All about hypernatremia viva question and answer in easy way
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough and easy-to-understand viva Q&A on hypernatremia, compiled from multiple authoritative medical textbooks:
Hypernatremia - Viva Questions & Answers
🔵 BASICS
Q1. What is hypernatremia?
A. Hypernatremia is defined as a serum sodium (Na+) concentration above 145 mEq/L. It always reflects a hyperosmolar state - meaning the blood is too concentrated relative to water.
Simple memory trick: "Too much salt, too little water"
Q2. What is the key concept behind hypernatremia?
A. Three golden rules:
- Hypernatremia is always a water problem, and sometimes also a salt problem.
- For hypernatremia to persist, the patient must either have a defect in thirst or limited access to free water.
- The serum Na+ level itself does NOT tell you anything about total body sodium or volume status.
Q3. Who is at highest risk for hypernatremia?
A. High-risk groups:
- Elderly (impaired thirst sensation)
- Infants (cannot access water themselves)
- Comatose or intubated patients (no access to water)
- Patients with dementia or neurological disease
- Patients in the ICU (6-26% develop hypernatremia in the ICU)
🔵 CAUSES / CLASSIFICATION
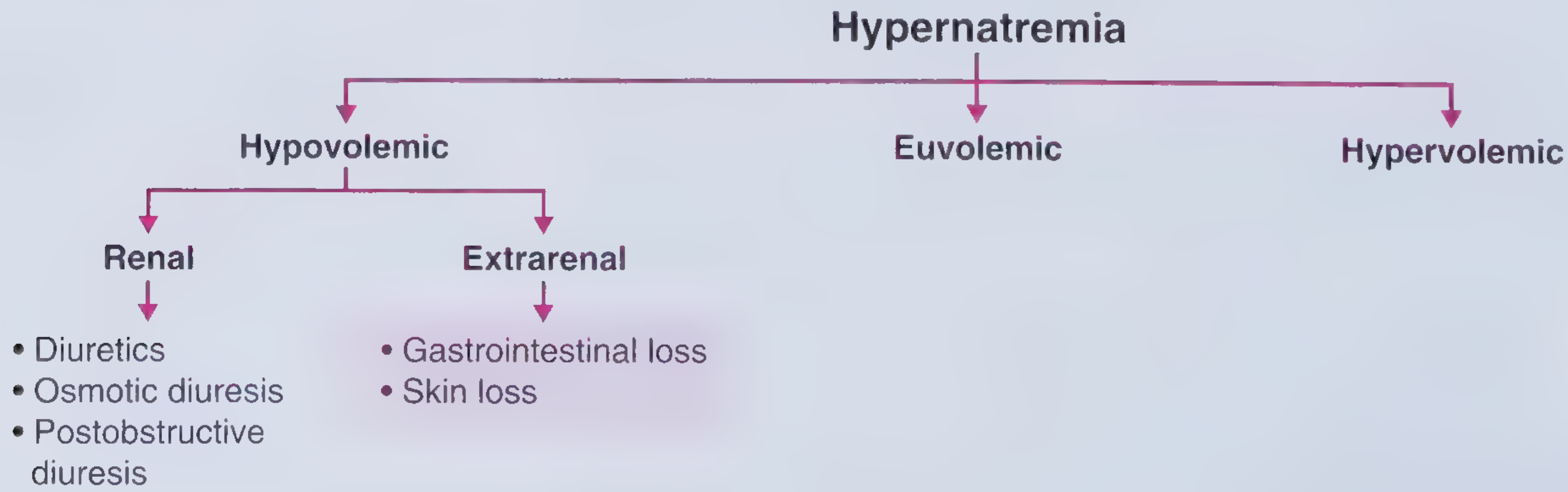
Q4. How do you classify hypernatremia by volume status?
A. Three types:
| Type | Mechanism | Examples |
|---|---|---|
| Hypovolemic | Loss of hypotonic fluid (water > salt) | Diarrhea, vomiting, burns, sweating, osmotic diuresis |
| Euvolemic | Pure water deficit (normal body sodium) | Diabetes insipidus (DI), decreased water intake |
| Hypervolemic | Gain of hypertonic fluid (salt > water) | Hypertonic saline, sodium bicarbonate IV, hyperaldosteronism, Cushing's |
(Source: Frameworks for Internal Medicine, Rosen's Emergency Medicine)
Q5. What are the causes of hypovolemic hypernatremia?
A.
- Renal causes: Diuretics, osmotic diuresis (glucose, mannitol), post-obstructive diuresis
- Extrarenal causes: GI losses (diarrhea, vomiting, NG tube drainage), skin losses (burns, excessive sweating in marathon runners)
Key fact: Sweat Na+ is ~40 mEq/L - always lower than serum, so sweat loss causes hypotonic fluid loss → hypernatremia
Q6. What are causes of euvolemic hypernatremia?
