Key nasofacial angles and metrices with respect to facial aesthetics and SLAD-R procedure both in detail according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
SLAD-R procedure ENT septoplasty rhinoplasty nasofacial angles
Finding Sources
Searching the Web
SLAD-R procedure nasal surgery ENT definition technique
Loading Image
Loading Image
Reading Web Page
https://laryngopedia.com/slad-r
Loading Image
Searching the Web
SLAD-R surgical technique steps bilateral RLN ansa cervicalis reinnervation Berke
Reading Web Page
https://www.uclahealth.org/sites/default/files/documents/Chh…
I now have comprehensive data from both the textbooks and authoritative sources to compile a detailed, well-illustrated answer. Let me compose the full response.
Nasofacial Angles, Facial Aesthetic Metrics & the SLAD-R Procedure
PART 1: KEY NASOFACIAL ANGLES AND FACIAL AESTHETIC METRICS
Facial Proportions - The Classic Framework
Before angles, facial analysis begins with proportional divisions (KJ Lee's Essential Otolaryngology):
Vertical Fifths (width):
- The face is divided into 5 equal vertical segments, demarcated laterally by the outer ear, lateral canthi, and medial canthi.
- Each fifth approximates the width of one eye = intercanthal distance.
Horizontal Thirds (height):
- Upper third: trichion to glabella
- Middle third: glabella to subnasale
- Lower third: subnasale to menton
Lower Third Subdivision:
- Subnasale to stomion = 1/3 of lower facial height
- Stomion to menton = 2/3 of lower facial height
Ideal Facial Width:Length ratio = 3:4
The Powell and Humphreys Nasofacial Angle System
The framework most used in ENT/facial plastic surgery is the Powell and Humphreys classification, which defines four key angles relating the nose to the face on lateral profile view. Here is the facial angles diagram from KJ Lee:
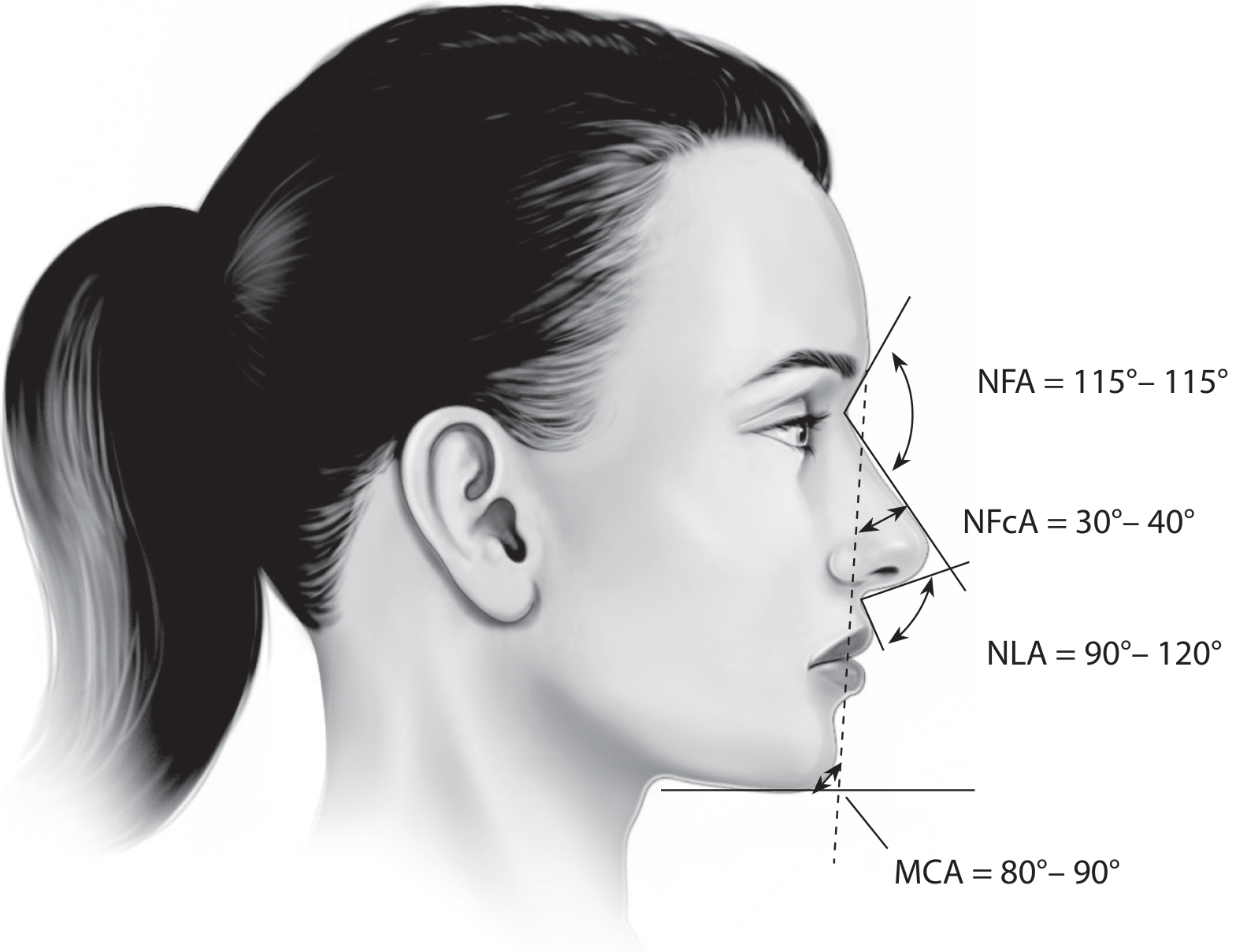
1. Nasofrontal Angle (NFA)
| Feature | Detail |
|---|---|
| Definition | Intersection of the glabella-to-nasion line with the nasion-to-nasal-tip line (nasal dorsal line) |
| Normal range | 115-130° |
| Landmarks | Glabella, nasion, nasal tip |
| Clinical note | A shallow (acute) NFA gives the nose a projecting, prominent appearance; an obtuse angle makes the nasal bridge appear recessed |
2. Nasofacial Angle (NFcA)
| Feature | Detail |
|---|---|
| Definition | Intercept of the facial plane (glabella to pogonion) with the nasal dorsal line (nasion to tip) |
