Give me a detailed understanding on spinal tracts and what happens when there is tumor ressecetion from cervicomedullary to d2 region what will be the management, what gets affected how to treat, manage and what will be the physiotherapy
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
cervicomedullary to D2 spinal tumor resection neurological deficits management physiotherapy rehabilitation
Reading File
Finding Sources
Finding Sources
Searching PubMed
intramedullary spinal cord tumor resection cervical thoracic outcome
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, detailed answer. Let me compile it.
Spinal Tracts, Cervicomedullary-to-D2 Tumor Resection: Complete Clinical Guide
PART 1: SPINAL TRACTS - DETAILED ANATOMY
Here is the cross-sectional layout of all major spinal tracts:
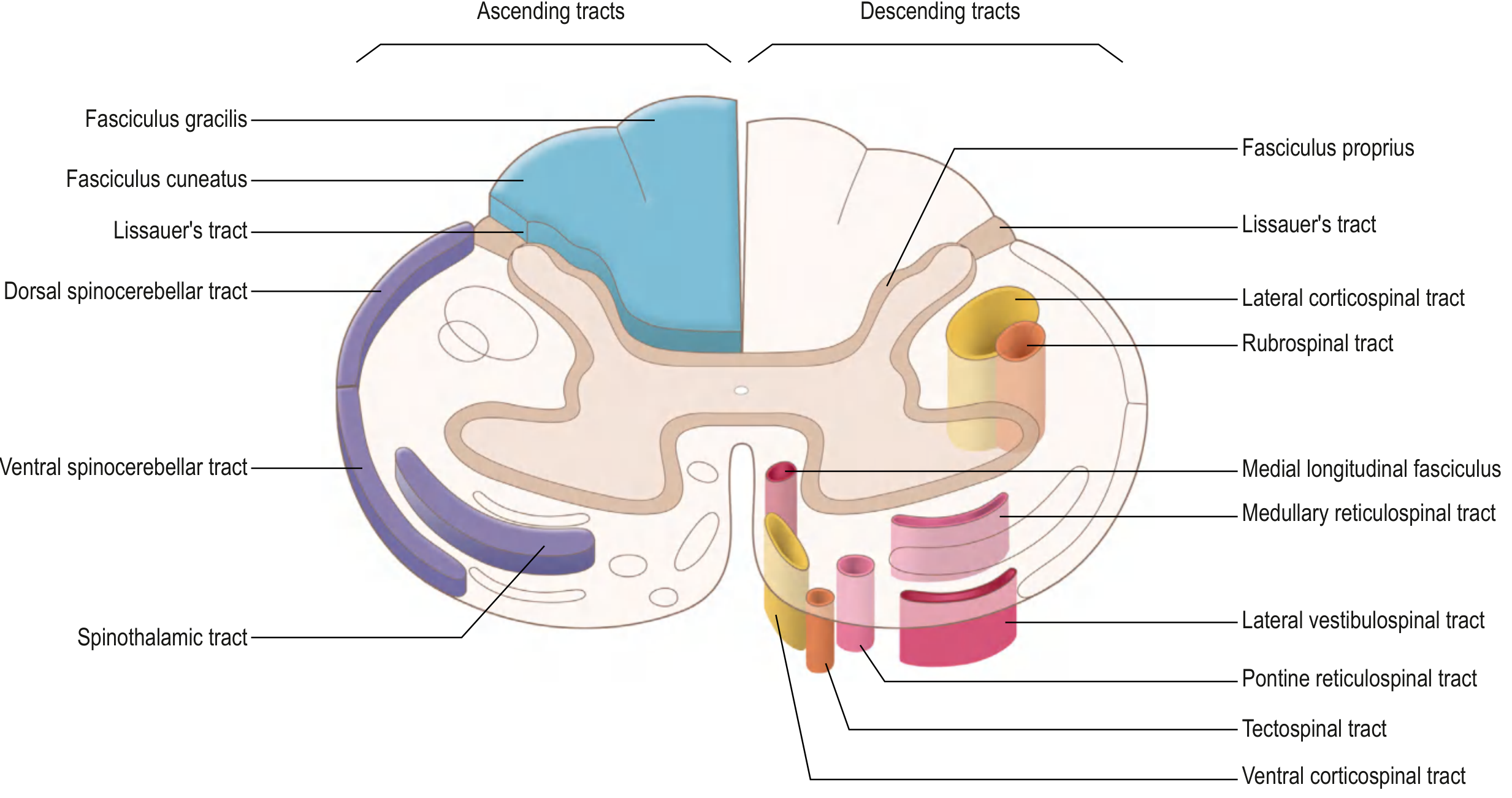
A. ASCENDING (Sensory) Tracts
1. Anterolateral / Spinothalamic Tract
-
Location: Anterolateral funiculus (contralateral, after crossing)
-
Carries: Pain, temperature, crude touch
-
Pathway:
- 1st-order neuron: Dorsal root ganglion → enters posterior horn
- Collaterals ascend/descend 1-2 levels in Lissauer's tract before synapsing (laminae I and V)
- 2nd-order neuron: Crosses obliquely in anterior commissure within 2-3 segments → ascends contralaterally as spinothalamic tract
- Synapse at ventral posterior lateral (VPL) nucleus of thalamus
- 3rd-order neuron: Projects via posterior limb of internal capsule → primary somatosensory cortex
-
Clinical pearl: Pain/temperature loss occurs contralateral, starting 1-2 segments below the lesion level
-
Spinoreticular tract: Same origin, but projects to reticular formation (emotional/arousal aspect of pain)
-
Spinomesencephalic tract: Projects to periaqueductal gray and superior colliculus (central pain modulation)
2. Posterior Column - Medial Lemniscal Pathway
- Location: Posterior (dorsal) funiculus, ipsilateral
- Carries: Fine/discriminative touch, vibration, conscious proprioception
- Sub-components:
- Fasciculus gracilis (medial): lower limbs and trunk (below T6)
- Fasciculus cuneatus (lateral): upper limbs and neck (above T6 - relevant in cervicomedullary region)
- Pathway:
- 1st-order neuron: Dorsal root ganglion → ascends ipsilaterally to caudal medulla
- Synapse: Nucleus gracilis / nucleus cuneatus in caudal medulla
- 2nd-order neuron: Crosses as internal arcuate fibers → forms medial lemniscus (contralateral medulla)
- Ascends to VPL thalamus
