Direct bilirubinemia vs indirect bilirubinemia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive content. Now I'll compile a thorough, well-organized answer.
Direct (Conjugated) vs. Indirect (Unconjugated) Bilirubinemia
1. Origin of the Terms
The terms "direct" and "indirect" come from the van den Bergh diazo reaction (1916). Bilirubin reacts with diazotized sulfanilic acid to form a reddish-purple azopigment. Conjugated bilirubin reacts directly with the reagent (no accelerator needed), while unconjugated bilirubin reacts only indirectly (after addition of methanol or another accelerator). Total bilirubin minus direct bilirubin = indirect bilirubin.
- Tietz Textbook of Laboratory Medicine, 7th Ed, p. 1971
2. Bilirubin Metabolism - The Pathway
The steps involved:
| Step | What happens | Bilirubin form |
|---|---|---|
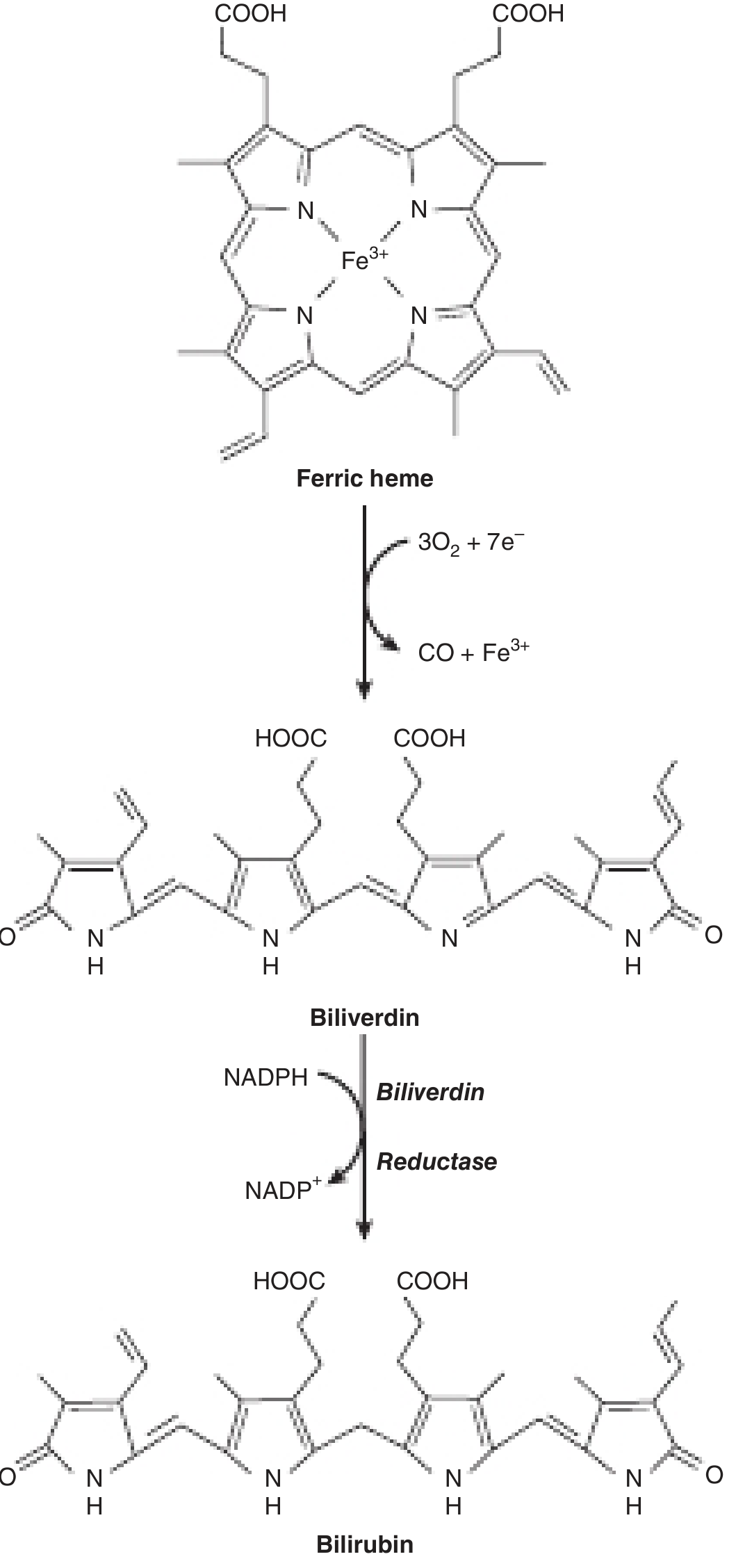
| RBC breakdown | Heme oxygenase cleaves ferric heme → biliverdin → bilirubin (via biliverdin reductase, using NADPH) | Unconjugated (indirect) |
| Plasma transport | Unconjugated bilirubin is lipid-soluble, non-polar; bound tightly to albumin | Indirect |
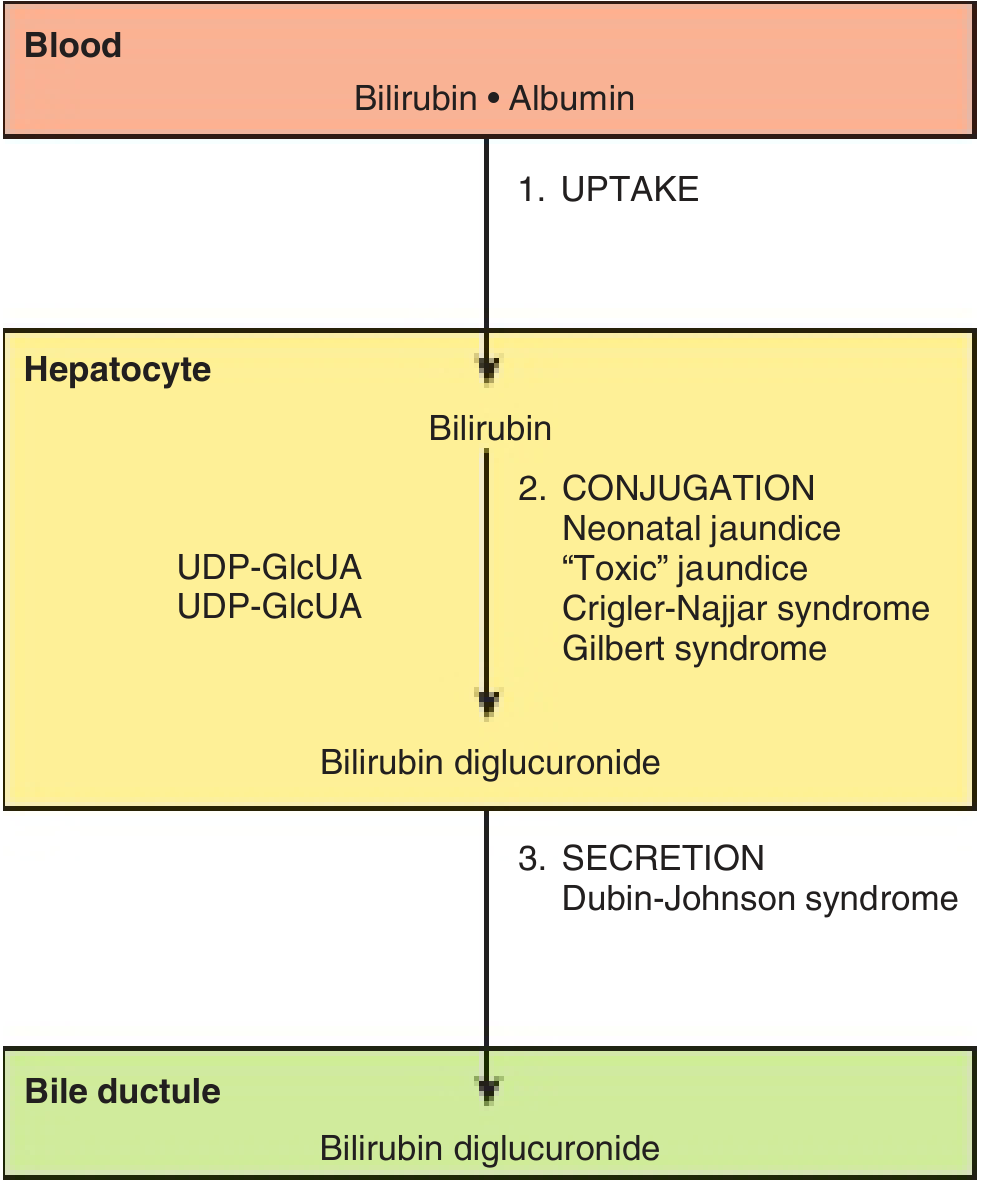
| Hepatic uptake | Removed from albumin at sinusoidal surface; binds intracellular glutathione S-transferase (ligandin) | Indirect |
| Conjugation | UDP-glucuronosyltransferase (UGT1A1) in ER attaches two glucuronate molecules → bilirubin diglucuronide | Direct (conjugated) |
| Biliary secretion | Active transport via MRP2 (MOAT) into bile canaliculi - rate-limiting step | Direct |
| Gut | Bacterial β-glucuronidases cleave glucuronides → urobilinogen → urobilin (fecal/urinary excretion) | - |
3. Key Properties Compared
| Property | Indirect (Unconjugated) | Direct (Conjugated) |