| Normal range | 30-40° (ideal 36°) |
| Landmarks | Glabella, pogonion, nasion, nasal tip |
| Clinical note | Reflects the incline of the nasal dorsum relative to the face; used to quantify nasal projection |
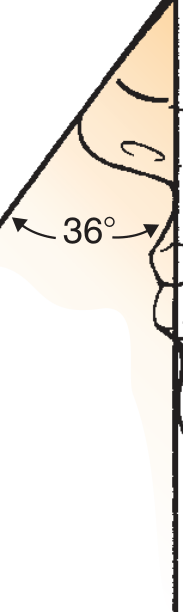
Fig: Nasofacial angle, ideally 36 degrees - Cummings Otolaryngology
3. Nasolabial Angle (NLA)
| Feature | Detail |
|---|---|
| Definition | Angular inclination of the columella as it meets the upper lip. Intersection of a line tangent to labrale superius-subnasale with a line from subnasale to the most anterior point of the columella |
| Normal range - Women | 95-110° (some sources extend to 120°) |
| Normal range - Men | 90-95° |
| Landmarks | Labrale superius, subnasale, columella tip |
| Clinical note | Decreased angle = plunging/over-rotated tip; increased angle = over-rotated/upturned tip. Affected by columellar position and tip rotation |
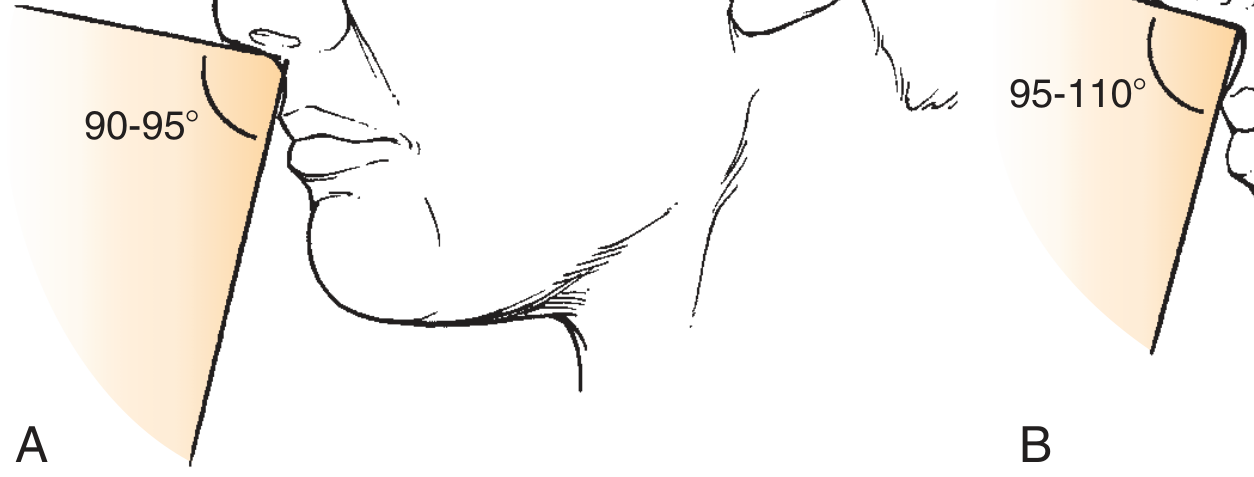
Fig: Nasolabial angle - A (male) 90-95°, B (female) 95-110° - Cummings Otolaryngology
4. Nasomental Angle (NMA)
| Feature | Detail |
|---|---|
| Definition | Intersection of the nasal dorsal line (nasion to nasal tip) with the nasomental line (tip to pogonion) |
| Normal range | 120-132° |
| Landmarks | Nasion, nasal tip, pogonion |
| Clinical note | Altered by chin or lip dysharmony. Lips should fall just behind this line: upper lip ~4 mm behind, lower lip ~2 mm behind |
5. Mentocervical Angle (MCA)
| Feature | Detail |
|---|---|
| Definition | Intercept of the facial plane (glabella to pogonion) with the menton-to-cervical-point line |
| Normal range | 80-95° |
| Clinical note | Assesses submental/chin-neck contour; affected by neck laxity, submental fat, and chin position |
Summary Table: Powell and Humphreys Angles
| Angle | Landmarks | Normal Range | Ideal |
|---|---|---|---|
| Nasofrontal (NFA) | Glabella-nasion / nasion-tip | 115-130° | ~120° |
| Nasofacial (NFcA) | Glabella-pogonion / nasion-tip | 30-40° | 36° |
| Nasolabial (NLA) | Columella / upper lip | M: 90-95° / F: 95-110° | - |
| Nasomental (NMA) | Nasion-tip / tip-pogonion | 120-132° | - |
| Mentocervical (MCA) | Facial plane / menton-cervix | 80-95° | - |
Nasal Projection and Rotation Metrics
Beyond angles, projection and rotation are separately quantified:
1. Tip Rotation
- Occurs along an arc with radius based at the external auditory canal (Cummings).
