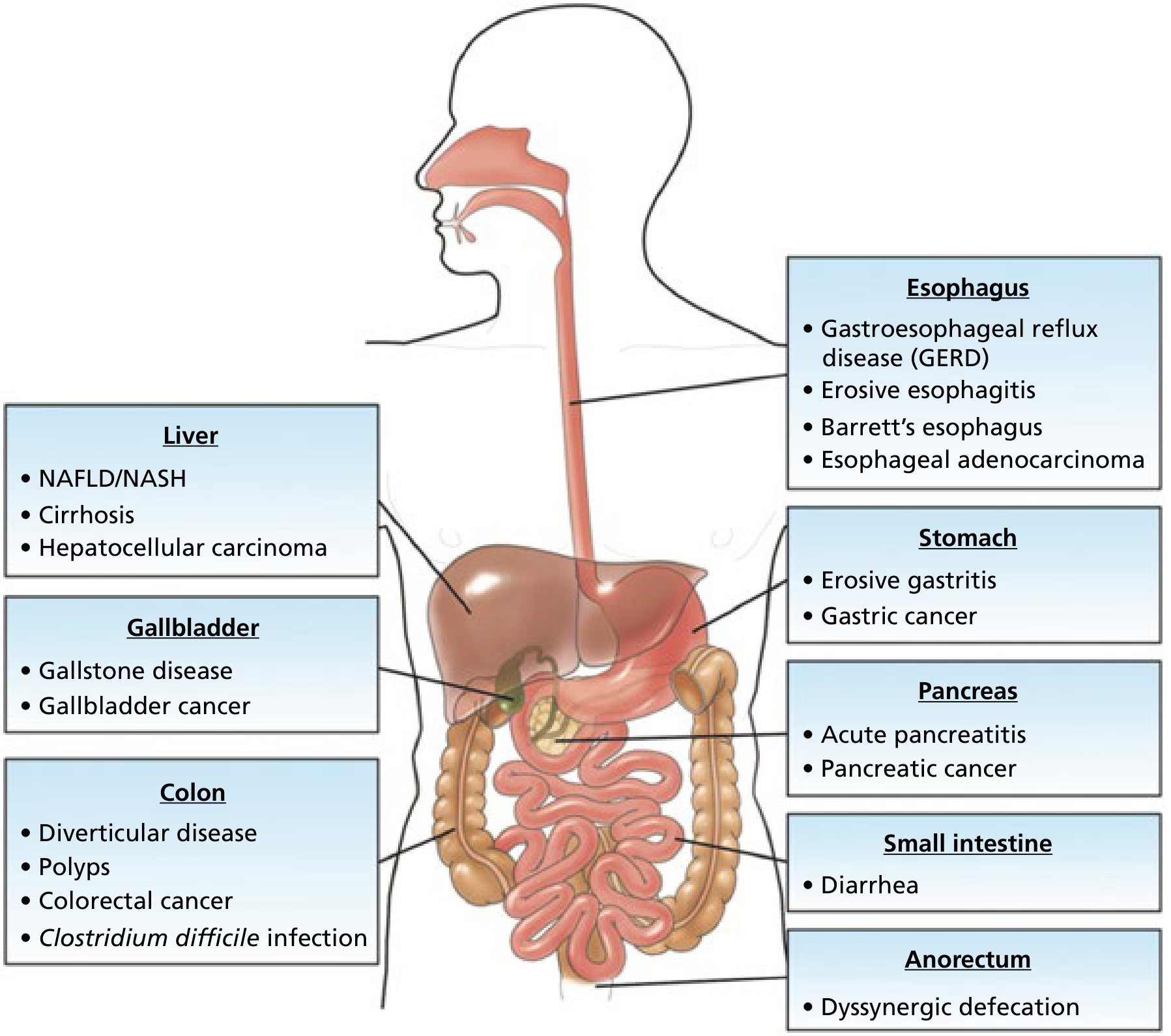
Here is a beautiful overview of obesity-related GI diseases from Yamada's Textbook - notice GERD sits right at the top of the esophageal disease list:
🔵 WHAT IS GERD?
GERD = Gastroesophageal Reflux Disease
It is a chronic condition where stomach acid (and sometimes bile) flows backward (refluxes) from the stomach into the esophagus, causing irritation and damage to the esophageal lining.
Ayurvedic Parallel (for your BAMS background): GERD correlates closely with Amlapitta in Ayurveda - the condition of excess/vitiated Pitta in Amashaya (stomach) with urdhvaga (upward movement) pattern. The Ushna, Tikshna, Amla qualities of Pitta producing daha (burning) in Uras (chest) is your existing reference point.
Prevalence:
- Affects ~20% of adults in Western countries
- Affects ~8-15% in Asia (but rapidly rising with urbanization and obesity)
- One of the top 3 reasons people visit a gastroenterologist
🔵 NORMAL ANATOMY - What PREVENTS Reflux?