- 3rd-order neuron: → Primary somatosensory cortex
- Clinical pearl: Loss of proprioception, vibration sense, and fine touch ipsilateral to the lesion
3. Spinocerebellar Tracts (Subconscious proprioception)
- Dorsal spinocerebellar tract: Ipsilateral, from Clarke's nucleus (C8-L3), enters cerebellum via inferior cerebellar peduncle
- Ventral spinocerebellar tract: Bilateral, enters cerebellum via superior cerebellar peduncle
- Function: Coordination, postural regulation - damage causes ipsilateral ataxia
B. DESCENDING (Motor) Tracts
1. Lateral Corticospinal Tract (Lateral Motor System)
- Location: Lateral funiculus (posterior part)
- Carries: Voluntary movement, especially fine skilled movements of distal limbs
- Pathway:
- Upper motor neuron: Primary motor cortex → corona radiata → posterior limb of internal capsule → crus cerebri → pons (small bundles) → forms medullary pyramid
- At caudal medulla: ~90% decussate → lateral corticospinal tract (contralateral)
- ~10% stay ipsilateral → anterior corticospinal tract (cervical + upper thoracic levels)
- Synapse: Lower motor neurons in lateral anterior horn
- Clinical pearl: Upper motor neuron signs - ipsilateral weakness, spasticity, hyperreflexia, extensor plantar response (Babinski)
2. Rubrospinal Tract (Lateral Motor System)
- Origin: Red nucleus (midbrain)
- Crosses in ventral tegmental decussation → descends in lateral column
- Function: Limb movement modulation (complementary to corticospinal)
3. Medial Motor System Tracts
| Tract | Origin | Function |
|---|---|---|
| Anterior corticospinal tract | Motor cortex (uncrossed 10%) | Axial/proximal muscles |
| Vestibulospinal tract (lateral) | Lateral vestibular nucleus | Antigravity muscles, postural tone |
| Reticulospinal tracts (pontine + medullary) | Pontine/medullary reticular formation | Posture, gait, spinal reflex modulation |
| Tectospinal tract | Superior colliculus | Head/neck orientation to visual stimuli |
| Medial longitudinal fasciculus | Multiple brainstem nuclei | Coordinates head-eye movements, neck reflexes |
C. Somatotopic Organization in the Spinal Cord
In the lateral corticospinal and spinothalamic tracts, fibers are arranged somatotopically:
- Cervical fibers: medial (innermost)
- Sacral fibers: lateral (outermost)
This is clinically important: an intramedullary expanding lesion (like a tumor) affects cervical fibers first; an extramedullary lesion compresses sacral fibers first (producing "sacral sparing" in intramedullary lesions).