A. Pure water loss without sodium loss:
- Diabetes insipidus (DI) - most important cause
- Inadequate water intake (impaired thirst / no access)
- Insensible losses (fever, respiratory)
Q7. What are causes of hypervolemic hypernatremia?
A. Excess sodium intake:
- Hypertonic saline IV
- IV sodium bicarbonate
- Salt tablet ingestion / seawater ingestion
- Hypertonic saline enemas
- Hypertonic tube feeds
- Primary hyperaldosteronism / Conn syndrome
- Cushing syndrome
- Hemodialysis errors
🔵 DIABETES INSIPIDUS (DI)
Q8. What is diabetes insipidus?
A. DI is a syndrome characterized by production of excessive volumes (>50 mL/kg/day) of dilute urine (osmolality < 300 mOsm/kg). Symptoms include thirst, polyuria, enuresis, and nocturia. Dehydration does NOT usually occur if the thirst mechanism is intact.
Q9. What are the two types of DI? How are they different?
A.
| Feature | Central DI | Nephrogenic DI |
|---|---|---|
| Defect | Insufficient ADH secretion | Renal resistance to ADH |
| Causes | Head trauma, neurosurgery, idiopathic, sarcoidosis, malignancy, autoimmune | Lithium, hypercalcemia, hypokalemia, amyloidosis, polycystic kidney disease, sickle cell |
| Treatment | DDAVP (desmopressin) | Low Na+ diet + thiazide diuretics |
(Source: Frameworks for Internal Medicine)
Q10. How do you differentiate central from nephrogenic DI?
A. Using the water deprivation test followed by desmopressin (DDAVP):
- If urine concentrates after DDAVP → Central DI (ADH deficient, responds to replacement)
- If urine does NOT concentrate after DDAVP → Nephrogenic DI (resistant to ADH)
🔵 PATHOPHYSIOLOGY
Q11. What happens to the brain in hypernatremia?
A.
- High serum osmolality causes water to shift OUT of brain cells → brain shrinkage (cerebral dehydration)
- This can cause rupture of cerebral veins and subarachnoid hemorrhage
- In chronic hypernatremia, brain cells adapt by accumulating idiogenic osmoles (organic solutes) to pull water back in - this is why rapid correction is dangerous (causes cerebral edema)
Q12. Why is acute hypernatremia more dangerous than chronic?
A.
- Acute (<24 hours): Brain has not adapted; severe neurological damage occurs rapidly. Na+ >160 mEq/L → 75% mortality in adults
- Chronic (>48-72 hours): Brain adapts by generating idiogenic osmoles; symptoms may be mild. Mortality ~10%
- This distinction drives how quickly we correct it
🔵 CLINICAL FEATURES
Q13. What are the symptoms and signs of hypernatremia?
A. Symptoms arise from two sources:
From dehydration:
- Tachycardia
- Orthostatic hypotension
- Dry mucous membranes and axillae
From hypernatremia itself (CNS effects):
- Thirst (earliest symptom)
- Muscle weakness, restlessness, lethargy, insomnia
- Depressed sensorium → delirium → coma
- Focal neurological deficits
- Seizures
- Intracranial hemorrhage (subarachnoid hemorrhage)
Symptoms are more severe when hypernatremia develops rapidly.
Other metabolic effects:
- Inhibits insulin release → hyperglycemia
- Increases insulin resistance
- Decreases hepatic gluconeogenesis and lactate clearance
- Decreases cardiac function
(Source: Sabiston Textbook of Surgery, NKF Primer on Kidney Diseases)
Q14. What is the single most important prognostic indicator in hypernatremia?
A. The level of consciousness, not the absolute serum Na+ value. A decreased level of consciousness is strongly associated with mortality.
🔵 INVESTIGATION
Q15. What investigations do you order in hypernatremia?
A.
- Serum Na+, K+, creatinine, BUN, glucose
- Serum osmolality
- Urine osmolality (key!)
- Urine sodium concentration
- Urine specific gravity
Key interpretation using urine osmolality:
| Urine Osmolality | Interpretation |
|---|---|
| > 600 mOsm/L | Kidney conserving water normally → impaired intake (neurological cause, no access to water) |
| 300-600 mOsm/L | Partial DI or osmotic diuresis |
| < 300 mOsm/L | DI (complete central or nephrogenic) - kidneys not concentrating |
(Source: Symptom to Diagnosis, 4th Ed.)
Q16. How do you calculate the free water deficit?
A.