- Rotation increases along the upper arc and decreases along the lower arc.
2. Simons' Method (Projection)
- Nasal tip projection ≈ length of the upper lip (ratio 1:1).
3. Goode's Method (Projection)
- Draw a vertical from the nasion to the alar groove.
- Draw a perpendicular from the alar groove to the nasal tip.
- Ratio of (alar groove to tip) : (nasion to tip) = 0.55 to 0.60
- When this ratio is maintained, the NFcA approximates 36°.
4. Crumley-Lanser Method
- Uses a 3-4-5 right triangle: hypotenuse = nasal length; projection = smallest arm.
5. Alar-Columellar Complex
- Ala-to-tip / lobular complex ratio: optimal 1:1
- Columellar show on lateral view: 3-5 mm is acceptable
Ethnic Variations (Dermatology 2-Vol Set, 5e)
| Parameter | Caucasian | Asian | African |
|---|---|---|---|
| Nasolabial angle | ~136-138° | ~136° | ~137-138° |
| Nasofacial angle | 31-40° | ~33-39° | ~38-41° |
(Note: Some sources measure NLA differently, leading to slightly higher values than the Powell-Humphreys method above.)
PART 2: SLAD-R PROCEDURE
What is SLAD-R?
SLAD-R = Selective Laryngeal Adductor Denervation-Reinnervation
This is a laryngeal surgery (not a nasal procedure) developed by Dr. Gerald Berke at UCLA in the late 1990s for the treatment of Adductor Spasmodic Dysphonia (ADSD) - a focal laryngeal dystonia causing involuntary hyperadduction of the vocal folds during phonation, producing a strained, strangled voice quality with characteristic voice breaks.
Important clarification: SLAD-R is a laryngology/voice procedure, entirely separate from rhinoplasty or facial aesthetics. It is covered in ENT textbooks under laryngeal dystonia and phonosurgery.
Background and Rationale
- In ADSD, the thyroarytenoid (TA) and lateral cricoarytenoid (LCA) muscles (adductors) fire involuntarily during speech via the recurrent laryngeal nerve (RLN).
- Standard of care had been repeated botulinum toxin (Botox) injections into the TA muscle - effective but temporary (3-4 months), requiring ongoing injections.
- The Dedo operation (RLN section alone) provided initial relief but had high recurrence rates because the proximal RLN stump re-innervated the adductors over time with dystonic impulses.
- SLAD-R was designed to overcome this failure by combining denervation with reinnervation using the ansa cervicalis, which provides tonic non-dystonic neural input, preventing pathological re-innervation.