PART 2: WHAT HAPPENS DURING CERVICOMEDULLARY-TO-D2 TUMOR RESECTION
The Affected Region
The cervicomedullary junction (C0-C2) to D2 (T2) spans:
- The lower medulla and upper cervical cord
- The entire cervical enlargement (C3-C8) - which controls the brachial plexus and upper limb function
- The upper thoracic cord (T1-T2)
Tumors in this region are commonly:
- Intramedullary: Ependymoma (most common adult IMSC tumor), astrocytoma, hemangioblastoma
- Extramedullary intradural: Meningioma, schwannoma, neurofibroma
- Extradural: Metastases, primary bone tumors
Tracts and Structures Affected
| Structure Disrupted | Functional Loss |
|---|---|
| Bilateral lateral corticospinal tracts | Quadriplegia / tetraplegia (UMN type: spastic, hyperreflexic) - upper and lower limbs |
| Bilateral spinothalamic tracts | Loss of pain and temperature sensation bilaterally below the lesion |
| Posterior columns (fasciculus cuneatus + gracilis) | Loss of vibration, proprioception, fine touch bilaterally below the lesion |
| Cervical enlargement (anterior horn) | LMN lesion to upper limbs - flaccid weakness, wasting, fasciculations of upper limbs (C5-T1 segments) |
| T1 sympathetic fibers | Horner syndrome (ptosis, miosis, anhidrosis) - if T1 is disrupted |
| Phrenic nerve origin (C3-C5) | Respiratory compromise - particularly dangerous at cervicomedullary level |
| Cervicomedullary junction (medullary centers) | Autonomic instability: Blood pressure, heart rate dysregulation; respiratory center involvement |
| Spinocerebellar tracts | Ataxia, coordination deficits |
| Propriospinal tracts | Disruption of segmental reflexes |
PART 3: CLINICAL SYNDROMES THAT CAN RESULT
Post-resection, the patient may present with one or more of these syndromes depending on extent and location:
1. Central Cord Syndrome
- Most common incomplete cord syndrome
- Affects central gray matter and lateral corticospinal tract
- Upper extremities worse than lower extremities (because cervical fibers lie medially)
- Sacral sensation preserved (sacral fibers in outermost position)
- Bladder dysfunction common (urinary retention)
2. Brown-Séquard Syndrome (Hemisection)
- Ipsilateral: Motor loss + loss of vibration/proprioception (posterior column)
- Contralateral: Loss of pain and temperature (spinothalamic, crossed)
- Best prognosis among incomplete syndromes
3. Anterior Cord Syndrome
- Disruption of anterior spinal artery territory
- Loss of motor function + pain/temperature bilaterally below the lesion
- Proprioception and vibration preserved (posterior columns spared)
- Worst prognosis for recovery
4. Posterior Column Syndrome
- Loss of vibration, proprioception, fine touch
- Motor and pain/temperature relatively preserved
5. Cervicomedullary Syndrome (Specific to this level)
- Upper and lower limb weakness (quadriparesis)
- Respiratory compromise
- Autonomic instability
- Lower cranial nerve involvement possible (IX, X, XI, XII) if resection extends to medulla
- Ipsilateral arm > leg weakness sometimes seen
PART 4: WHAT GETS AFFECTED - SYSTEMATIC DEFICITS CHECKLIST
Motor
- Upper limbs (C3-T1): Combination of UMN (spastic weakness from corticospinal tract damage) + LMN (flaccid, wasted from anterior horn destruction at C5-T1)
- Lower limbs: UMN pattern - spastic paraparesis/paraplegia (corticospinal tract damage above T2)
- Loss of intercostal muscle function (T1-T2) → reduced forced expiratory volume, impaired cough
Sensory
- Pain and temperature loss: Bilateral, contralateral if asymmetric resection, starting 1-2 levels below surgery
- Proprioception/vibration loss: Ipsilateral to lesion (if asymmetric), bilateral if complete
- May have a "cape-like" sensory dissociation (loss of pain/temp over shoulders and arms but intact proprioception) - classic for central cord/syrinx
Respiratory
- Critical at cervicomedullary level: C3-C5 damage → phrenic nerve palsy → diaphragm weakness → ventilator dependence
