Ecg full detail related all diseases also with proper diagram in different clanical ecg
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a complete, structured ECG guide covering all major diseases with clinical diagrams from Harrison's, Goldman-Cecil, Tintinalli's, and Costanzo Physiology textbooks.
ECG (Electrocardiogram) - Full Clinical Guide
PART 1: ECG BASICS - WAVES, INTERVALS & SEGMENTS
The Normal ECG Waveform

Fig. 4.17 - The electrocardiogram measured from lead II (Costanzo Physiology, 7th Ed.)
| Component | Represents | Normal Value |
|---|---|---|
| P wave | Atrial depolarization | Duration < 120 ms; amplitude < 2.5 mm |
| PR interval | AV conduction time (atria + AV node) | 120-200 ms (3-5 small squares) |
| QRS complex | Ventricular depolarization | Duration < 120 ms (3 small squares) |
| ST segment | Plateau of ventricular action potential | Isoelectric (flat at baseline) |
| T wave | Ventricular repolarization | Upright in I, II, V3-V6 |
| QT interval | Total ventricular depolarization + repolarization | Corrected QTc < 440 ms (men), < 460 ms (women) |
Normal 12-Lead ECG
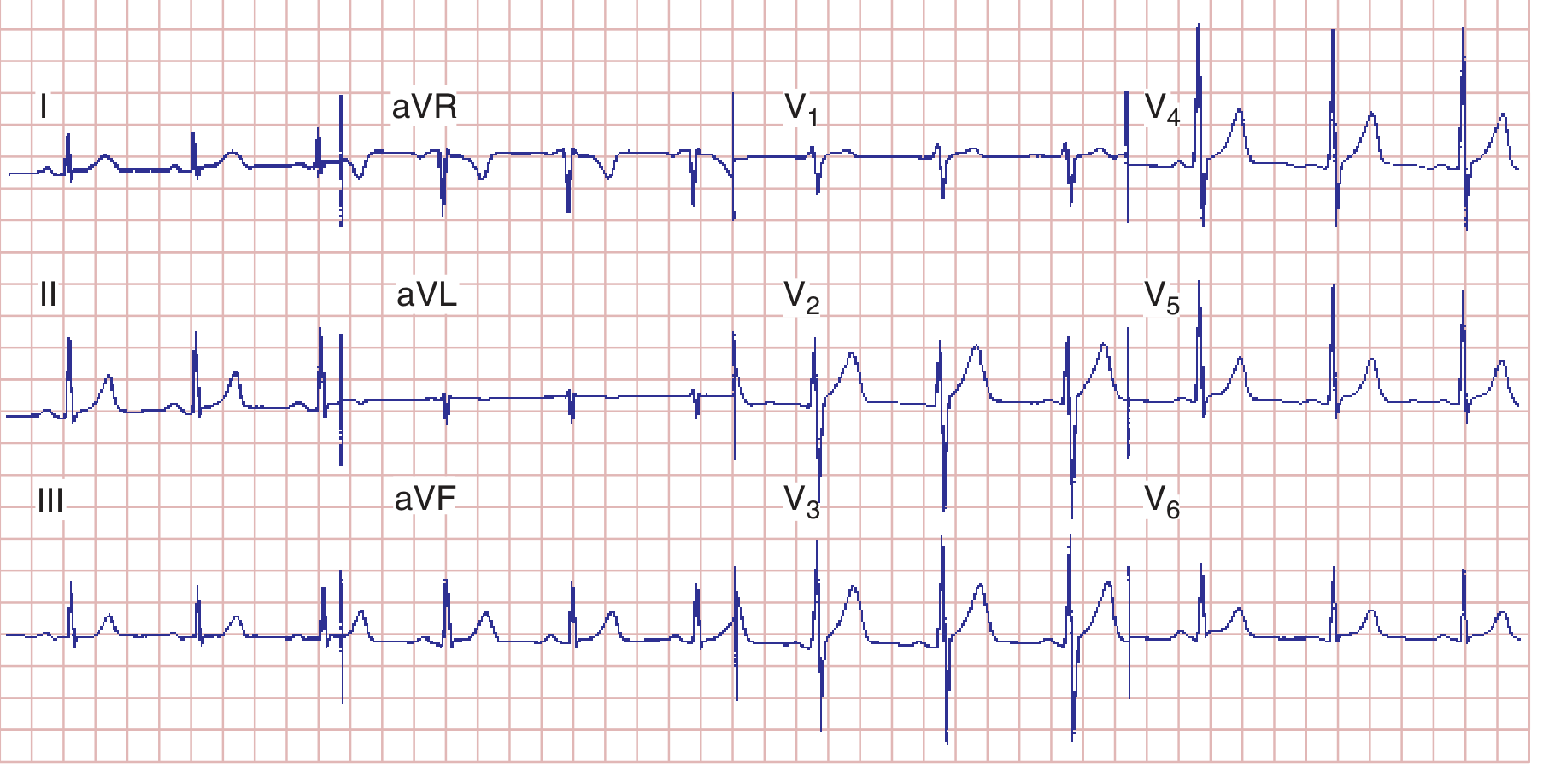
FIGURE 247-7 - Normal ECG, sinus rhythm, HR 75 bpm, PR 160 ms, QRS 80 ms, QTc ~390 ms (Harrison's Principles of Internal Medicine, 22e)
The 12 Leads - What They See
| Leads | Wall Viewed | Artery |
|---|---|---|
| II, III, aVF | Inferior wall | RCA |
| I, aVL, V5-V6 | Lateral wall | LCx |
| V1-V4 | Anterior wall | LAD |
| V1-V2 | Septal wall | LAD (septal branches) |
| V7-V9 (posterior) | Posterior wall | RCA / LCx |
| V3R-V6R | Right ventricle | RCA (proximal) |
PART 2: APPROACH TO ECG INTERPRETATION (SYSTEMATIC)
Always read ECGs in this order:
- Rate - count R-R intervals (300 / large squares between R waves)
- Rhythm - regular or irregular? P before every QRS?
- Axis - normal (0° to +90°); LAD (<0°); RAD (>+90°)
- P waves - present, morphology, relation to QRS
- PR interval - short/long/variable
- QRS duration - narrow (<120 ms) or wide (>120 ms)
- ST segment - elevation or depression
- T waves - peaked, inverted, flat