|---|---|---|
| Chemistry | Free bilirubin bound to albumin | Bilirubin diglucuronide (mainly) |
| Solubility | Lipid-soluble, water-insoluble | Water-soluble |
| Plasma binding | Tightly bound to albumin | Loosely bound (or free) |
| Crosses BBB? | Yes - can cause kernicterus | No |
| Appears in urine? | No (cannot pass glomerulus) | Yes (choluria/dark urine) |
| Normal range | 0.2-0.8 mg/dL | 0-0.3 mg/dL |
| Total bilirubin | Measured with accelerator | Measured without accelerator |
| δ-bilirubin | N/A | Covalently bound to albumin; appears in prolonged conjugated hyperbilirubinemia |
- Harper's Illustrated Biochemistry, 32nd Ed, p. 334
- Quick Compendium of Clinical Pathology, 5th Ed, p. 223
4. Causes of Hyperbilirubinemia
Indirect (Unconjugated) Hyperbilirubinemia
Caused by problems before or during conjugation - too much bilirubin delivered to the liver, or failure to conjugate it:
| Mechanism | Example Conditions |
|---|---|
| Excess heme breakdown (overproduction) | Hemolytic anemias, ineffective erythropoiesis, resorption of large hematoma |
| Excess delivery via shunting | Cirrhosis with portosystemic shunts, right heart failure |
| Impaired hepatic uptake | Gilbert syndrome, drugs (rifampin, probenecid) |
| Impaired conjugation (UGT1A1 deficiency) | Crigler-Najjar type I & II, neonatal physiologic jaundice, hypothyroidism |
Gilbert syndrome - mild unconjugated hyperbilirubinemia (usually <3 mg/dL); UGT1A1 activity 10-35% of normal; very common (~8% prevalence); bilirubin fluctuates with fasting, stress, intercurrent illness. - Harrison's Principles of Internal Medicine, 22nd Ed
Crigler-Najjar type I - complete absence of UGT1A1; severe unconjugated hyperbilirubinemia; kernicterus risk if untreated.