- Upper thoracic damage (T1-T2) → loss of intercostal contribution to breathing
Autonomic
- Neurogenic shock immediately post-op (hypotension + bradycardia due to loss of sympathetic tone)
- Autonomic dysreflexia (in chronic phase, lesions above T6): Massive sympathetic response to noxious stimuli below the lesion - hypertensive crisis, headache, sweating, bradycardia
- Neurogenic bladder: Spastic bladder if suprasacral (UMN) - detrusor hyperreflexia, urge incontinence, incomplete emptying
- Bowel dysfunction: Constipation, fecal incontinence, loss of voluntary sphincter control
- Sexual dysfunction: Erectile dysfunction, loss of orgasm, fertility issues
- Thermoregulation impairment: Inability to sweat/shiver below level of lesion
Temperature regulation, DVT Risk, Skin
- Loss of protective sensation → pressure ulcers
- Immobility + venous stasis → deep vein thrombosis (major risk)
- Impaired thermoregulation
PART 5: ACUTE & SURGICAL MANAGEMENT
Immediate Post-Operative Phase
Neurological monitoring:
- Intraoperative neurophysiological monitoring (IONM) - motor evoked potentials (MEPs), somatosensory evoked potentials (SSEPs), and D-wave monitoring. Changes on IONM guide the surgeon to modify technique and predict outcome.
- Neurological examination Q2-4 hours immediately post-op
Respiratory:
- ICU monitoring mandatory for all cervicomedullary resections
- Early intubation/ventilatory support if respiratory compromise (C3-C5 damage → phrenic involvement)
- Respiratory function tests (FVC, MIP, MEP)
- Avoid excessive sedation; promote early weaning trial
Cardiovascular:
- Hemodynamic monitoring in ICU
- Mean arterial pressure (MAP) >85-90 mmHg target to maintain spinal cord perfusion pressure
- Vasopressors (norepinephrine preferred) for neurogenic hypotension
- Atropine/pacemaker on standby for neurogenic bradycardia
Methylprednisolone:
- Controversial in surgical cord injury; many centers avoid routine use post-operatively due to surgical site complications
Spinal stability:
- Cervical orthosis (rigid collar or halo vest) if stability is compromised post-resection
- Hard cervical collar typically for 6-12 weeks if laminectomy performed without fusion
Medical Complications Prevention
| Complication | Prevention/Treatment |
|---|---|
| DVT/PE | LMWH (usually started 48-72h post-op), sequential compression devices, early mobilization |
| Pressure ulcers | Turn every 2 hours, pressure-relieving mattress, skin checks |
| Urinary tract infection | Clean intermittent catheterization (preferred over Foley), monitor urine culture |
| Autonomic dysreflexia | Identify and remove noxious stimulus (blocked catheter, impacted bowel), nifedipine/nitrates for acute episode |
| Neuropathic pain | Pregabalin, gabapentin; tricyclics (amitriptyline); opioids as last resort |
| Spasticity (subacute/chronic) | Baclofen (oral or intrathecal), tizanidine, physiotherapy |
| Heterotopic ossification | Etidronate (controversial), early ROM exercises |
PART 6: PHYSIOTHERAPY MANAGEMENT - PHASE BY PHASE
Phase 1: Acute ICU/Immediate Post-Op (Day 1-7)
Goals: Prevent complications, maintain joint range, initiate neurological recovery
-
Respiratory physiotherapy
- Manual assisted cough (MAC) and assisted bagging for secretion clearance
- Incentive spirometry
- Positioning for lung expansion (head-of-bed elevation 30°)
- Airway suction coordination
- Mechanical insufflator-exsufflator (Cough Assist) if cough is weak
-
Positioning
- Proper alignment of spine at all times
- Log-roll technique for position changes with cervical precautions
- Anti-spasticity positioning: Avoid hip/knee flexion contracture position
- Arm resting splints if wrist drop is present
-
Passive Range of Motion (PROM)
- All joints of upper and lower limbs through full ROM to prevent contractures
- Gentle cervical PROM only once cleared by neurosurgeon