- QT interval - prolonged?
PART 3: ATRIAL ABNORMALITIES
Right Atrial Overload (RAO) / P Pulmonale
- Cause: COPD, pulmonary hypertension, tricuspid stenosis
- ECG: Tall, peaked P waves >2.5 mm in II, III, aVF ("P pulmonale")
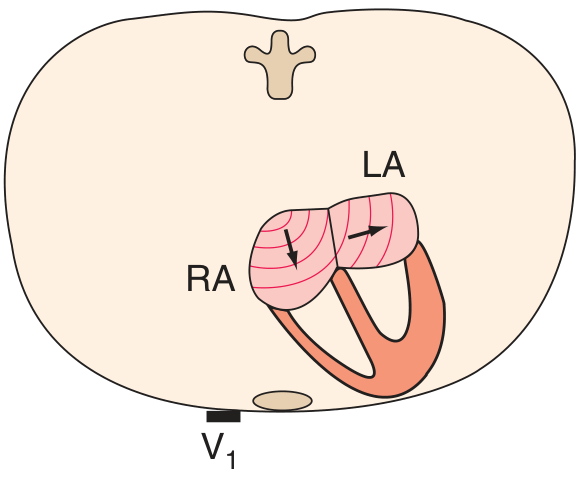
- V1: Large positive component of P wave
Left Atrial Abnormality (LAA) / P Mitrale
- Cause: Mitral stenosis, LV failure
- ECG: Broad notched P wave >120 ms in limb leads; biphasic P in V1 with prominent negative (terminal) component
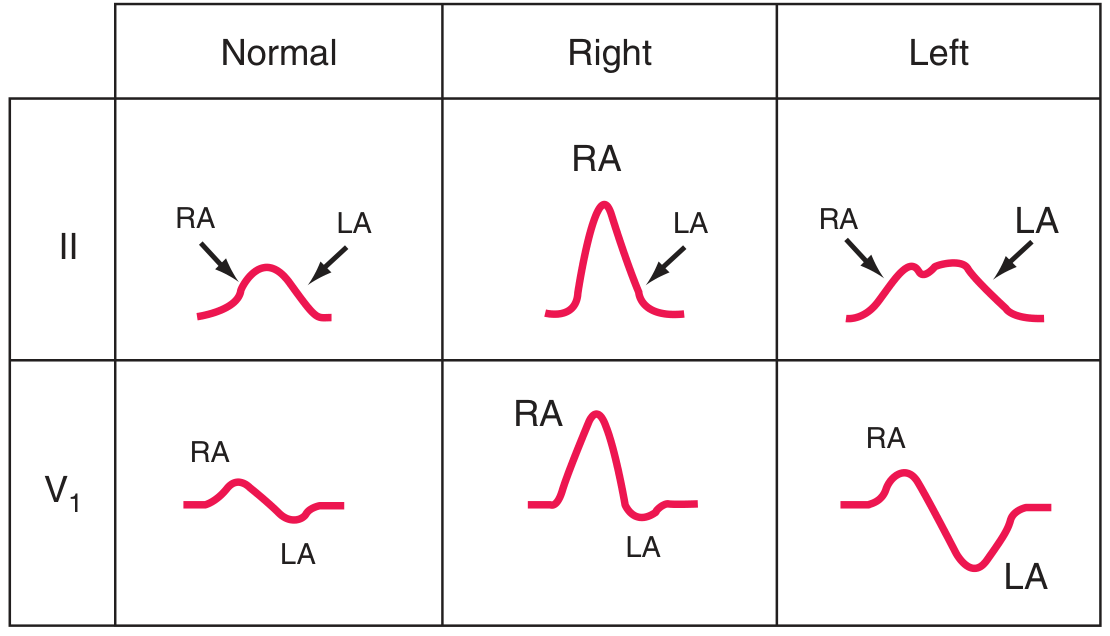
FIGURE 247-8 - Right atrial overload causes tall peaked P waves; left atrial abnormality causes broad notched P waves and biphasic P in V1. (Harrison's Principles of Internal Medicine, 22e)
PART 4: VENTRICULAR HYPERTROPHY
Left Ventricular Hypertrophy (LVH)
- Cause: Hypertension (most common), aortic stenosis, HCM
- ECG criteria (Sokolow-Lyon): S in V1 + R in V5 or V6 > 35 mm
- Cornell criterion: R in aVL + S in V3 > 28 mm (men), >20 mm (women)
- Associated findings: ST depression + T-wave inversion in lateral leads (V5-V6, I, aVL) = "LV strain pattern"
- Sensitivity: 30-50%; Specificity: 85-95%
Right Ventricular Hypertrophy (RVH)
- Cause: Pulmonary hypertension, pulmonary stenosis, cor pulmonale
- ECG: Tall R wave in V1 (R > S), right axis deviation >+90°
- Associated: T-wave inversions in V1-V3; prominent S waves in V5-V6

FIGURE 247-9 - LVH shifts electrical forces to the left and posteriorly (tall R in V6, deep S in V1). RVH shifts QRS vector rightward (tall R in V1, deep S in V6). (Harrison's Principles of Internal Medicine, 22e)
PART 5: CONDUCTION SYSTEM DISEASES
AV Blocks
First-Degree AV Block
- PR interval > 200 ms (>1 large square)
- Every P wave conducts - just slowly
- Causes: Inferior MI, digitalis toxicity, increased vagal tone, myocarditis
Second-Degree AV Block - Type I (Wenckebach / Mobitz I)
- Progressive PR prolongation until a P wave is BLOCKED (no QRS follows)
- Then cycle resets
- Site of block: AV node
- Causes: Inferior MI, digitalis, increased vagal tone
- Usually benign; may not need pacemaker