Before understanding GERD, understand the normal defense:
MOUTH
↓ (swallowing)
ESOPHAGUS (25 cm pipe - NO acid here normally)
↓
[LOWER ESOPHAGEAL SPHINCTER = LES] ← THE GATEKEEPER
↓ (one-way valve - opens only to let food down)
STOMACH (full of HCl acid, pH 1.5-3.5)
The LES (Lower Esophageal Sphincter) is the key structure. It is:
- A thick ring of circular smooth muscle at the bottom of the esophagus
- Normally closed (resting pressure 15-30 mmHg) - keeps acid IN the stomach
- Opens briefly when you swallow to let food into stomach
- Supported by diaphragmatic crura (external LES) and the phreno-esophageal ligament
Three things protect against reflux:
- High LES resting pressure (15-30 mmHg)
- Adequate LES length (at least 2 cm must be inside the abdomen)
- Normal angle of His (sharp angle between esophagus and stomach)
🔵 PATHOPHYSIOLOGY - Why Does Reflux Happen?
(Source: Fischer's Mastery of Surgery 8th Ed)
GERD develops when this protective LES mechanism fails. There are 3 main mechanisms:
Mechanism 1 - Transient LES Relaxations (tLESRs) ← MOST COMMON
- The LES relaxes at the wrong time - NOT during swallowing
- These are reflex relaxations triggered by gastric distension
- Account for ~80% of all reflux episodes in GERD patients
- This is the main mechanism in mild to moderate GERD
Mechanism 2 - Low Resting LES Pressure
- The sphincter is simply too weak
- Pressure drops below 6 mmHg (normal = 15-30 mmHg)
- Causes continuous reflux, especially when lying flat
- Seen in severe GERD and scleroderma patients
Mechanism 3 - Hiatal Hernia
- The upper part of the stomach slides above the diaphragm into the chest
- This disrupts both the LES and the diaphragmatic crura (external sphincter)
- The diaphragm no longer helps squeeze the LES shut
- Seen in most patients with severe GERD and Barrett's esophagus
Additional Contributing Factors:
| Factor | How It Causes GERD |
|---|---|
| Obesity | High intraabdominal pressure pushes acid upward |
| Pregnancy | Progesterone relaxes LES + enlarging uterus increases abdominal pressure |
| Smoking | Nicotine directly reduces LES tone |
| Alcohol | Relaxes LES, increases acid secretion |
| High-fat meals | Delays gastric emptying, distends stomach |
| Caffeine, chocolate, mint | Reduce LES pressure |
| NSAIDs | Directly damage esophageal mucosa |
| Lying down after meals | Gravity no longer helps keep acid down |
🔵 WHY DOES ACID DAMAGE THE ESOPHAGUS?
The stomach is designed for acid - it has a thick mucus layer protecting its lining.
The esophagus has NO such protection. Its squamous epithelium is very sensitive to acid.
When acid refluxes:
- pH of esophagus drops from normal (6-7) to below 4
- Acid + pepsin together cause mucosal injury
- Repeated exposure → inflammation → erosions → ulcers → scarring
- Long-term repeated injury → Barrett's Esophagus (pre-cancerous change)
🔵 SYMPTOMS OF GERD
Typical (Esophageal) Symptoms:
| Symptom | Description | Key Point |
|---|---|---|
| Heartburn (Pyrosis) | Burning sensation behind the sternum (breastbone) | Worsens after meals, lying down, bending forward |
| Regurgitation | Sour/bitter liquid coming up into mouth or throat | Patient says "acid taste in mouth" |
| Water Brash | Sudden flood of saliva in mouth | Reflex hypersalivation to neutralize acid |
| Dysphagia | Difficulty swallowing | Alarm symptom - suggests stricture or cancer |
| Odynophagia | Pain on swallowing | Suggests severe esophagitis or ulcer |
Atypical (Extra-Esophageal) Symptoms:
These are tricky - GERD can MIMIC other diseases!
| Symptom | Explanation |
|---|---|
| Chronic cough | Acid microaspiration irritates airways |
| Asthma / wheezing | Acid triggers bronchospasm via vagal reflex |
| Hoarseness / voice change | Acid damages vocal cords (laryngopharyngeal reflux) |
| Chronic sore throat | Acid irritates pharynx |
| Dental erosions | Acid destroys tooth enamel |
| Non-cardiac chest pain | GERD mimics heart attack! |
| Sinusitis / ear problems | In some patients |
Clinical Pearl: When a patient comes with "heart attack-like" chest pain and the cardiac workup is negative - always think GERD! GERD is one of the top causes of non-cardiac chest pain.
🔵 ALARM SYMPTOMS - Red Flags (URGENT Investigation Needed!)
