Discuss management of spontaneous csf rhinorrhea in a middle aged female. Ms ent University exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"spontaneous CSF rhinorrhea" AND "management"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material for a full 20-mark answer. Let me compose the complete university exam answer.
Management of Spontaneous CSF Rhinorrhea in a Middle-Aged Female
MS ENT University Examination - 20 Marks
Introduction (2 marks)
Spontaneous cerebrospinal fluid (CSF) rhinorrhea refers to the egress of CSF through the skull base into the nasal cavity without any preceding trauma or iatrogenic cause. The term "spontaneous" is best reserved for cases of true idiopathic CSF rhinorrhea where comprehensive investigations fail to reveal a specific cause. It accounts for approximately 4% of all CSF leaks. It has a strong predilection for obese, middle-aged women - a demographic that closely mirrors that of benign intracranial hypertension (BIH / idiopathic intracranial hypertension / pseudotumor cerebri).
Why Middle-Aged Obese Women? - Pathophysiology (3 marks)
The demographics are not coincidental. Multiple lines of evidence link spontaneous CSF rhinorrhea in this group to occult elevated intracranial pressure (ICP):
- ICP link: Schlosser et al. showed that ALL patients undergoing lumbar puncture after successful endoscopic repair of nontraumatic CSF rhinorrhea had elevated ICP (mean 26.5-32.5 cm H2O). The leak itself acts as a pressure release valve, so ICP may appear falsely normal while the patient is actively leaking.
- BIH / Idiopathic Intracranial Hypertension (IIH): BIH is defined as elevated ICP in the absence of intracranial masses, hydrocephalus, or dural sinus thrombosis. Features include headache, pulsatile tinnitus, papilledema, visual disturbances, and abducens palsy. In one study, 82% of spontaneous CSF leak patients had an elevated BMI (average 36.2).
- Empty Sella Syndrome (ESS): A statistically significantly greater incidence of empty sella is found in nontraumatic vs. traumatic CSF leak patients. It is proposed that pulsatile CSF pressure transmission erodes the sella turcica floor and thins the skull base.
- Lateral Lamella of Cribriform Plate (LLCP): A long LLCP represents a thin region of the skull base susceptible to pressure erosion. Combined with elevated ICP, this creates a vulnerable point for CSF fistula formation.
- Multifactorial: The combination of bony skull base thinning + elevated ICP (from BIH/ESS) + female sex + obesity creates the clinical phenotype of spontaneous CSF rhinorrhea in middle-aged women.
Classification of CSF Rhinorrhea (1 mark)
(Box 48.1 - Cummings Otolaryngology)
| Type | Subtypes |
|---|---|
| I. Traumatic | A. Accidental (immediate/delayed); B. Surgical (post-neurosurgical or rhinologic) |
| II. Nontraumatic | A. Elevated ICP (neoplasm, hydrocephalus, BIH); B. Normal ICP (congenital, skull base tumor, erosive process) |
| III. Spontaneous/Idiopathic | No identifiable cause after full workup |
Clinical Features / Diagnosis (3 marks)
History
- Unilateral watery nasal discharge - characteristically clear, profuse, unilateral
- Positional variation - rhinorrhea worsens on head-down position (e.g., bending to tie shoes) - the "reservoir sign"
- Salty/metallic taste
- Headache that improves when rhinorrhea occurs (ICP decompressed by the leak) and worsens when rhinorrhea stops - highly characteristic of idiopathic CSF rhinorrhea
- History of recurrent bacterial meningitis (suggests persistent skull base defect)
- Symptoms of BIH: pulsatile tinnitus, visual obscurations, papilledema headache
Physical Examination
- Endoscopic examination may reveal a watery bead at cribriform plate, roof of ethmoid, or sphenoid sinus
- "Halo sign" on filter paper (CSF spreads further than blood forming a halo) - unreliable
- Evidence of papilledema on fundoscopy
Laboratory Confirmation of CSF
- Beta-2 transferrin (β2TF) - Gold standard. A protein exclusive to CSF, perilymph, and vitreous humor. High sensitivity (97%) and specificity (99%). Requires only 0.5 mL fluid.