Second-Degree AV Block - Type II (Mobitz II)
- Constant PR interval with SUDDEN non-conducted P waves (no warning)
- Site of block: Below AV node (His-Purkinje)
- Causes: Anterior MI, sclerodegenerative disease
- High risk of progressing to complete block - PACEMAKER usually needed
Third-Degree (Complete) AV Block
- NO relationship between P waves and QRS complexes (AV dissociation)
- P rate > QRS rate
- Escape rhythm: Junctional (narrow QRS, rate 40-60) or ventricular (wide QRS, rate 20-40)
- Causes: Inferior MI, Lyme disease, surgical trauma, idiopathic fibrosis
- PACEMAKER required
Bundle Branch Blocks
Left Anterior Fascicular Block (LAFB)
- Left axis deviation (axis around -60°); QRS duration normal
- Small Q waves in I, aVL; small R waves in II, III, aVF
- Delayed precordial R-wave progression
Right Bundle Branch Block (RBBB)
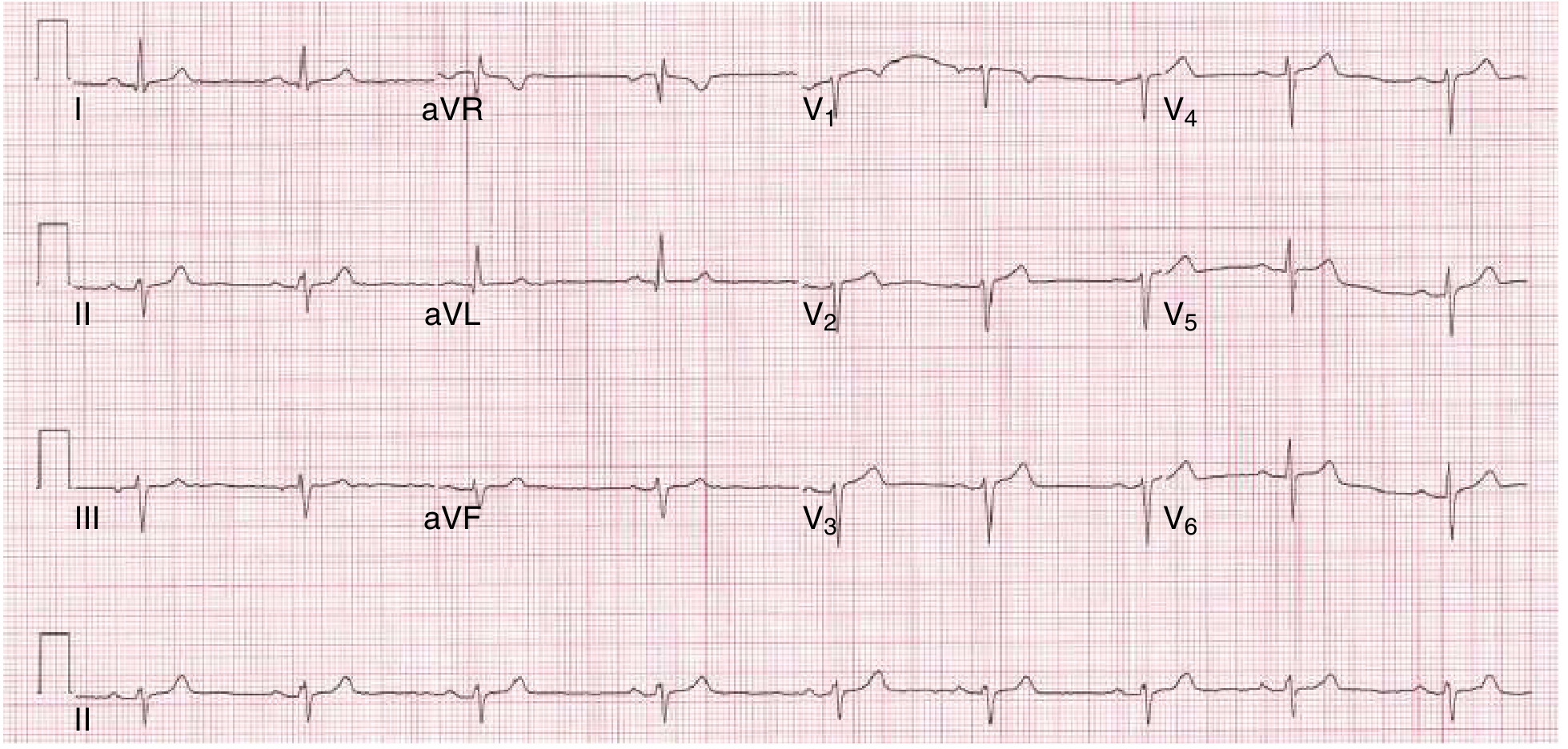
FIGURE 42-5B - RBBB: widened QRS, rsR' ("M" shape) in V1, wide terminal S wave in V5-V6, discordant ST-T changes in right precordial leads. (Goldman-Cecil Medicine)
- ECG hallmarks:
- QRS > 120 ms
- rSR' (M-shape) in V1
- Wide, slurred S wave in I, V5, V6
- Discordant T-wave inversion in V1-V2
- Causes: RV overload, PE, anterior MI, normal variant
Left Bundle Branch Block (LBBB)
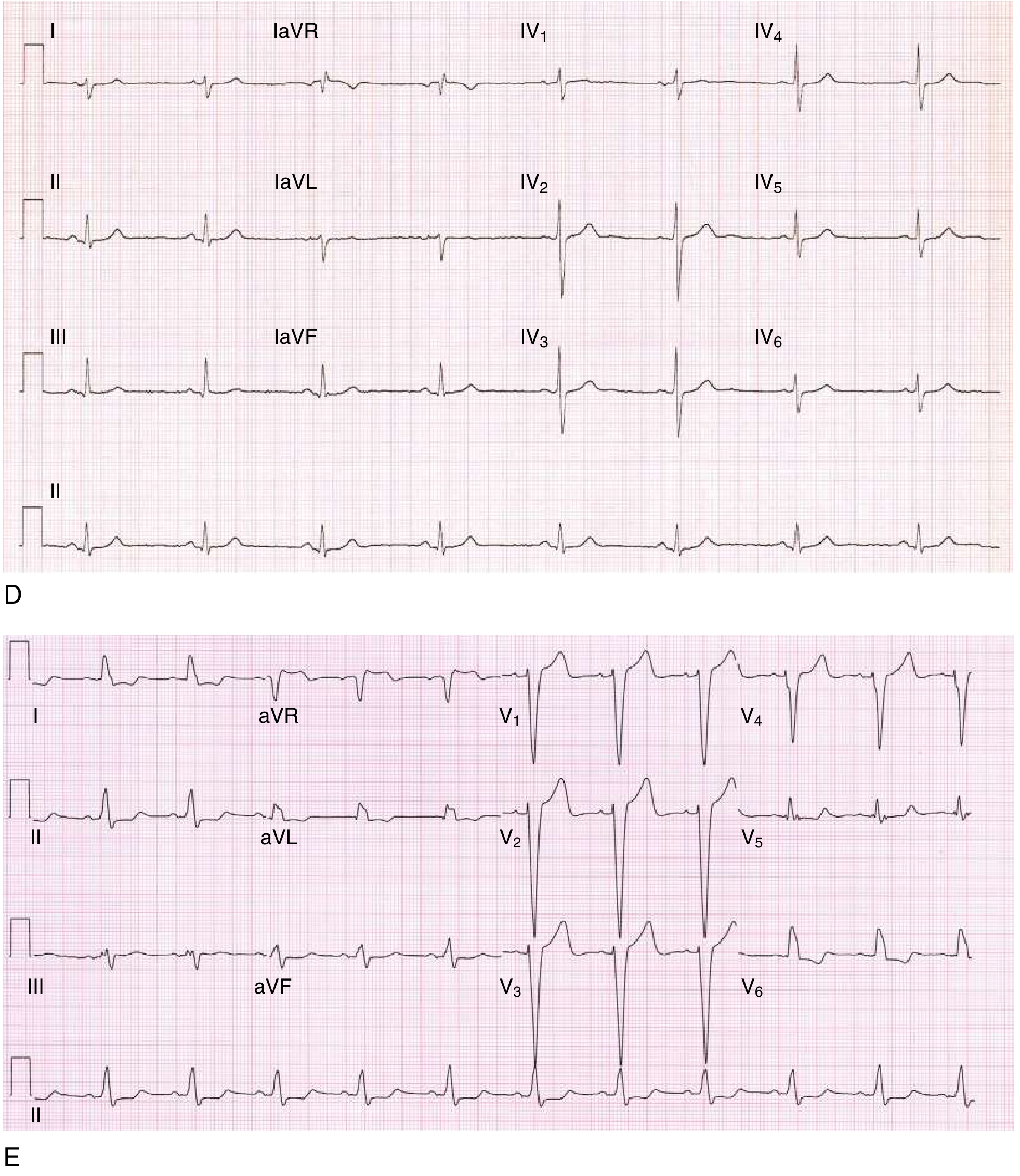
FIGURE 42-5E - LBBB: wide QRS, broad notched R in I, aVL, V5-V6; small r with broad deep S in right precordial leads. ST and T waves discordant throughout. (Goldman-Cecil Medicine)
- ECG hallmarks:
- QRS > 120 ms
- Broad notched ("M-shaped") R in I, aVL, V5-V6
- Small r with deep S in V1-V3 (dominant S)
- No septal Q waves in I, V5-V6
- Discordant ST-T changes
- Causes: CAD, hypertension, cardiomyopathy, aortic stenosis
- New LBBB + symptoms = STEMI equivalent until proven otherwise
Left Posterior Fascicular Block (LPFB)
- Right axis deviation (~+120°); QRS normal duration
- Small R waves in I, aVL; small Q in II, III, aVF
- Diagnosis of exclusion (must rule out RVH)
PART 6: ISCHEMIA AND MYOCARDIAL INFARCTION
Pathophysiology of ECG Changes in Ischemia