If a GERD patient has ANY of these, they need immediate endoscopy:
- 🚨 Dysphagia (difficulty swallowing) - may mean stricture or cancer
- 🚨 Odynophagia (painful swallowing)
- 🚨 Unexplained weight loss
- 🚨 Hematemesis (vomiting blood)
- 🚨 Melena (black tarry stools)
- 🚨 Anemia (iron deficiency)
- 🚨 Age >50 with new onset symptoms
- 🚨 Symptoms not responding to treatment
🔵 COMPLICATIONS OF GERD
This is the GERD → Barrett's → Cancer progression - the most important chain in GI medicine:
NORMAL ESOPHAGUS
↓ (repeated acid injury over years)
REFLUX ESOPHAGITIS (Grade A-D)
↓ (continued injury)
PEPTIC STRICTURE (scarring narrows the esophagus → dysphagia)
↓ (in some patients with severe long-standing GERD)
BARRETT'S ESOPHAGUS ← PRE-CANCEROUS CHANGE
↓ (in ~0.5% per year)
ESOPHAGEAL ADENOCARCINOMA ← CANCER
Complication 1 - Reflux Esophagitis
- Graded by the Los Angeles Classification (LA Grade A-D):
| Grade | Finding |
|---|---|
| Grade A | Mucosal breaks < 5 mm, not continuous between folds |
| Grade B | Mucosal breaks > 5 mm, not continuous between folds |
| Grade C | Mucosal breaks continuous between folds, < 75% circumference |
| Grade D | Mucosal breaks involving > 75% of esophageal circumference |
Complication 2 - Peptic Stricture
- Repeated inflammation → fibrosis and narrowing
- Patient presents with progressive dysphagia (first to solids, then liquids)
- Treatment: endoscopic dilation + PPIs
Complication 3 - Barrett's Esophagus ← MOST IMPORTANT COMPLICATION
(Source: Goldman-Cecil Medicine)
- Definition: Normal squamous epithelium of the distal esophagus is replaced by columnar epithelium (intestinal metaplasia with goblet cells)
- This is called metaplasia - one type of cell replacing another
- Affects 5-15% of patients who undergo endoscopy for GERD symptoms
- Risk factors: Long-standing GERD, obesity, male sex, white race, smoking, age >50
- Importance: Barrett's is a pre-malignant condition - it can progress to esophageal adenocarcinoma
- Annual cancer risk from Barrett's: ~0.5% per year (low in any single year, but significant over a lifetime)
- Surveillance: Regular endoscopy + biopsy every 3-5 years (or more frequently if dysplasia found)
Key Histology: You look for goblet cells on biopsy - their presence confirms intestinal metaplasia = Barrett's esophagus
🔵 DIAGNOSIS OF GERD
(Source: Harrison's Principles of Internal Medicine 22E)
Step 1 - Clinical Diagnosis (Most common approach)
- Classic heartburn + regurgitation = GERD diagnosis can be made clinically
- PPI trial: Give a proton pump inhibitor for 4-8 weeks
- If symptoms improve significantly → confirms GERD (therapeutic trial)
- This is the standard first approach in typical cases without alarm symptoms
Step 2 - Investigations (When needed)
| Investigation | What It Shows | When Used |
|---|---|---|
| Upper GI Endoscopy (OGD) | Esophagitis grading, Barrett's, ulcers, strictures | Alarm symptoms, treatment failure, surveillance |
| 24-hour pH monitoring | Most sensitive test - measures how often acid drops below pH 4 | When diagnosis uncertain, before surgery |
| pH-Impedance monitoring | Detects both acid AND non-acid reflux | Best for complete reflux assessment |
| Esophageal Manometry | Measures LES pressure and esophageal motility | Before anti-reflux surgery |
| Barium Swallow | Shows strictures, hiatal hernia | Less used now |
Key Exam Fact: The most sensitive test for GERD diagnosis = 24-hour ambulatory pH + impedance monitoring - Harrison's 22E
🔵 TREATMENT OF GERD
Treatment is stepwise - start conservative, escalate if needed.
Step 1 - Lifestyle Modifications (Always first!)