- Beta-trace protein (BTP) - Prostaglandin D2 synthase; high sensitivity and specificity; useful adjunct
- Glucose testing - Historically used (CSF glucose >30 mg/dL), but unreliable due to contamination from nasal secretions
- Halo test - Unreliable; not recommended
- Intrathecal fluorescein (0.1 mL of 10% fluorescein diluted to 10 mL with CSF, given intrathecally) - used intraoperatively to identify leak site under blue-light endoscopy
Radiological Localization
Localization is the second essential step after confirming CSF presence.
| Modality | Role |
|---|---|
| High-resolution CT (HRCT) skull base | Bony defect localization; best for cribriform plate, ethmoid roof, sphenoid; sensitivity ~90% for active leaks |
| MRI (T2W/CISS/FIESTA) | Identifies meningoencephaloceles; superior soft tissue; complements CT |
| CT cisternography | Intrathecal contrast + CT; useful for active leaks; invasive; best sensitivity for active leaks |
| MR cisternography | Non-invasive; uses heavily T2W sequences; does not require intrathecal contrast |
| Radionuclide cisternography | Useful for slow/intermittent leaks; low sensitivity for localization |
| Intrathecal fluorescein + endoscopy | Most accurate intraoperative localization |
Management Strategy
The management of spontaneous CSF rhinorrhea is governed by the flowchart below:
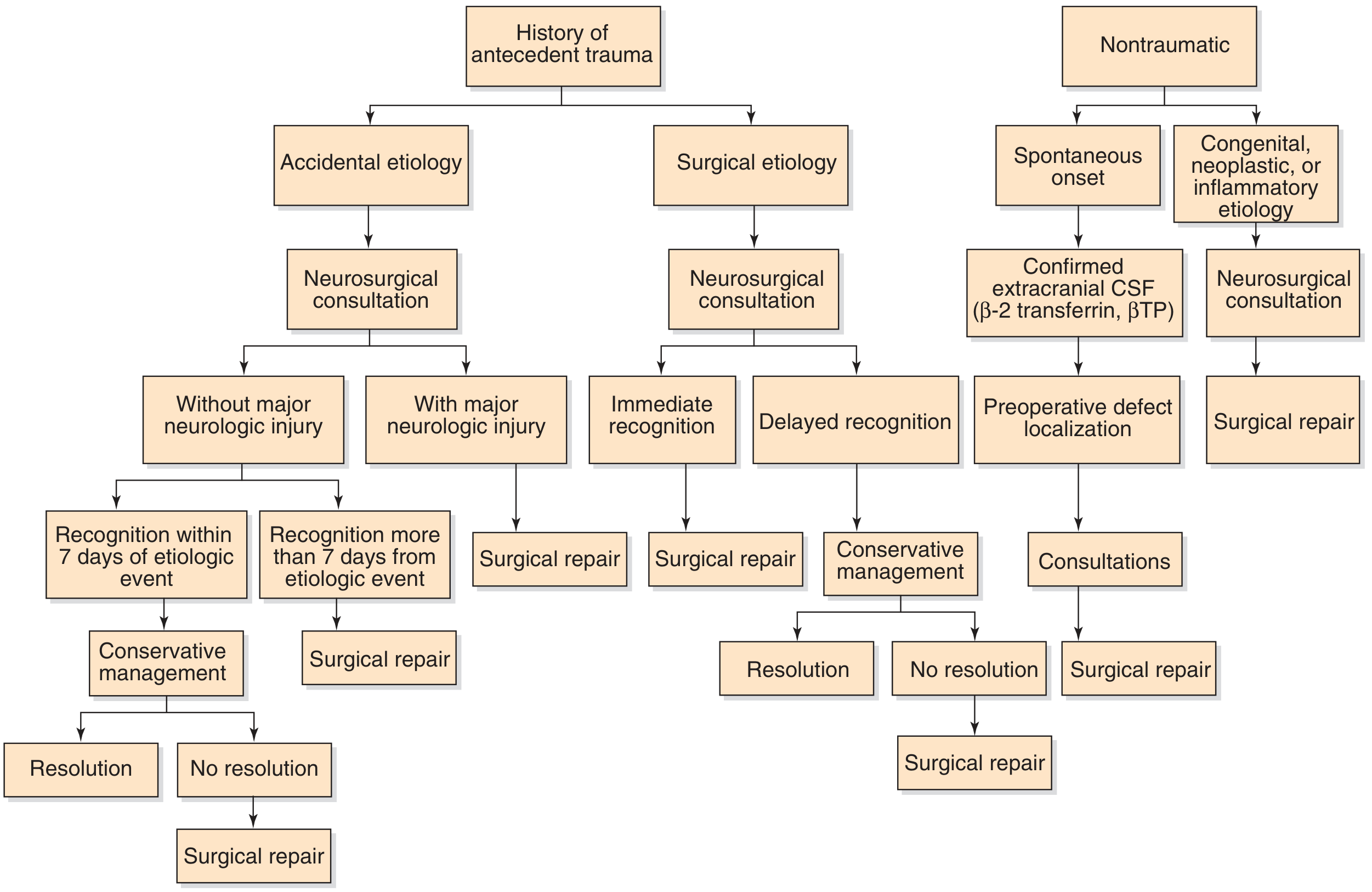
For spontaneous (nontraumatic) leaks in a middle-aged female, the pathway is:
- Confirm CSF (β2TF / BTP) → Localize defect (HRCT + MRI) → Specialist consultations → Trial of conservative management → Surgical repair if conservative treatment fails or is contraindicated
A. Conservative (Non-Surgical) Management (2 marks)
Reserved for acute presentations and as a trial before surgery in spontaneous leaks:
| Measure | Rationale |
|---|---|
| Strict bed rest with head elevation (30°) | Reduces ICP and CSF flow to defect |
| Lumbar subarachnoid drainage (catheter) | Decompresses ICP; 10 mL/hr preferred; daily CSF cell count, glucose, protein, culture |
| Avoid nose blowing, sneezing, straining, Valsalva | Prevents transient ICP spikes |
| Stool softeners | Avoids straining-related ICP elevation |