- Ankle foot orthoses (AFOs) in neutral position to prevent equinus
-
Sensory stimulation
- Tactile stimulation over affected areas
- Proprioceptive input to limbs
Phase 2: Subacute Rehabilitation (Week 2-12)
Goals: Strengthen preserved muscles, early mobility, functional independence
Neurological Level: C3-C8 / T1-T2 affected (expected functional outcomes per Bailey & Love):
| Level | Expected Physiotherapy Functional Goals |
|---|---|
| C3-C4 | Power wheelchair control; ventilator weaning; communication with adaptive technology |
| C5 | Power wheelchair; assisted UL dressing; self-feeding with aids; some shoulder/elbow control |
| C6 | Manual wheelchair (possibly); wrist extension-assisted grip; driving with adaptations |
| C7 | Manual wheelchair independence; independent transfers; use of triceps for push-up relief |
| C8-T1 | Independent in most ADLs; bladder/bowel with assistance; independent manual wheelchair |
| T2 | Full upper-limb function; independent with all self-care; trunk stability partially impaired |
Key Interventions:
-
Active Assisted Range of Motion (AAROM) progressing to Active ROM (AROM)
- Use gravity-eliminated positions initially (side-lying, supported seated)
- Target muscles: deltoid, biceps, wrist extensors (C5/C6), triceps (C7), hand intrinsics (C8/T1)
-
Strengthening
- Preserved muscle strengthening: Theraband, free weights, pulleys
- Functional Electrical Stimulation (FES) to activate paralyzed muscles (prevents atrophy, facilitates neuroplasticity)
- Neuromuscular Electrical Stimulation (NMES) for muscle re-education
-
Respiratory rehabilitation
- Ventilatory muscle training (threshold inspiratory muscle trainer)
- Active cycle of breathing technique (ACBT)
- Glossopharyngeal breathing for ventilator-weaning support
-
Bed mobility training
- Rolling (log roll with cervical precautions initially)
- Supine-to-sit transfers
- Assisted sitting balance progressing to independent sitting
-
Transfer training
- Assisted transfers: Bed-to-wheelchair, wheelchair-to-toilet
- Sliding board transfers
- Stand-pivot transfers (for lower-level lesions)
-
Wheelchair prescription and training
- Power wheelchair (mouth/chin control) for C3-C4
- Power-assisted or manual wheelchair for C5-C6
- Manual wheelchair for C7 and below
- Pressure relief lifts every 15-30 minutes
-
Spasticity management (physiotherapy component)
- Sustained stretch, standing frame, tilt table
- Hydrotherapy/aquatic therapy - warm water reduces tone
- Vibration therapy
- Kinesio-taping
-
Sensory re-education
- Textured surfaces, temperature discrimination training
- Mirror therapy for central reorganization
- Graded sensory stimulation
Phase 3: Late Rehabilitation / Community Re-integration (3 months+)
Goals: Maximum functional independence, gait (if possible), community participation
-
Gait training (for incomplete lesions / T2 levels)
- Partial body weight-supported treadmill training (PBWSTT / Lokomat robotic therapy)
- Parallel bar walking progressing to walking aids
- Long leg braces (KAFOs) or short leg braces (AFOs) as appropriate
- Functional electrical stimulation cycling (FES-cycling) for lower limbs
-
Balance training
- Seated balance: trunk stabilization on unstable surfaces (balance boards, Swiss ball)
- Standing balance: parallel bars → crutches → forearm crutches
- Virtual reality-based balance training
-
ADL Training (with Occupational Therapy)
- Adaptive equipment: built-up utensils, button hooks, reachers
- Environmental modifications: ramps, grab rails, shower chairs
- Driving assessment and hand control adaptation
-
Pain Management
- TENS (Transcutaneous Electrical Nerve Stimulation) for neuropathic pain
- Heat/cold modalities (with extreme caution given sensory loss - MUST check temperature before application)
- Myofascial release for secondary musculoskeletal pain
-
Neuroplasticity-based training