FIGURE 247-11 - A: Subendocardial ischemia directs the ST vector inward = ST depression. B: Transmural (epicardial) ischemia directs ST vector outward = ST elevation. (Harrison's Principles of Internal Medicine, 22e)
ECG Evolution of STEMI (Typical Sequence)
| Time | ECG Finding |
|---|---|
| Minutes | Hyperacute tall peaked T waves ("hyperacute T waves") |
| Hours | ST segment elevation (convex/tombstone) |
| Hours-days | T-wave inversion (symmetrical) |
| Days-weeks | Pathological Q waves develop (>40 ms wide, >1/4 amplitude of R) |
| Weeks-months | Q waves may persist permanently (old MI marker) |
ST Elevation Localization by Lead
| Territory | Leads with ST Elevation | Reciprocal ST Depression | Artery |
|---|---|---|---|
| Anterior | V1-V4 | II, III, aVF | LAD |
| Anteroseptal | V1-V3 | - | LAD (septal) |
| Anterolateral | V1-V6, I, aVL | II, III, aVF | LAD / LCx |
| Lateral | I, aVL | II, III, aVF | LCx |
| Inferior | II, III, aVF | I, aVL | RCA |
| Inferolateral | II, III, aVF, V5-V6 | I, aVL | RCA / LCx |
| Posterior | Tall R in V1-V2, ST depression V1-V3 | - (mirror image) | RCA / LCx |
| Right ventricular | ST elevation in V3R-V6R; also II, III, aVF | Lateral leads | RCA (proximal) |
(Source: Tintinalli's Emergency Medicine, Table 49-4)
Anterior Wall Ischemia - T-wave Inversions

FIGURE 247-12 - Severe anterior wall ischemia causes prominent T-wave inversions in V1-V6 and leads I, aVL ("Wellens syndrome / LAD T-wave pattern"). (Harrison's Principles of Internal Medicine, 22e)
Non-ST Elevation MI (NSTEMI) / Unstable Angina
- ECG: ST depression, T-wave inversions, or nonspecific changes
- Unlike STEMI, does NOT get immediate primary PCI based on ECG alone
- Diagnosis confirmed by troponin rise
Posterior MI (True Posterior)
- Tall R waves in V1-V2 (R > S); ST depression in V1-V3
- These are reciprocal changes of posterior ST elevation
- Confirm with posterior leads V7-V9 (ST elevation >0.5 mm)
Right Ventricular MI
- Always suspect when inferior STEMI present (II, III, aVF elevation)
- Get right-sided leads (V4R) - ST elevation >1 mm is diagnostic