| Serial spinal taps (alternate if no lumbar drain) | Reduces CSF volume and ICP |
| Prophylactic antibiotics | Controversial - not routinely recommended; first-generation cephalosporin reasonable for lumbar drain site; evidence is weak |
| Pneumococcal, Hib, meningococcal immunization | Reduces risk of meningitis through skull base defect |
Lumbar drain caution: Avoid in markedly elevated ICP (risk of brainstem herniation). Monitor for low ICP (headache, pneumocephalus). Risk of meningitis must be weighed.
In traumatic leaks presenting within 7 days, conservative management is the first-line approach (>85% of traumatic leaks resolve spontaneously within 1 week). Spontaneous leaks have a much lower rate of spontaneous resolution and most require surgical repair.
B. Multidisciplinary Consultations (1 mark)
- Ophthalmology - formal assessment for papilledema (ICP marker)
- Neurosurgery - co-management; consider VP shunt / LP shunt if persistent elevated ICP
- Neuroradiology - imaging and cisternography
- Endocrinology - if empty sella present on MRI (pituitary dysfunction evaluation)
- Infectious disease - if meningitis is suspected; antibiotic selection
C. Surgical Management (6 marks)
Surgery is indicated for spontaneous CSF rhinorrhea when:
- Conservative management fails (no resolution after 1-2 weeks)
- Recurrent meningitis
- Meningoencephalocele through defect
- Large or persistent skull base defect
- Most spontaneous leaks - surgical repair is often the primary treatment given low spontaneous resolution rates
1. Endoscopic (Transnasal) Repair - Primary Technique
Since the initial descriptions in the 1980s, endoscopic endonasal repair has become the gold standard for surgical management of skull base CSF fistulae, replacing open intracranial approaches.
Steps of Endoscopic Repair:
- Preoperative intrathecal fluorescein: 0.1 mL of 10% fluorescein in 10 mL CSF given 30-60 minutes before surgery via lumbar puncture; blue-light endoscopy identifies leak site intraoperatively
- Endoscopic exposure: Standard functional endoscopic sinus surgery (FESS) to expose the skull base. 0° scope initially, then 30° for skull base visualization.