Crigler-Najjar type II - markedly reduced but detectable UGT1A1; less severe.
Direct (Conjugated) Hyperbilirubinemia
Caused by problems after conjugation - failure to secrete conjugated bilirubin into bile or obstruction to bile flow. Conjugated hyperbilirubinemia is said to be present when >30% of serum bilirubin is conjugated.
| Mechanism | Example Conditions |
|---|---|
| Impaired canalicular secretion (hepatocellular) | Viral hepatitis, sepsis/endotoxin, estrogen (pregnancy, OCP), cyclosporine |
| Genetic secretory defects | Dubin-Johnson syndrome (MRP2 mutation), Rotor syndrome |
| Intrahepatic cholestasis | Primary biliary cholangitis, drug-induced cholestasis, intrahepatic cholestasis of pregnancy, alcoholic hepatitis |
| Extrahepatic obstruction | Choledocholithiasis, cholangiocarcinoma, pancreatic head carcinoma, primary sclerosing cholangitis, stricture |
- Quick Compendium of Clinical Pathology, 5th Ed, p. 223
5. Clinical Differentiation
| Feature | Indirect (Unconjugated) | Direct (Conjugated) |
|---|---|---|
| Urine color | Normal (no bilirubinuria) | Dark (bilirubinuria - "Coca-Cola urine") |
| Stool color | Normal to pale | Pale/acholic (if obstruction) |
| Pruritus | Absent | Present (esp. cholestatic) |
| Neurological signs | Kernicterus (esp. neonates) | Absent |
| ALT/AST | Usually normal or mildly elevated | Elevated in hepatocellular; less in cholestatic |
| Alkaline phosphatase | <3× ULN | >3× ULN (cholestatic) |
| Serum cholesterol | Normal | Elevated (cholestasis) |
| Urinary urobilinogen | Elevated (hemolysis) | Decreased/absent (obstruction) |
Approach to a jaundiced patient (Harrison's)
The initial steps are to determine: (1) whether hyperbilirubinemia is predominantly conjugated or unconjugated, and (2) whether other liver biochemical tests are abnormal. - Harrison's Principles of Internal Medicine, 22nd Ed, Block 5
6. Special Notes
- Neonatal jaundice is predominantly unconjugated (indirect), due to immature UGT1A1 activity + increased bilirubin production from fetal hemoglobin turnover. In adults, jaundice is usually conjugated.
- Kernicterus occurs only with unconjugated bilirubin (crosses the BBB due to its lipid solubility); conjugated bilirubin cannot cause it.
- Choluria (bile pigments in urine) occurs only with conjugated hyperbilirubinemia - the water-soluble form passes the glomerular filter.
- δ-bilirubin: In prolonged conjugated hyperbilirubinemia (e.g., obstructive jaundice), bilirubin becomes covalently bound to albumin (δ-fraction). It is measured as "direct" on standard assays but has a long half-life (~21 days), explaining why jaundice persists even after relief of obstruction.
- In obstructive jaundice, plasma bilirubin conjugates are predominantly monoglucuronides (vs. the normal diglucuronide in bile).
Sources:
- Harper's Illustrated Biochemistry, 32nd Ed (Chapters 31)
- Harrison's Principles of Internal Medicine, 22nd Ed (Chapter on jaundice, disorders of bilirubin metabolism)
- Quick Compendium of Clinical Pathology, 5th Ed (Section 1.1.1.7)
- Tietz Textbook of Laboratory Medicine, 7th Ed (Chapter 51)
This is a shared conversation. Sign in to Orris to start your own chat.