- Task-specific repetitive training (most evidence-based approach)
- Constraint-induced movement therapy (CIMT) if one limb is more affected
- Body-weight support systems (Lokomat, ReWalk exoskeleton)
- Transcranial magnetic stimulation (TMS) or transcranial direct current stimulation (tDCS) as adjuncts
-
Cardiorespiratory fitness
- Arm ergometry
- FES-assisted cycling
- Aquatic exercise
-
Long-term monitoring
- Monitor for post-operative syringomyelia (ascending neurological deficit, cape-like sensory loss, worsening pain)
- Serial MRI at 6 months, 1 year, then annually
- Monitor for tumor recurrence, especially for ependymomas and astrocytomas
PART 7: MULTIDISCIPLINARY TEAM ROLES
| Specialist | Role |
|---|---|
| Neurosurgeon | Resection, stability assessment, post-op monitoring |
| Neurologist | Seizure management, neuropathic pain, electrophysiology (EMG/NCS) |
| Physiatrist | Rehabilitation prescription, spasticity management, bladder/bowel protocols |
| Physiotherapist | Motor retraining, respiratory, gait, balance, ADL |
| Occupational Therapist | ADL, adaptive equipment, upper limb function, home modifications |
| Speech Therapist | If cervicomedullary junction affects swallowing/vocal cord (X, XII) |
| Respiratory Therapist | Ventilator weaning, secretion clearance |
| Urologist | Neurogenic bladder management - UDS, CIC training, medications |
| Psychologist | Adjustment to disability, depression screening, cognitive rehabilitation |
| Dietitian | Nutritional support (hypermetabolic post-surgery; avoid constipation with high-fiber diet) |
| Orthotist/Prosthetist | Bracing - cervical collar, AFOs, KAFOs, hand splints |
| Social Worker | Discharge planning, community resources, caregiver training |
PART 8: KEY OUTCOME PREDICTORS
- Pre-operative neurological status - the most powerful predictor
- Completeness of resection - GTR (gross total resection) associated with better functional outcomes for ependymomas
- Histology - Ependymomas (WHO grade 2) best prognosis; astrocytomas more infiltrative, worse
- Level of injury - Higher cervical lesions have worse functional outcomes
- Age and comorbidities
- Intraoperative IONM data - D-wave preservation predicts long-term motor recovery even when MEPs are lost
- Duration of deficits before surgery - Shorter = better recovery potential
Summary: A cervicomedullary-to-D2 tumor resection creates a complex neurological picture involving the entire cervical spinal cord and upper thoracic cord. The key tracts affected are the lateral corticospinal tracts (causing spastic quadriplegia with UMN signs in legs and mixed UMN/LMN in arms), the spinothalamic tracts (bilateral pain/temperature loss), posterior columns (bilateral proprioception/vibration loss), and cervical anterior horn cells (LMN flaccid paralysis in upper limbs). Autonomic dysfunction including neurogenic bladder, bowel, and potentially life-threatening autonomic dysreflexia must be proactively managed. Physiotherapy follows a systematic phase-based approach: respiratory and positioning in the acute phase, progressive strengthening and mobility training in the subacute phase, and task-specific neuroplasticity-based rehabilitation in the late phase. The goal is always to maximize preserved neural function, prevent secondary complications, and restore the highest possible level of functional independence.
Sources: Gray's Anatomy for Students (9780323934237); Tintinalli's Emergency Medicine (9781260019933); Bradley & Daroff's Neurology in Clinical Practice (9780323642613); Bailey & Love's Short Practice of Surgery, 28th Ed. (9780367548117); Frameworks for Internal Medicine (9781496359308); Harrison's Principles of Internal Medicine 22E (9781265977061); Frontiers in Neurology IONM study; Farooqi et al. 2023 (PMID 36858296) - Systematic Review of IMSC Ependymomas
This is a shared conversation. Sign in to Orris to start your own chat.