- Defect identification: Identified by fluorescein pooling under blue light or clear fluid welling
- Defect preparation:
- Remove residual bony partitions around the defect to create a flat surface
- Strip sinus mucosa 5 mm around the defect margin (denuded bone essential for graft adherence)
- Any meningoencephalocele present must be treated with bipolar cautery/Coblation (radiofrequency) - never pushed intracranially
- Graft selection and placement:
| Graft Type | Notes |
|---|---|
| Fascia lata | Most popular autograft; reliable |
| Temporalis fascia | Smaller harvest; good for small defects |
| Abdominal fat | For selected defects (especially sphenoid) |
| Free mucosa (middle turbinate / nasal floor) | Reliable, readily available |
| Pedicled middle turbinate flap | Higher failure rate than free grafts; used in selected cases |
| Acellular dermal allograft (AlloDerm) | Off-the-shelf option |
| Xenogeneic collagen dural substitutes (Durepair, Dura-Gen) | Scaffold for native fibroblast ingrowth; useful for large defects |
| Free cartilage / bone (nasal septum, calvarium) | For structural support |
A meta-analysis of 289 CSF fistulae (Hegazy et al.) found that the choice of grafting material does NOT significantly alter outcomes - technique of placement is more important.
- Underlay vs. overlay technique:
- Underlay (intradural): Graft placed beneath the dura, intracranially; good for larger defects
- Overlay (extradural): Graft placed over the defect on the nasal side; suitable for most spontaneous leaks
- Multilayer: Combination - a fascial underlay + cartilage/bone support layer + mucosal overlay; preferred for large defects and high-flow leaks
- Tissue sealant: Fibrin glue applied over graft to secure position
- Packing: Absorbable collagen-based packing ± non-absorbable nasal pack placed to support graft
Success rates: Endoscopic repair achieves >90% success on first attempt for spontaneous leaks (superior to intracranial approaches which have failure rates >25%).
2. Open (Intracranial) Approaches - Now Rarely Used
- Frontal craniotomy: Required for cribriform plate and ethmoid roof defects; provides direct access but involves brain retraction
- Extended craniotomy / skull base approaches: For sphenoid sinus and posterior skull base defects
- Drawbacks: Brain compression, hemorrhage, seizures, anosmia; failure rates >25%; largely replaced by endoscopic techniques
- Reserved for: failed endoscopic repair, very large defects, concurrent intracranial pathology, or areas not accessible endoscopically
3. Extradural Extracranial (External) Approaches - Historical
- Transseptal, transethmoidal, transsinus approaches via external incision
- Largely replaced by endoscopic techniques
D. Management of Elevated ICP - Critical in Middle-Aged Women (2 marks)
This is the most important aspect specific to spontaneous CSF rhinorrhea in middle-aged obese females, distinguishing it from traumatic leaks.
Failure to address elevated ICP leads to recurrent CSF leak even after technically successful surgical repair.
Options for long-term ICP management:
| Intervention | Details |
|---|---|
| Weight reduction | Most important - obese women with BIH; sustained weight loss reduces ICP |
| Acetazolamide (Diamox) | Carbonic anhydrase inhibitor; reduces CSF production by 50%; first-line medical therapy for BIH; 250-1000 mg/day |
| Furosemide | Alternative/adjunct diuretic for ICP reduction |
| Lumbar peritoneal (LP) shunt | For refractory elevated ICP; CSF diverted from lumbar subarachnoid space to peritoneum |
| Ventriculoperitoneal (VP) shunt | If hydrocephalus present or LP shunt not feasible |
| Optic nerve sheath fenestration | If threatened vision from papilledema |
A single surgical repair of the CSF fistula without addressing the underlying elevated ICP results in high recurrence rates. Postoperative ICP management is mandatory in spontaneous CSF rhinorrhea.