| Modification | Reason |
|---|---|
| Lose weight | Reduces intraabdominal pressure |
| Elevate head of bed by 6-8 inches | Uses gravity to prevent nighttime reflux |
| Don't lie down for 3 hours after meals | Keeps acid in stomach while digesting |
| Avoid trigger foods: fatty food, chocolate, mint, coffee, alcohol, citrus, tomato | All reduce LES pressure or irritate directly |
| Small, frequent meals | Prevents excessive gastric distension |
| Stop smoking | Nicotine relaxes LES |
| Avoid tight clothing | Reduces abdominal pressure |
Step 2 - Antacids (For mild, occasional symptoms)
- Examples: Aluminum hydroxide, Magnesium hydroxide, Calcium carbonate (Tums)
- Mechanism: Neutralize acid already in stomach (don't reduce acid production)
- Onset: Fast (minutes) but short-lasting (30-60 min)
- Use: On-demand for mild heartburn
Step 3 - H2 Blockers (Moderate symptoms)
- Examples: Ranitidine (withdrawn due to NDMA), Famotidine, Cimetidine
- Mechanism: Block H2 receptors on parietal cells → reduce acid secretion
- Reduce acid by ~70%
- Problem: Tolerance develops (tachyphylaxis) with regular use
Step 4 - Proton Pump Inhibitors (PPIs) - THE GOLD STANDARD
- Examples: Omeprazole, Pantoprazole, Rabeprazole, Lansoprazole, Esomeprazole
- Mechanism: Irreversibly block H+/K+ ATPase pump (the final step in acid production) on parietal cells
- Reduce acid by >90% - most powerful acid suppressants available
- Taken 30-60 minutes before meals (so drug reaches parietal cells while they are being activated by food)
- Duration: 4-8 weeks for esophagitis; long-term for Barrett's and severe GERD
- Side effects (long-term): Hypomagnesemia, B12 deficiency, increased infection risk, osteoporosis
Mnemonic for PPIs: "Omeprazole Pantoprazole Rabeprazole Lansoprazole Esomeprazole" = OPRLE or just remember they all end in "-prazole"
Step 5 - Prokinetics (Adjunct therapy)
- Examples: Metoclopramide, Domperidone
- Mechanism: Increase LES pressure + speed up gastric emptying
- Reduce gastric distension - less reflux trigger
- Limited long-term use due to side effects (extrapyramidal effects with metoclopramide)
Step 6 - Anti-Reflux Surgery (When all else fails)
- Nissen Fundoplication - the stomach fundus is wrapped 360° around the lower esophagus to mechanically strengthen the LES
- Indicated when: Young patient who doesn't want lifelong PPIs, large hiatal hernia, symptoms persist despite max medical therapy
- LINX procedure: A magnetic ring placed around the LES to reinforce it (newer, reversible option)
🔵 GERD IN SPECIAL SITUATIONS
| Situation | Key Points |
|---|---|
| Pregnancy | Use antacids/alginate first; PPIs generally safe but use cautiously |
| Children/Infants | Very common in infants (immature LES); usually resolves by age 1; lifestyle first |
| Elderly | Often present atypically (no heartburn!); present with silent esophagitis, anemia |
| Asthma patients | GERD worsens asthma; treat GERD to improve asthma control |
🔵 CLINICAL CASE (Practice Your Thinking!)
Patient: 45-year-old man, desk job, BMI 32 (obese), smoker. Comes to you with:
- Burning sensation in chest after meals for 2 years
- Worse when lying down at night
- Sour taste in mouth in the mornings
- Occasional dry cough
- No weight loss, no difficulty swallowing, no blood in stools
Questions:
- What is your diagnosis?
- What alarm symptoms are ABSENT here?
- What will you do first - investigate or treat?
- What medication and what advice will you give?
- What complication is this patient at risk of developing?
(Try to answer before reading below)
Answers:
- GERD - classic presentation (heartburn, regurgitation, nocturnal symptoms, cough)
- No dysphagia, no weight loss, no bleeding, no anemia - absence of alarm symptoms means no urgent endoscopy needed
- Treat empirically first - PPI trial for 4-8 weeks (no need for immediate endoscopy since no alarm symptoms)
- Omeprazole 20 mg once daily, 30 min before breakfast + Lifestyle: lose weight, elevate head of bed, stop smoking, avoid late meals, reduce fatty food
- Barrett's Esophagus - he is a middle-aged obese male smoker with long-standing GERD = high-risk profile
✅ Lesson 2 Summary - Key Points to Never Forget
| # | Key Point |
|---|---|
| 1 | GERD = failure of the LES (Lower Esophageal Sphincter) |
| 2 | Most common mechanism = transient LES relaxations (tLESRs) |
| 3 | Hiatal hernia is the main structural cause |
| 4 | Typical symptoms = heartburn + regurgitation |
| 5 | Atypical symptoms = cough, hoarseness, asthma, chest pain |
| 6 | Alarm symptoms = refer for urgent endoscopy |
| 7 | Most sensitive test = 24-hour pH-impedance monitoring |
| 8 | Gold standard treatment = PPIs ("-prazole" drugs) |
| 9 | GERD → Barrett's Esophagus → Esophageal Adenocarcinoma |
| 10 | Barrett's = squamous → columnar metaplasia (goblet cells on biopsy) |
🎯 Coming Up in Lesson 3
Peptic Ulcer Disease (PUD) - the disease that changed all of medicine when we discovered bacteria (H. pylori) cause ulcers:
- Why stomach acid eats through its own wall
- H. pylori - the Nobel Prize-winning discovery
- How to diagnose and eradicate H. pylori
- Complications: perforation, bleeding, obstruction
- All the drugs used to treat it
Reply "Next" for Lesson 3, or ask me any question about GERD before we move on! 🚀
Sources: Fischer's Mastery of Surgery 8th Ed | Goldman-Cecil Medicine | Yamada's Textbook of Gastroenterology 7E | Harrison's Principles of Internal Medicine 22E (2025)
You did great Lekin mujhe ye sb Hinglish me chahiye aur clinical cases chahiye achche achche se 3 kam se kam aur bs jo main aur important points h gastroenterologist ke loye vohi details jo jyada mt do aur Is baar make it best aur treatment lifestyle diet ye sb bhi achche se smjhao
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Perfect - textbook se live content aur actual endoscopy image bhi mil gayi. Ab tumhare liye best Hinglish lesson likhta hoon!
🔥 LESSON 2 - GERD (Acid Reflux Disease)
Hinglish mein - Maximum Clarity, Minimum Bakwaas
🎯 EK LINE MEIN GERD KYA HAI?