- Management: AVOID nitrates and diuretics (preload-dependent)
PART 7: ARRHYTHMIAS
Sinus Node Disorders
| Condition | ECG | Rate |
|---|---|---|
| Sinus tachycardia | Normal P-QRS, regular | >100 bpm |
| Sinus bradycardia | Normal P-QRS, regular | <60 bpm |
| Sinus arrhythmia | P-QRS vary with respiration | Varies |
| Sick sinus syndrome | Brady-tachy pattern; pauses | Variable |
Supraventricular Tachycardias (SVT)
Atrial Fibrillation (AF)
- ECG hallmarks:
- Absent P waves (replaced by irregular fibrillatory "f" waves, rate 350-600/min)
- Irregularly irregular ventricular rhythm (no two R-R intervals the same)
- Narrow QRS (unless aberrant conduction or WPW)
- Causes: Hypertension, valvular disease, heart failure, hyperthyroidism, alcohol
- Rate: Ventricular response typically 100-160/min if uncontrolled
Atrial Flutter
- ECG hallmarks:
- Sawtooth "flutter waves" at atrial rate 250-350/min (typically 300/min)
- Best seen in II, III, aVF and V1
- Regular ventricular rate (usually 2:1 block = ventricular rate ~150/min)
- Key: Regular rate of exactly 150 bpm = suspect atrial flutter 2:1
- Carotid sinus massage slows AV conduction, unmasking flutter waves
AVNRT (AV Nodal Re-entrant Tachycardia)
- Most common paroxysmal SVT
- ECG: Narrow complex tachycardia, rate 150-250/min
- P waves buried in or just after QRS (retrograde, short RP interval)
- Treatment: Vagal maneuvers, adenosine
Wolff-Parkinson-White (WPW) Syndrome
- Accessory pathway (Bundle of Kent) bypasses AV node
- ECG (sinus rhythm):
- Short PR interval (<120 ms)
- Delta wave (slurred QRS upstroke)
- Wide QRS complex
- Risk: AF with rapid conduction down accessory pathway → VF
- DANGER: Do NOT give AV nodal blockers (verapamil, digoxin) in AF+WPW
Ventricular Arrhythmias
Premature Ventricular Contractions (PVCs)
- Wide, bizarre QRS without preceding P wave
- Followed by compensatory pause
- Types: Unifocal (same morphology), multifocal (different morphologies)
- Bigminy = every other beat is a PVC; Trigeminy = every third beat
Ventricular Tachycardia (VT)