E. Postoperative Care (1 mark)
- Head elevation (30°) maintained
- Strict avoidance of nose blowing, sneezing, straining for 4-6 weeks
- Stool softeners continued
- Lumbar drain may be continued 3-5 days postoperatively for large defects
- Nasal packing removed at 5-7 days
- Prophylactic antibiotics: controversial but a first-generation cephalosporin is commonly given perioperatively
- Continued acetazolamide for BIH
- Follow-up ophthalmology for papilledema resolution
- Post-op CT head to exclude intracranial complications
- Meningitis vaccination if not already given
Complications (1 mark)
| Complication | Notes |
|---|---|
| Meningitis | Most feared; Streptococcus pneumoniae most common pathogen; vaccinate |
| Pneumocephalus | Air through skull base defect; tension pneumocephalus is life-threatening |
| Anosmia | From cribriform plate manipulation |
| Recurrence | More common if elevated ICP not treated |
| Orbital injury | Medial wall breach during endoscopic repair |
| Intracranial bleeding | Rare with endoscopic technique |
Summary Table - Key Exam Points
| Parameter | Key Fact |
|---|---|
| Demographics | Middle-aged, obese, female = overlap with BIH/IIH phenotype |
| Gold standard lab test | Beta-2 transferrin (β2TF) |
| Imaging of choice | HRCT + MRI skull base |
| Intraoperative localization | Intrathecal fluorescein + endoscopy |
| First-line surgical treatment | Endoscopic endonasal repair (>90% success) |
| Most critical adjunct in spontaneous leaks | ICP management (acetazolamide / LP shunt / weight loss) |
| Failure cause #1 | Untreated elevated ICP → recurrence |
| Open surgery failure rate | >25% |
References:
- Cummings Otolaryngology Head and Neck Surgery, 6th Ed., Chapter 48 (CSF Rhinorrhea)
- K.J. Lee's Essential Otolaryngology, 11th Ed.
- Mughal Z et al. "Outcomes of Endoscopic Management of Spontaneous Cerebrospinal Fluid Rhinorrhea: A Meta-Analysis." Laryngoscope, 2026 Jan. [PMID: 40650638]
Recent Evidence Note: A 2026 meta-analysis (PMID: 40650638) on endoscopic management of spontaneous CSF rhinorrhea confirms high success rates for endoscopic repair, consistent with current standard-of-care recommendations.
Discuss bondy's modified radical mastoidectomy. Ms ent University exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from both Shambaugh and Cummings. Let me now compose the complete 20-mark university exam answer.
Bondy's Modified Radical Mastoidectomy
MS ENT University Examination - 20 Marks
1. Introduction and Historical Background (2 marks)
Mastoid surgery evolved over more than a century in response to chronic suppurative ear disease. The pivotal milestones are:
- 1873 - Schwartze and Eysell: Described simple cortical mastoidectomy for acute mastoiditis
- 1890 - Zaufal: Expanded the concept to include removal of the posterior canal wall, tympanic membrane, and lateral ossicular chain - the classical radical mastoidectomy
- 1910 - Gustav Bondy: Recognized that when disease is limited to the pars flaccida and epitympanum, it is unnecessary to sacrifice the middle ear. He described opening only the epitympanum and externalizing the cholesteatoma while leaving the uninvolved tympanic membrane, ossicular chain, and mesotympanum intact - this became the Bondy's Modified Radical Mastoidectomy (BMRM). His 1910 description was one of the first in mastoid surgery to address hearing function.
- 1938 - Lempert: Popularized the use of a drill and loupe magnification
- 1953 onwards: Introduction of the operating microscope and canal-wall-up (CWU) mastoidectomy by Jansen
The term "modified radical mastoidectomy" is frequently (incorrectly) used interchangeably with canal-wall-down mastoidectomy. Classically, modified radical mastoidectomy refers specifically to the Bondy procedure.