"Stomach ka acid wapas esophagus mein aana - aur esophagus ko jalana - yahi GERD hai."
Simple sa concept hai, lekin iska cascade of complications bahut dangerous hai. Isi liye gastroenterologist ke liye GERD ek foundation disease hai.
🔑 MOST IMPORTANT CONCEPT - LES (Lower Esophageal Sphincter)
Ek darwaza imagine karo esophagus aur stomach ke beech mein - yahi LES hai.
ESOPHAGUS (food pipe - koi acid nahi hota yahan)
↓
[LES] ← YE DARWAZA HAI
↓
STOMACH (acid factory - pH 1.5 to 3.5)
Normal mein: LES band rehta hai - acid upar nahi aata.
GERD mein: LES kaam nahi karta properly - acid upar aata hai - esophagus jalti hai.
LES kyun fail hota hai? (3 main reasons)
| Reason | Kya hota hai | Kahan zyada |
|---|---|---|
| Transient LES relaxations | LES galat time pe khul jaata hai | 80% cases - most common |
| Weak LES pressure | Pressure <6 mmHg ho jaata hai (normal 15-30) | Severe GERD |
| Hiatal Hernia | Stomach ka part diaphragm ke upar aa jaata hai - LES support khatam | Barrett's risk high |
⚡ RISK FACTORS - "Ye log GERD ke liye bane hain"
| Risk Factor | Reason |
|---|---|
| Obesity | Pet mein pressure badh jaata hai, acid upar dhakelta hai |
| Pregnancy | Progesterone LES relax karta hai + uterus pressure deta hai |
| Smoking | Nicotine directly LES tone kam karta hai |
| Alcohol | LES relax + acid secretion increase |
| Fatty food, chocolate, mint, coffee | Sab LES pressure reduce karte hain |
| Late night khana | Lete waqt gravity help nahi karta |
| Tight clothes | Abdominal pressure increase |
| NSAIDs (aspirin, ibuprofen) | Directly esophageal mucosa damage karte hain |
🩺 SYMPTOMS - Kaise Pehchanein GERD?
Typical Symptoms (Classic GERD):
| Symptom | Hindi mein | Key point |
|---|---|---|
| Heartburn / Pyrosis | Seene mein jalan | Khane ke baad worse, raat ko worse |
| Regurgitation | Khatta/kadwa taste aana | "Muh mein acid aa jaata hai" |
| Water Brash | Muh mein suddenly paani bhar jaata hai | Saliva reflex - acid neutralize karne ke liye |
Atypical Symptoms (Confusing - GERD dusri bimari jaise lagta hai!):
| Symptom | Explanation |
|---|---|
| Chronic cough | Acid microaspiration se airway irritate hoti hai |
| Hoarseness / voice change | Acid vocal cords tak pahunch jaata hai |
| Asthma jaise symptoms | Vagal reflex se bronchospasm hota hai |
| Non-cardiac chest pain | GERD heart attack jaisa feel kara sakta hai! |
| Dental erosions | Acid daant gala deta hai |
🔴 Clinical Pearl: Jab patient aaye chest pain se aur cardiac workup normal ho - always think GERD! Ye ek top GI trap hai boards mein bhi.
🚨 ALARM SYMPTOMS - Ye Dekho Toh Seedha Endoscopy!
Ye signs dikh jaayein toh PPI trial mat karo - seedha endoscopy karo:
- 🚩 Dysphagia (nigalne mein takleef) - stricture ya cancer?
- 🚩 Unexplained weight loss
- 🚩 Hematemesis (khoon ki ulti)
- 🚩 Melena (kaala poth jaisa stool)
- 🚩 Anemia (iron deficiency)
- 🚩 Age >50 mein naye symptoms
- 🚩 4-8 weeks PPI ke baad bhi symptoms - response nahi
Mnemonic: "ABCDE" - Anemia, Bleeding, Chest pain persists, Dysphagia, Emesis (vomiting) + weight loss = Endoscopy karo!