Free Water Deficit (L) = TBW × [(Serum Na+ / 140) - 1]
Where TBW (Total Body Water) = body weight (kg) × correction factor:
| Population | TBW Factor |
|---|---|
| Children + adult men | × 0.6 |
| Adult women | × 0.5 |
| Elderly men | × 0.5 |
| Elderly women | × 0.45 |
Example: 70 kg male with Na+ = 160 mEq/L
- TBW = 70 × 0.6 = 42 L
- Deficit = 42 × [(160/140) - 1] = 42 × 0.143 = 6 L
Important: This formula gives a snapshot only. It does NOT account for ongoing losses (urine, sweat, GI). Always recheck Na+ frequently and factor in ongoing losses.
(Source: Rosen's Emergency Medicine, NKF Primer)
🔵 MANAGEMENT
Q17. What are the three goals of treatment in hypernatremia?
A.
- Correct underlying shock/hypovolemia - give isotonic (0.9%) saline FIRST if hemodynamically unstable
- Treat the underlying cause (e.g., fever, DI, vomiting)
- Carefully lower serum Na+ by replacing the free water deficit
(Source: Rosen's Emergency Medicine)
Q18. What is the rate of correction of hypernatremia?
A. This is a very common viva question!
| Situation | Rate |
|---|---|
| Acute hypernatremia (<24 hrs, e.g., salt loading) | Rapid correction: 1 mEq/L/hr decrease is relatively safe |
| Chronic/unknown duration | Max 0.5 mEq/L/hr, or 10-12 mEq/L/day |
| Chronic hypernatremia (>48-72 hrs) | Even more cautious: 5-8 mEq/L/day |
Why? Rapid correction → brain cells (which have accumulated idiogenic osmoles) now face a hypo-osmolar environment → cerebral edema → seizures → permanent neurological damage → death
(Source: Washington Manual, Schwartz's Principles of Surgery, Rosen's)
Q19. What fluids do you use in treatment?
A.
| Situation | Fluid of Choice |
|---|---|
| Hemodynamic instability / severe hypovolemia | 0.9% Normal Saline (isotonic - restores volume first) |
| After stabilization / free water replacement | 5% Dextrose (D5W) or 0.45% NS (half-normal saline) or 0.225% NS (quarter-normal saline) |
| Mild cases with intact GI | Oral water / NG free water (preferred route!) |
Oral water is ALWAYS preferred when feasible - it is the most physiological route.
Q20. How do you treat specific types?
A.
- Hypovolemic hypernatremia: NS first to restore volume, then switch to hypotonic fluids for water deficit
- Central DI: DDAVP (desmopressin) 1-2 mcg IV/SC - acts as ADH analog
- Nephrogenic DI: Low Na+ diet + thiazide diuretics (induce mild volume depletion → enhanced proximal tubule reabsorption → reduced urinary free water loss)
- Hypervolemic hypernatremia (salt loading): Stop the sodium source; give D5W; loop diuretics if needed
🔵 COMPLICATIONS & PROGNOSIS
Q21. What are the complications of hypernatremia?
A.
- Neurological: Seizures, coma, subarachnoid hemorrhage, permanent brain damage
- Metabolic: Hyperglycemia (inhibits insulin), impaired lactate clearance
- Cardiac dysfunction
- Increased mortality: Hospital-acquired hypernatremia with Na+ >150 mEq/L carries a severity-adjusted relative risk of death of 2.6x
- Increased length of hospital stay
Q22. What is the significance of hospital-acquired hypernatremia?
A. It is frequently underappreciated and under-treated:
- Fewer than 50% of patients with hospital-acquired hypernatremia receive free water replacement within 24 hours
- Patients whose hypernatremia is corrected within 72 hours have lower mortality than those corrected later
- It should NEVER be treated as incidental or negligible
(Source: NKF Primer on Kidney Diseases, 8th Ed.)
🔵 HIGH-YIELD VIVA POINTS SUMMARY
| Point | Key Fact |
|---|---|
| Definition | Na+ > 145 mEq/L |
| Always reflects | Hyperosmolar state |
| Must have | Impaired thirst OR no access to water |
| Most common type | Hypovolemic (free water loss > Na+ loss) |
| Brain effect | Shrinkage → cerebral vein rupture → SAH |
| Urine in DI | Dilute (< 300 mOsm/L) |
| Urine in impaired intake | Concentrated (> 600 mOsm/L) |
| Acute correction rate | Up to 1 mEq/L/hr |
| Chronic correction rate | ≤ 0.5 mEq/L/hr or 10-12 mEq/day |
| Danger of rapid correction | Cerebral edema, seizures |
| Central DI treatment | DDAVP |
| Nephrogenic DI treatment | Low Na diet + thiazide |
| Acute Na >160 mortality | ~75% |
Sources: Rosen's Emergency Medicine; Frameworks for Internal Medicine; NKF Primer on Kidney Diseases 8e; Washington Manual of Medical Therapeutics; Symptom to Diagnosis 4e; Sabiston Textbook of Surgery; Comprehensive Clinical Nephrology 7e
This is a shared conversation. Sign in to Orris to start your own chat.