Indications
- Adductor Spasmodic Dysphonia confirmed by laryngoscopy and EMG
- Inadequate response to, or patient dissatisfaction with, Botox injections
- Patient willingness to accept 3-6 months of post-operative breathiness
- Confirmed intact distal RLN stumps and intact ansa cervicalis bilaterally
- Normal glottic airway (not compromised)
Contraindications
- Glottic airway compromise
- Absent distal RLN stump
- Absent ansa cervicalis bilaterally
- Poor prognosis (insufficient life expectancy to benefit from reinnervation)
Surgical Technique (Chhetri and Berke, UCLA)
The operation is bilateral and proceeds in sequential steps on each side:
Pre-operative preparation:
- EMG-equipped endotracheal tube (NIM-Response System, Medtronic Xomed) to monitor RLN integrity intraoperatively
- Operating table rotated 90° from anesthesiologist; surgeon stands at the head
- Shoulder roll placed to extend the neck
- IV dexamethasone 10 mg and prophylactic antibiotics before incision
Step 1 - Neck incision and exposure:
- A horizontal cervical incision is made (similar to thyroid/parathyroid approach)
- Subplatysmal flaps elevated
- The strap muscles are divided or retracted to expose the larynx
Step 2 - Identification of the RLN:
- The recurrent laryngeal nerve is traced to its entry into the larynx
- The anterior (adductor) branch of the RLN - supplying the TA and LCA - is identified
- Intraoperative EMG confirms nerve identity
Step 3 - Selective adductor denervation:
- A laryngotomy window is opened to expose the TA muscle insertion
- A 3-0 silk suture ties the anterior RLN branch close to its TA insertion
- The nerve is divided distal to the suture, leaving an adequate distal stump for anastomosis
- The nerve is retracted posteriorly and freed to the posterior border of the laryngotomy window
- The branch to the LCA is identified during this maneuver and divided
Step 4 - LCA partial myotomy:
- A partial LCA myotomy is performed at the midbelly using microscissors
- This prevents LCA re-innervation from the proximal adductor nerve stump
- Initially full LCA myotomy was done; now partial myotomy is preferred to avoid permanent breathiness (especially in males)
- The distal RLN stump is sutured to the posterior lamina of the thyroid cartilage via the French-eye needle technique
Step 5 - Ansa cervicalis reinnervation:
- A branch of the ansa cervicalis nerve (C1-C3, normally supplying infrahyoid strap muscles) is harvested
- Microsurgical neurorrhaphy (7-0 or 8-0 nylon, epineural anastomosis x3 locations) is performed connecting the ansa cervicalis branch to the severed adductor nerve stump
- This provides tonic, non-dystonic reinnervation
- Microsurgical magnification (loupe or operating microscope) is mandatory
Step 6 - Repeat on contralateral side:
- The procedure is repeated on the other side of the neck
Post-operative Course and Outcomes
| Phase | Timeframe | Expected Finding |
|---|---|---|
| Immediate | 0-2 weeks | Markedly breathy, whispery voice |
| Early recovery | 1-3 months | Gradually improving voice volume |
| Reinnervation | 3-6 months | Return of vocal fold tone from ansa reinnervation |
| Long-term | >6 months | Fluent voice, minimal breathiness |
Long-term results (Chhetri & Berke, 81 patients, mean follow-up 49 months):
- 83% had significantly improved Vocal Handicap Index-10 (VHI-10) scores
- 91% rated post-surgery voice as more fluent than after Botox
- Majority achieved fluent voice with absent-to-minimal breathiness
Comparison with Botulinum Toxin
| Feature | Botox Injections | SLAD-R |
|---|---|---|
| Duration of effect | 3-4 months | Long-term (years) |
| Repeatability | Repeated indefinitely | One-time (bilateral) |
| Breathy phase | Short (1-2 weeks) | Prolonged (3-6 months) |
| Reversibility | Reversible | Irreversible |
| Invasiveness | Office procedure | Open neck surgery |
| Long-term control | High but temporary | Sustained in ~83-91% |
Key Nerves Involved
| Nerve | Role |
|---|---|
| RLN - anterior (adductor) branch | Supplies TA and LCA; severed in SLAD-R |
| RLN - posterior (abductor) branch | Supplies posterior cricoarytenoid (PCA); preserved |
| Ansa cervicalis (C1-C3) | Supplies infrahyoid muscles; harvested for reinnervation graft |
Sources:
- Cummings Otolaryngology Head and Neck Surgery - Nasofacial Relationships, Nasal Rotation and Projection (Ch. 16)
- KJ Lee's Essential Otolaryngology - Facial Angles (Figure 54-2), p. 1057
- Chhetri DK & Berke GS. "Treatment of Adductor Spasmodic Dysphonia with Selective Laryngeal Adductor Denervation-Reinnervation Surgery." UCLA Health/Ann Otol Rhinol Laryngol 1999;108(3):227-31.
- Laryngopedia - SLAD-R overview
This is a shared conversation. Sign in to Orris to start your own chat.