⚠️ COMPLICATIONS - GERD Ka Dangerous Safar
NORMAL ESOPHAGUS
↓ (months-years of acid exposure)
REFLUX ESOPHAGITIS (Grade A → B → C → D)
↓
PEPTIC STRICTURE (scarring → narrowing → dysphagia)
↓
BARRETT'S ESOPHAGUS ← DANGER ZONE
↓ (0.5% per year)
ESOPHAGEAL ADENOCARCINOMA
Barrett's Esophagus - Samjho Achi Tarah
- Normal esophagus mein squamous cells hote hain (flat cells)
- Repeated acid injury ke baad ye cells columnar cells (goblet cells) mein badal jaate hain
- Yahi metaplasia hai - ek cell type dusre mein replace hona
- Ye change pre-cancerous hai
- Endoscopy pe kaisa dikhta hai? - Salmon-pink coloured mucosa normal white mucosa ki jagah
Yahan dekho - actual endoscopy image of Barrett's Esophagus:
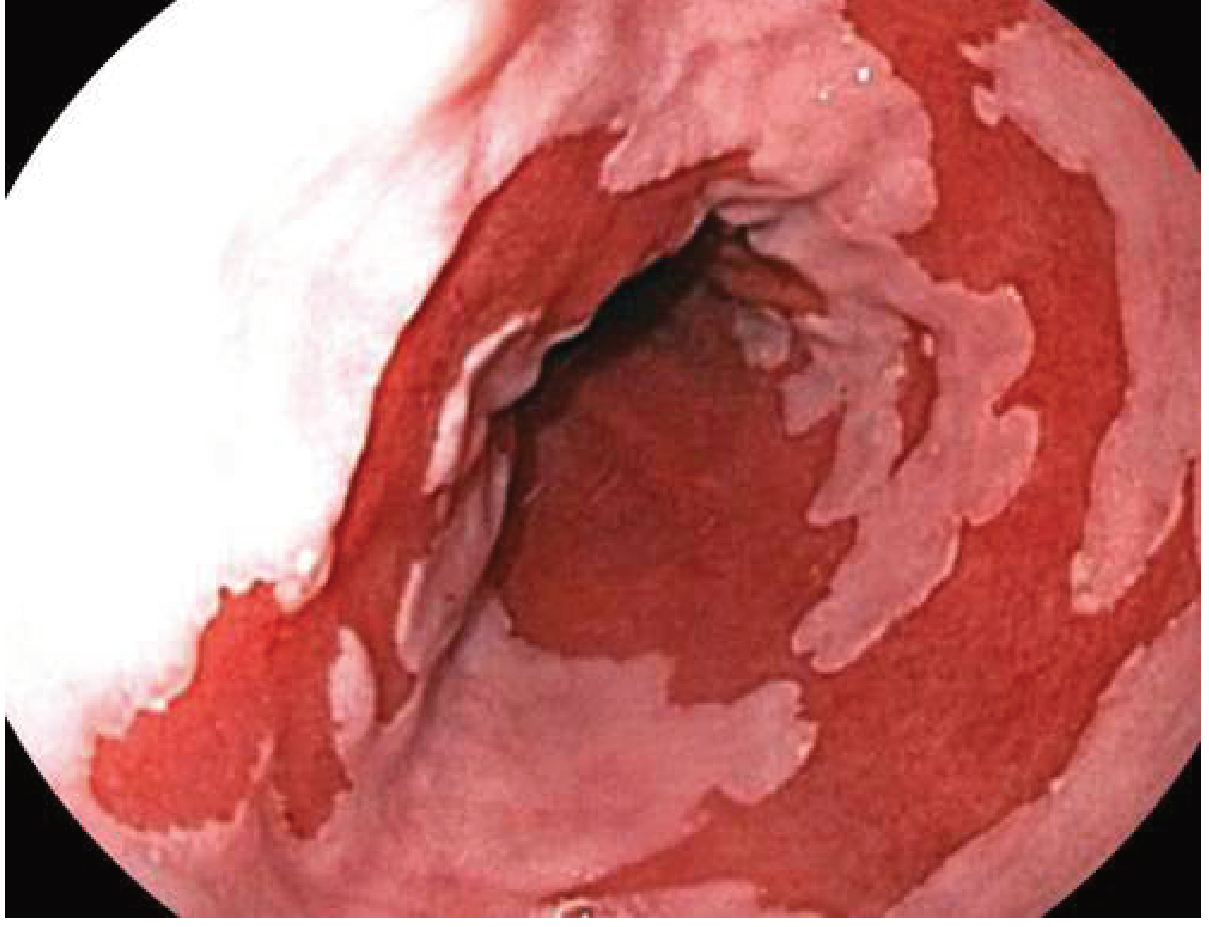
Endoscopy mein dekho - upar white squamous mucosa hai, neeche salmon-pink Barrett's mucosa. Yahi squamocolumnar junction ka displacement hai. (Goldman-Cecil Medicine)
🔬 DIAGNOSIS - Kaise Confirm Karte Hain?
| Test | Kya batata hai | Kab karte hain |
|---|---|---|
| Clinical + PPI Trial | Symptoms + 4-8 wk PPI response | First step - typical symptoms, no alarm |
| Upper GI Endoscopy (OGD) | Esophagitis grade, Barrett's, stricture | Alarm symptoms, treatment failure |
| 24-hr pH + Impedance monitoring | Most sensitive test - actual acid exposure measure karta hai | Diagnosis doubtful, pre-surgery |
| Esophageal Manometry | LES pressure, motility | Anti-reflux surgery se pehle |
| Barium Swallow | Stricture, hiatal hernia | Limited use ab |
(Harrison's 22E: "Most sensitive test for GERD = 24-hour ambulatory pH and impedance monitoring")
💊 TREATMENT - Step by Step
🥗 STEP 1 - LIFESTYLE + DIET (Sabse Pehle Yahi!)