- ECG: Wide QRS tachycardia (>120 ms), rate >100 bpm, >3 consecutive beats
- AV dissociation (more QRS than P waves) - pathognomonic of VT
- Fusion beats and capture beats are diagnostic
- Causes: Ischemic heart disease (scar), cardiomyopathy, electrolyte disorders
- Sustained VT = VT lasting >30 seconds (or requiring termination)
Ventricular Fibrillation (VF)
- ECG: Chaotic, rapid, irregular undulations - NO recognizable QRS
- No effective cardiac output - immediate defibrillation required
- Most common initial rhythm in sudden cardiac death
Torsades de Pointes
- "Twisting of the points" - polymorphic VT where QRS axis rotates
- Always preceded by prolonged QT interval
- Causes: Long QT syndrome (congenital or acquired), drugs (antiarrhythmics, antibiotics, antipsychotics), hypokalemia, hypomagnesemia
- Treatment: IV magnesium sulfate, correct electrolytes, pacing
PART 8: METABOLIC & ELECTROLYTE DISORDERS
Hyperkalemia
| Serum K+ | ECG Changes |
|---|---|
| 5.5-6.5 mEq/L | Tall, peaked, tent-shaped T waves (earliest sign) |
| 6.5-7.5 mEq/L | PR prolongation, P wave flattening/loss |
| 7.5-8.0 mEq/L | Wide QRS (intraventricular block), RBBB/LBBB patterns |
| >8.0 mEq/L | Sine-wave pattern, VF, asystole |
- Treatment: Calcium gluconate (stabilizes membrane), then glucose + insulin, bicarbonate, kayexalate
Hypokalemia
- ECG: Flattened T waves, prominent U waves (after T wave), prolonged QU interval
- U waves >T waves = significant hypokalemia
- Risk of torsades de pointes
Hypercalcemia
- ECG: Short QT interval (shortened ST segment)
- Bradycardia, AV block at very high levels
Hypocalcemia
- ECG: Prolonged QT interval (due to prolonged ST segment)
Digitalis Effect (therapeutic level)
- ECG: "Reverse tick" or "Salvador Dali mustache" ST depression (scooped ST in V5-V6)
- Slowed AV conduction (longer PR interval)
- Digitalis toxicity: PVCs, bigeminy, accelerated junctional rhythm, various AV blocks
PART 9: MISCELLANEOUS CONDITIONS
Pulmonary Embolism (PE)
- Most common ECG finding: Sinus tachycardia
- Classic (uncommon) pattern: S1Q3T3
- Large S wave in lead I