- Cummings Otolaryngology Head and Neck Surgery, Ch. 143
- Shambaugh Surgery of the Ear, Ch. 31
2. Definition (1 mark)
Bondy's Modified Radical Mastoidectomy is a surgical procedure in which:
- Disease limited to the epitympanum (pars flaccida cholesteatoma, attic disease) is exteriorized by removing portions of the adjacent superior and posterior canal wall
- The middle ear (mesotympanum) is NOT entered
- The tympanic membrane and ossicular chain are preserved - the cholesteatoma matrix on the lateral surface of the ossicular heads is maintained in place as a lining for the created cavity
- A meatoplasty is performed to facilitate cavity access and cleaning
- This differs from retrograde mastoidectomy in that the defects of the canal and tympanic membrane are NOT repaired
3. Comparison with Related Procedures (1 mark)
| Feature | Cortical (Simple) Mastoidectomy | Bondy's MRM | Canal-Wall-Down (Modified Radical) | Radical Mastoidectomy |
|---|---|---|---|---|
| Canal wall | Preserved | Superior/posterior wall removed | Completely removed | Completely removed |
| TM | Intact | Intact | Reconstructed | Removed |
| Ossicles | Intact | Preserved (matrix left) | Stapes left; reconstruction possible | Removed |
| Middle ear | Not entered | Not entered | Sealed / reconstructed | Obliterated |
| ET | Patent | Patent | Patent | Obliterated |
| Primary aim | Exenterate air cells | Exteriorize attic disease | Eradicate disease + preserve function | Eradicate all disease |
| Hearing | Preserved | Preserved | Variable | Lost |
4. Indications for Bondy's Modified Radical Mastoidectomy (2 marks)
Classic Indications:
- Cholesteatoma strictly limited to the epitympanum (pars flaccida / attic cholesteatoma) with an intact ossicular chain - the ideal and primary indication
- Small attic cholesteatoma where disease has NOT extended into the mesotympanum, antrum, or mastoid
- Patients unwilling or unable to undergo the two-stage canal-wall-up (CWU) technique
- Situations where follow-up for a second-stage procedure is impractical (patient factors, geographic inaccessibility)
- The occasional otologic surgeon when confronted with attic cholesteatoma, as the technique is less demanding than staged CWU mastoidectomy
Contraindications / When NOT to Choose Bondy's:
- Cholesteatoma extending beyond the epitympanum into the antrum, mastoid, or mesotympanum
- Anterior epitympanic disease extending to the tensor fold or into the protympanum
- Labyrinthine fistula
- Extensive erosion of vital structures (facial nerve, labyrinth, dura)
When Conservative Management is Contraindicated and Surgery is Mandatory:
- Radiographic enlargement of a smooth-walled antrum (large cholesteatoma cavity)
- Persistent otorrhea despite cleaning
- Very small attic perforation making cleaning painful and unsatisfactory
- Cholesteatoma behind the pars tensa
- Signs of erosion of vital structures (facial canal, semicircular canals, cochlea, dura)
- Conductive or sensorineural hearing loss indicating cholesteatoma progression
- Intracranial complications
5. Preoperative Assessment (1 mark)
- Microscopic examination: meticulous cleaning of the ear; identify extent of attic perforation
- HRCT temporal bones: defines bony erosion; scutum erosion with attic soft tissue mass is diagnostic of attic cholesteatoma; evaluates semicircular canals, cochlea, tegmen plate, facial canal, sigmoid sinus
- MRI with gadolinium: adjunct when tegmen erosion is present - identifies meningoencephalocele, dural inflammation; MR angiography for suspected sigmoid sinus thrombosis
- Assess Eustachian tube function - functional ET is prerequisite for hearing preservation
- Preoperative audiogram (pure tone + tympanogram)
- Control active infection preoperatively: 1.5% acetic acid irrigations + antibiotic otic drops for several weeks; oral fluoroquinolones (10-14 days) for extensive mucosal infection
6. Surgical Technique (7 marks)
Anesthesia and Preparation
- General anesthesia
- Povidone-iodine preparation of external canal, auricle, and postauricular area
- 1% lidocaine with 1:100,000 epinephrine injected into postauricular region and ear canal for hemostasis
Step 1 - Incision
Postauricular approach (preferred):
- C-shaped postauricular incision placed ~1 cm behind the postauricular crease (facilitates closure)
- Plane developed between subcutaneous tissue and temporalis muscle / mastoid periosteum
- Areolar tissue and temporalis fascia harvested and set aside to dry (for grafting)
- T-shaped incision in soft tissue over mastoid: horizontal superior to temporal line through temporalis muscle; vertical incision down to mastoid tip
- Mastoid bone exposed using Lempert elevator
- Vascular strip (tympanomeatal flap incisions in canal) elevated and reflected anteriorly
Endaural approach (historical/Shambaugh):
- Two incisions from "12 o'clock" at the incisura terminalis: one along posterior canal wall to "6 o'clock", the second extending superiorly
- Periosteum elevated widely over entire mastoid; self-retaining (Shambaugh) endaural retractor inserted
Step 2 - Atticotomy (The Defining Step of Bondy's Procedure)
- Exposure of the bone above and behind the meatus, from posterior zygomatic root to 2-3 cm posterior to the spine of Henle
- Atticotomy with a cutting bur: outer cortex removed just above and behind the meatus over a semilunar area
- As the groove deepens, the pink color of the middle fossa dura is watched for
- The groove between the dura and superior meatal wall is deepened toward the notch of Rivinus
- Cholesteatoma debris and matrix in the lateral epitympanum are encountered
- If the cholesteatoma is confined to the epitympanum and lateral to the ossicles: the disease is exteriorized without entering the middle ear
Step 3 - Limited Cavity Bondy Technique (when ossicular chain intact)
- Limited intact canal wall procedure is performed, staying superior in the dissection
- Antrum is identified; lateral semicircular canal identified as landmark
- Superior and posterior canal wall removed until only a thin rim of bone remains over the ossicles
- A medium-sized bur drawn medially to laterally facilitates bone removal
- The final rim of bone is removed with a small curette - avoids traumatizing the intact ossicular chain
- The cholesteatoma matrix on the lateral surface of the ossicular heads (malleus head, incus body) is left in situ as a lining for the created cavity
- With experience, this can be performed entirely from the canal side ("inside out"), creating the smallest possible cavity
The key distinguishing principle of Bondy's procedure: The middle ear is NOT entered; the tympanic membrane and ossicular chain are preserved; the cholesteatoma matrix is retained as a cavity lining.