Ye changes genuinely kaam karte hain - sirf advice mat do, explain karo kyon:
KHAANA:
| ✅ Khao | ❌ Bilkul Avoid Karo |
|---|---|
| Daliya, oats, banana, apple | Fried/oily food - LES relax karta hai |
| Lean protein (chicken, fish, dal) | Chocolate - LES tone kam karta hai |
| Green vegetables | Mint/peppermint - LES relax karta hai |
| Low-fat dairy | Coffee/tea zyada - acid production increase |
| Whole grains | Alcohol - dual effect (LES + acid) |
| Ginger (anti-inflammatory) | Citrus fruits, tomatoes - directly irritate |
| Coconut water | Carbonated drinks - gas se pressure |
| Curd/yogurt (thodi matra) | Spicy masaledaar food |
LIFESTYLE RULES:
| Rule | Reason |
|---|---|
| Khane ke 3 ghante baad leto | Gravity se acid neeche rehta hai |
| Bed ka head end 15-20 cm utha do | Raat ko gravity help karta hai |
| Chhoti chhoti meals lena, 5-6 baar | Stomach zyada distend na ho |
| Weight loss | Abdominal pressure kam hota hai - GERD dramatically better |
| Smoking band karo | Nicotine ka LES pe direct effect |
| Tight belt/clothing avoid karo | Abdominal pressure kam karo |
| Stress management karo | Stress gastric acid secretion badhata hai |
💊 STEP 2 - MEDICATIONS (Ladder Approach)
Mild symptoms → ANTACIDS
↓ (if not enough)
Moderate → H2 BLOCKERS
↓ (gold standard)
Standard/Severe → PPIs ← CORNERSTONE OF TREATMENT
↓ (adjunct)
Prokinetics → METOCLOPRAMIDE (limited use)
↓ (surgery last resort)
NISSEN FUNDOPLICATION
🔵 ANTACIDS
- Examples: Gelusil, Digene, Eno, Milk of Magnesia
- Mechanism: Acid ko neutralize karte hain (production nahi rokate)
- Onset: 5-10 minutes - bahut fast
- Duration: 30-60 minutes only
- Use: Kabhi kabhi heartburn ke liye - on-demand
- Dose: 15 mL after meals and at bedtime
🔵 H2 BLOCKERS (H2 Receptor Antagonists)
- Examples: Famotidine (most common), Cimetidine, Ranitidine (withdrawn)
- Mechanism: Parietal cells pe H2 receptor block karo → acid secretion ~70% kam
- Problem: Tachyphylaxis - regular use se effectiveness kam hoti hai
- Use: Mild-moderate GERD, nighttime acid breakthrough
🔴 PPIs - PROTON PUMP INHIBITORS ← KING OF GERD TREATMENT
- Examples: Omeprazole 20mg, Pantoprazole 40mg, Rabeprazole 20mg, Lansoprazole 30mg, Esomeprazole 40mg
- Mechanism: H+/K+ ATPase pump (proton pump) ko irreversibly block karta hai - yahi acid banane ki final step hai
- Acid reduction: >90% - sabse powerful
- Timing: Khane se 30-60 min pehle - issi waqt parietal cells activate hote hain
- Duration: 4-8 weeks esophagitis ke liye; long-term Barrett's ke liye
Long-term PPI side effects (important for exams!):
- Vitamin B12 deficiency
- Hypomagnesemia
- C. difficile infection risk
- Osteoporosis / hip fracture risk
- SIBO (small intestinal bacterial overgrowth)
🔵 SURGERY - Nissen Fundoplication
- Kab: Young patient, surgery prefer karta ho; large hiatal hernia; PPIs se symptoms nahi jaate
- Kya hota hai: Stomach ka fundus esophagus ke around 360° wrap kar dete hain - mechanical LES banana
- New option: LINX device - magnetic ring LES ke around lagaate hain
🏥 CLINICAL CASES - 3 Real-World Scenarios
🟢 CASE 1 - The Classic Presentation
Patient: Ramesh, 42 saal, IT professional, BMI 29, smoker
Complaint: 18 mahine se seene mein jalan - dinner ke baad worse, raat ko zyada, subah uthke muh mein khatta taste
Tumhara approach:
Q1: Diagnosis kya hai?
→ GERD - classic symptoms (heartburn + regurgitation + nocturnal worsening)
Q2: Koi investigation zaroor hai abhi?
→ Nahi! Alarm symptoms absent hain - koi dysphagia, weight loss, bleeding nahi
→ Clinical diagnosis sufficient hai
Q3: Treatment kya doge?
→ Lifestyle: Weight kam karo, smoking band karo, late dinner avoid karo, bed elevate karo
→ Diet: Oily food, coffee, alcohol, mint avoid karo
→ Medication: Tab. Pantoprazole 40mg - khane se 30 min pehle - 8 weeks
Q4: 8 weeks baad kya?
→ Agar symptoms gaaye - PPI taper ya stop karo
→ Agar symptoms wapas aaye - low-dose maintenance PPI consider karo
→ Agar symptoms remain despite PPI - endoscopy karo!
Q5: Is patient ko Barrett's ka risk hai?