- Q wave in lead III
- Inverted T wave in lead III
- Other findings: New RBBB, right axis deviation, T-wave inversions V1-V4, P pulmonale
- These reflect acute right heart strain
Pericarditis
- ECG (acute stage):
- Diffuse (saddle-shaped/concave upward) ST elevation in almost ALL leads
- PR segment depression (very specific for pericarditis)
- No reciprocal changes (unlike STEMI)
- Evolution over days/weeks: ST normalizes, T-wave inversions, then normalization
Hypertrophic Cardiomyopathy (HCM)
- Often markedly abnormal ECG despite young patient
- LVH criteria; deep Q waves in lateral leads (I, aVL, V5-V6) from septal hypertrophy
- Widespread T-wave inversions
Long QT Syndrome
- QTc > 440-460 ms
- Congenital (Romano-Ward, Jervell-Lange-Nielsen) or acquired (drug-induced)
- Risk of torsades de pointes and sudden death
Brugada Syndrome
- ECG: Right bundle branch block pattern + ST elevation in V1-V3 (coved/saddleback type)
- Normal-appearing heart; risk of sudden VF
- Type 1 (coved): Down-sloping ST elevation ≥2 mm then negative T wave in V1-V2
- Sodium channel mutation (SCN5A)
Hypothermia
- ECG: Osborn wave (J wave) - positive deflection at J point, best in V4-V6
- Bradycardia, prolonged intervals (PR, QRS, QT), muscle tremor artifact
- At severe temperatures: VF risk
Dextrocardia
- ECG: Negative P, QRS, T in lead I; right-sided precordial progression
- R-wave decreases from V1 to V6 (reversed)
- Corrected by reversing arm leads and placing precordial leads on right side
PART 10: ECG IN SPECIFIC PATIENT SCENARIOS
Cardiac Monitoring in the ICU / OR
From Braunwald's - FIGURE 61.11 (ECG events and artifacts):
- Sinus rhythm with short bursts of atrial tachycardia
- Pseudo-arrhythmia from electrode artifact (mimicking flutter or VT)
- Nonsustained VT: wide, rapid QRS not preceded by P wave
- Pseudo-pacemaker failure artifact (flat ECG with preserved pulse on arterial line)
Post-Cardiac Arrest ECG
- After ROSC, obtain 12-lead ECG immediately
- ST elevation → cardiac catheterization
- Note: ~1/3 of post-arrest patients without ST elevation still have acute coronary occlusion