Step 4 - Identifying Key Landmarks During Bone Work
- Temporal line (tegmen): marks the middle fossa floor - stay below to avoid dural injury
- Lateral semicircular canal (LSSC): identifies the depth of the antrum; key safety landmark
- Facial nerve (vertical/mastoid segment): identified by the digastric ridge and LSSC; the facial ridge is NOT taken down as extensively in Bondy's as in MRM
- Sigmoid sinus: posterior limit
- Anterior buttress: where posterior canal wall meets the tegmen
- Posterior buttress: where posterior canal wall meets the floor of EAC lateral to facial nerve
Step 5 - Cavity Formation
- The resultant cavity is smaller than full CWD mastoidectomy since only the attic region is exteriorized
- The cavity should approach an ovoid or rectangular shape with no ledges
- Copious irrigation used to reduce bacterial count and aid hemostasis
- The cholesteatoma matrix is left as the epithelial lining of the lateral epitympanic cavity
Step 6 - Meatoplasty (Essential Step)
- 1% lidocaine with 1:100,000 epinephrine infiltrated into conchal bowl
- Posterior aspect of conchal bowl exposed with sharp dissection
- Semilunar incision into posterior conchal cartilage - a crescent-shaped piece (~1.5 × 2 cm) removed
- Creates a large meatus to allow:
- Visualization and cleaning of the mastoid cavity
- Adequate aeration of the cavity
- Epithelialization
Meatoplasty is mandatory - without an adequate meatus, the cavity will accumulate debris and become infected. An inadequate meatoplasty is a major cause of cavity problems.
Step 7 - Closure
- Cavity lined with Gelfoam or packing
- Postauricular wound closed in layers
- Mastoid dressing applied

7. Goals / Objectives of the Operation (1 mark)
The three fundamental objectives of Bondy's and related radical procedures are:
- Eradicate disease: Remove all bone-invading cholesteatoma safely
- Exteriorize the cavity: Create an accessible, exteriorized cavity amenable to lifelong periodic cleaning and surveillance
- Promote epithelialization: Encourage healthy skin/epithelial coverage of the cavity
- Preserve hearing: Unlike the radical mastoidectomy, Bondy's specifically aims to preserve the intact ossicular chain and middle ear function
8. Why is Bondy's Limited? The Shortcoming Addressed by Full MRM (1 mark)
The limitation of Bondy's procedure is its limited dissection of the canal wall and mastoid region:
- Peripheral mastoid air cells are isolated from the Eustachian tube
- If mucosa continues to produce mucus, it discharges into the mastoid cavity causing persistent otorrhea
- Results in recurrent cholesteatoma or persistent aural discharge from subsequent infection of remaining mastoid air cells
This led to the evolution of the full Modified Radical Mastoidectomy (canal-wall-down mastoidectomy + tympanoplasty), in which:
- The posterior canal wall is completely removed (addressing Bondy's shortcoming)
- Tympanoplasty is added to seal the middle ear space and eliminate drainage from exposed middle ear mucosa
- Hearing, however, remains a secondary consideration in the full MRM
- A dry, self-cleaning mastoid cavity can be maintained in 95% of cases
9. Postoperative Care and Follow-up (1 mark)
- Mastoid dressing removed at 24-48 hours
- Ear canal packing/Gelfoam removed at 2-4 weeks
- Lifelong periodic cavity cleaning is mandatory - the key obligation of all canal-wall-down procedures
- The cavity must be cleaned at regular intervals (typically every 6-12 months) at an otology clinic under microscopy
- Patients advised to keep the ear dry - water exposure causes caloric vertigo and infection