→ Haan - middle-aged male, smoker, long-standing GERD = high risk
→ Agar 10+ saal ka history ho - screening endoscopy recommend karo
🔴 CASE 2 - The Alarm Symptom Case
Patient: Savita, 55 saal, housewife. 5 saal se "acidity" ki problem thi - khud se antacid le rahi thi. Ab 3 mahine se khana nigalne mein takleef ho rahi hai. 4 kg weight kaam hua hai.
Tumhara approach:
Q1: Ab kya karo?
→ ALARM SYMPTOMS present hain - dysphagia + weight loss
→ PPI trial mat karo - seedha urgent endoscopy (OGD)
Q2: Endoscopy mein kya milega?
→ Possible findings:
- Peptic stricture (scarring se narrowing - benign)
- Barrett's esophagus with dysplasia
- Esophageal adenocarcinoma (cancer - worst case)
Q3: Endoscopy mein peptic stricture mili - kya karoge?
→ Endoscopic dilation - stricture ko balloon se stretch karo
→ PPI start karo - long-term
→ Regular follow-up
Q4: Endoscopy mein Barrett's with high-grade dysplasia mili - kya karoge?
→ Radiofrequency Ablation (RFA) - abnormal tissue ko burn karo
→ Ya Endoscopic Mucosal Resection (EMR)
→ Regular surveillance endoscopy - every 3-6 months
Lesson: Ye case batata hai ki GERD ko "sirf acidity" samajhke ignore nahi karte! Years of untreated GERD → dangerous consequences.
🟡 CASE 3 - The Tricky Atypical Presentation
Patient: Suresh, 38 saal, teacher, non-smoker. 6 mahine se chronic cough hai. Pulmonologist ke paas gaya - chest X-ray normal, spirometry normal, asthma ka treatment diya - koi fark nahi. ENT doctor bola - throat thoda red hai, "post-nasal drip" diagnose ki.
- No heartburn (patient specifically bolta hai - "seene mein jalan nahi hoti")
- Subah uthke thodi hoarseness hoti hai
- Raat ko khana khane ke baad kuch ghante baad theek se so nahi pata
Q1: Kya soch rahe ho?
→ GERD with atypical/extraesophageal presentation - specifically Laryngopharyngeal Reflux (LPR)
→ Ye patients aksar heartburn nahi feel karte - "Silent GERD"
Q2: Ye kaise possible hai bina heartburn ke?
→ Acid throat/larynx tak aata hai - esophagus sensitize nahi hoti, isliye burning feel nahi
→ Lekin vocal cords + airway irritate hote hain
→ Chronic cough + hoarseness in GERD = LPR (Laryngopharyngeal Reflux)
Q3: Diagnosis confirm kaise karo?
→ 24-hr pH + impedance monitoring - upright position mein bhi reflux dikhega
→ Ya empiric PPI trial (8-12 weeks) - agar cough better ho → confirms LPR/GERD
Q4: Treatment?
→ PPIs - twice daily (LPR ko once daily se zyada dose chahiye hoti hai)
→ Lifestyle changes - especially late meals avoid karo
→ ENT + GI coordination
Lesson: GERD = sirf heartburn nahi! Chronic cough, hoarseness, asthma-like symptoms - sab GERD ho sakta hai. Ye trap bahut boards mein aata hai!
📊 GERD - Quick Revision Table (Exam Ready!)
| Topic | Key Point |
|---|---|
| Most common mechanism | Transient LES relaxations (tLESRs) |
| Most common structural cause | Hiatal Hernia |
| Most sensitive test | 24-hr pH + impedance monitoring |
| Gold standard diagnosis in routine | Clinical + PPI trial response |
| Endoscopy kab | Alarm symptoms ya treatment failure |
| Gold standard treatment | PPIs (omeprazole, pantoprazole) |
| Timing of PPI | Khane se 30-60 min pehle |
| Barrett's kya hai | Squamous → Columnar metaplasia (goblet cells) |
| Barrett's ka cancer risk | ~0.5% per year |
| Barrett's treatment | Radiofrequency Ablation (RFA) |
| Surgery | Nissen fundoplication |
| Atypical GERD | Cough, hoarseness, asthma, chest pain |
✅ Lesson 2 Complete!
3 cheezein jo kabhi nahi bhoolni:
- LES fail → GERD → Barrett's → Cancer - ye chain yaad rakho
- Alarm symptoms → Endoscopy seedha - PPI trial mat dena
- Heartburn nahi matlab GERD nahi - galat! Silent GERD hota hai
🎯 Lesson 3 Mein Aayega:
Peptic Ulcer Disease (PUD)
- H. pylori kya hai - Nobel Prize wali discovery
- Stomach apna aap kyun nahi khata (normally)?
- Ulcer kab khata hai - mechanism samjhenge
- Classic presentation + 3 clinical cases (Hinglish mein!)
- Complications: bleeding, perforation, obstruction
- H. pylori eradication regimens - exactly kaunsi drugs, kitni dose
"Next" likho aur Lesson 3 shuru hoga! 🚀
Sources: Goldman-Cecil Medicine | Harrison's Principles of Internal Medicine 22E | Yamada's Textbook of Gastroenterology 7E | Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.