- New LBBB post-arrest should raise suspicion for anterior MI
QUICK SUMMARY TABLE - Disease vs ECG Pattern
| Disease | Key ECG Finding |
|---|---|
| Normal sinus rhythm | Rate 60-100; P before each QRS; PR 120-200 ms; QRS <120 ms |
| Sinus tachycardia | Rate >100, normal P-QRS |
| Atrial fibrillation | No P waves, irregularly irregular QRS |
| Atrial flutter | Sawtooth waves 300/min, regular ventricular rate (often 150 bpm) |
| WPW | Short PR, delta wave, wide QRS |
| 1st degree AV block | PR >200 ms |
| Mobitz I (Wenckebach) | Progressive PR lengthening then dropped beat |
| Mobitz II | Constant PR with sudden dropped beats |
| 3rd degree (complete) block | AV dissociation, escape rhythm |
| RBBB | rSR' in V1, wide S in I/V6, QRS >120 ms |
| LBBB | Broad notched R in I/aVL/V6, QRS >120 ms |
| STEMI anterior | ST elevation V1-V4 |
| STEMI inferior | ST elevation II, III, aVF |
| STEMI lateral | ST elevation I, aVL, V5-V6 |
| Posterior MI | Tall R in V1-V2, ST depression V1-V3 |
| RV MI | ST elevation V4R |
| Pericarditis | Diffuse concave ST elevation, PR depression |
| Hyperkalemia | Peaked T waves → wide QRS → sine wave |
| Hypokalemia | Flat T waves, prominent U waves |
| Long QT | QTc >440-460 ms |
| Torsades de Pointes | Polymorphic VT twisting around axis, preceded by long QT |
| PE | S1Q3T3 pattern, sinus tachycardia, new RBBB |
| Brugada | RBBB pattern + coved ST elevation V1-V2 |
| LVH | Sokolow >35 mm, lateral strain pattern |
| RVH | Tall R in V1, RAD, T inversions V1-V3 |
| Digitalis toxicity | PVCs/bigeminy, scooped ST, AV blocks |
| Hypothermia | Osborn (J) waves, bradycardia |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - Chapter 247 (ECG)
- Goldman-Cecil Medicine, International Edition - Chapters 42 & 52 (Arrhythmias, Conduction)
- Tintinalli's Emergency Medicine - Chapter 49 (AMI/ECG)
- Costanzo Physiology, 7th Ed. - Chapter 4 (Cardiac Physiology/ECG)
- Braunwald's Heart Disease, 10e - Chapter 61 (Ambulatory/monitoring ECG)
This is a shared conversation. Sign in to Orris to start your own chat.