- Earplugs for bathing/swimming
- Annual audiometry
- Watch for:
- Residual/recurrent cholesteatoma (keratin pearls - occur in 5-6% of cases; usually treatable in-office)
- Cavity infection / granulation tissue
- Cavity problems (see below)
10. Complications (2 marks)
Intraoperative Complications:
| Complication | Cause / Prevention |
|---|---|
| Facial nerve injury | Failure to identify the vertical segment; confused with tegmen; use digastric ridge + LSSC as landmarks |
| Labyrinthine fistula | Drilling too close to semicircular canals; leave matrix over blue line |
| Dural exposure/tear | Working too close to tegmen |
| Sigmoid sinus injury | Posterior dissection too aggressive |
| Ossicular chain damage | Curette or drill trauma while taking down the last rim of bone over ossicles in Bondy's |
| Cholesteatoma matrix tear | Incomplete removal; seeding of residual cells |
Postoperative Complications:
| Complication | Notes |
|---|---|
| Residual / recurrent cholesteatoma | Most important; keratin pearls; requires vigilant follow-up |
| Cavity problems (wet, discharging cavity) | Due to inadequate meatoplasty, sump trap effect, or persistent mucosa |
| Sump trap / "sink trap" effect | When mastoid tip extends below level of bony canal floor - creates a pocket that collects debris; prevented by lowering mastoid tip cells lateral to digastric ridge |
| Caloric vertigo | Water entering large cavity triggers caloric stimulation |
| Facial nerve palsy | Immediate (intraoperative) or delayed (edema, infection) |
| Sensorineural hearing loss | Drill trauma, labyrinthine fistula disturbance |
| Persistent conductive hearing loss | Ossicular disruption, middle ear problems |
| Wound infection / mastoiditis | Rare |
| Meningitis / intracranial complications | More likely if disease was already extradural |
Causes of a "Bad Cavity" (Problem Cavity):
- Inadequate meatoplasty - meatus too small for adequate ventilation and cleaning
- High facial ridge - obscures the hypotympanum and sinus tympani from view
- Anterior and posterior buttress not removed - creates ledges
- Mastoid tip sump trap - mastoid floor lower than EAC floor
- Persistent mucosa - mucus-producing mucosa not adequately exteriorized
- Residual air cells - especially retrofacial cells that continue to discharge
11. Summary: Key Exam Points (1 mark)
| Parameter | Fact |
|---|---|
| Described by | Gustav Bondy, 1910 |
| Primary indication | Attic/pars flaccida cholesteatoma limited to the epitympanum |
| Defining principle | Middle ear NOT entered; TM and ossicles preserved; cholesteatoma matrix left as cavity lining |
| What is removed | Superior and posterior canal wall (limited); attic disease exteriorized |
| What is preserved | Tympanic membrane, ossicular chain, mesotympanum |
| Essential step | Meatoplasty (mandatory) |
| Key landmark | Lateral semicircular canal (depth of antrum); digastric ridge (facial nerve) |
| Key shortcoming | Residual mastoid air cells isolated from ET → persistent discharge / recurrent cholesteatoma |
| Evolution from Bondy's | Full MRM (complete removal of posterior canal wall + tympanoplasty) |
| Cavity self-cleaning rate (full MRM) | 95% |
| Epithelial pearl recurrence | 5-6% |
References:
- Shambaugh Surgery of the Ear, 6th Ed., Chapter 31 (Modified Radical Mastoidectomy) and Chapter on Technique of Radical and Bondy MRM
- Cummings Otolaryngology Head and Neck Surgery, 6th Ed., Chapter 143 (Mastoidectomy)
- K.J. Lee's Essential Otolaryngology, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.