Ring enhancing lesion of brain
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ring enhancing lesion" brain differential diagnosis
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Excellent. I now have very rich content. Let me compile the comprehensive answer.
Ring Enhancing Lesion of the Brain
A ring enhancing lesion (REL) on contrast CT or MRI appears as a hypodense/hypointense center surrounded by a peripheral rim of contrast enhancement, often with surrounding edema. The ring represents breakdown of the blood-brain barrier at the periphery of the lesion, while the center is avascular (necrosis, pus, or necrotic tumor core).
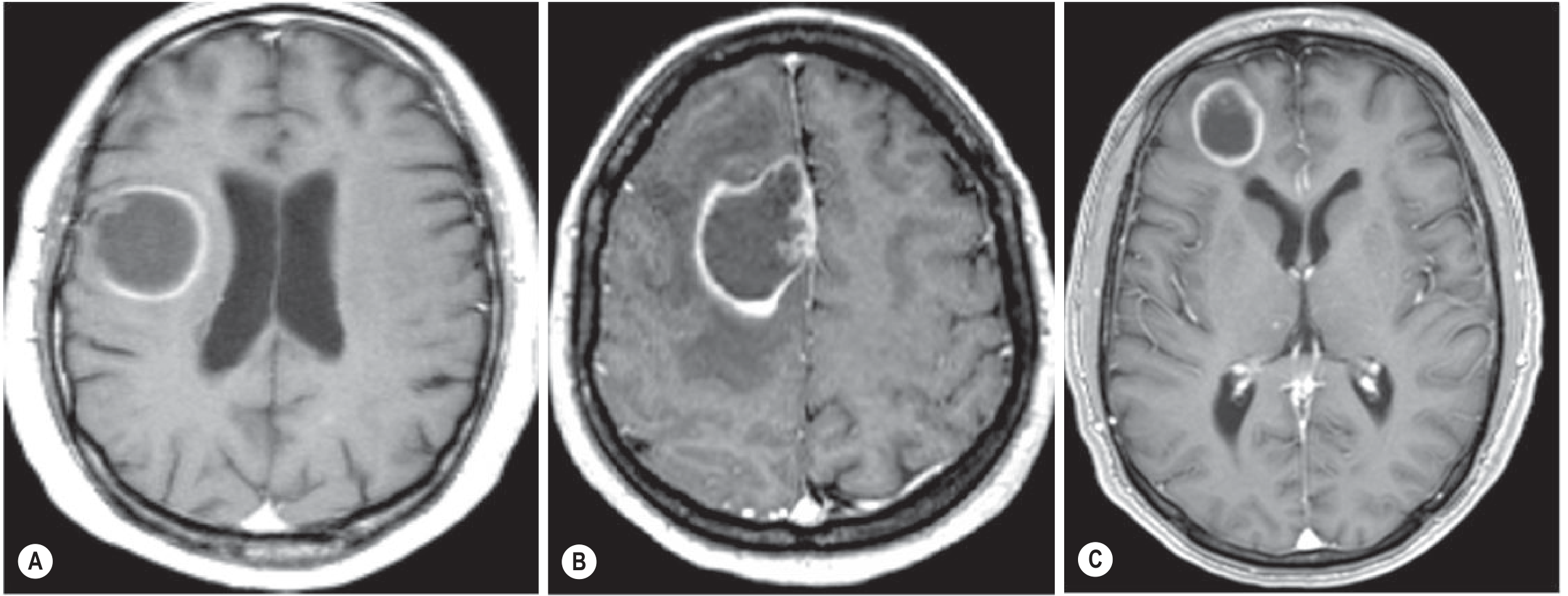
Contrast-enhanced T1 MRI: (A) Pseudotumoral MS lesion - note incomplete/open ring facing cortical grey matter; (B) Glioblastoma - complete ring enhancement; (C) Brain metastasis - complete ring enhancement. - Grainger & Allison's Diagnostic Radiology
Differential Diagnosis - The Classic Mnemonic: "MAGIC DR"
| Cause | Key Features |
|---|---|
| Metastasis | Most common cause in adults >45 yrs; often multiple; at grey-white junction; well-defined complete ring; known primary cancer |
| Abscess (bacterial) | Thin, smooth, complete ring; DWI restriction (bright on DWI) is key distinguishing feature; fever, leukocytosis; daughter abscess sign |
| Glioblastoma (GBM) | Thick, irregular ring; usually single; no DWI restriction; ring surrounds necrotic tumor core |
| Infarction (subacute) | Gyral/cortical enhancement; follows vascular territory; gyriform pattern |
| Contusion / hematoma (resolving) | History of trauma; evolving on serial imaging |
| Demyelination (MS - tumefactive) | Open/incomplete ring (open toward cortex); younger female; other MS lesions; perivenous |
| Radiation necrosis | History of prior RT; within radiation field; may be indistinguishable from recurrence |
Most Common Causes in Detail
1. Brain Abscess
The classic imaging is a thin, smooth, complete ring on gadolinium T1 MRI surrounding a central pus cavity.
- FLAIR: hypointense rim separating hyperintense core from surrounding edema
- DWI restriction (bright on DWI, dark on ADC map) is the hallmark - distinguishes abscess from tumor
- "Daughter abscess" sign: smaller ring-enhancing satellite lesion connected to the parent - highly suggestive of abscess
- The inner (deep) wall of the ring may be thinner than the outer wall
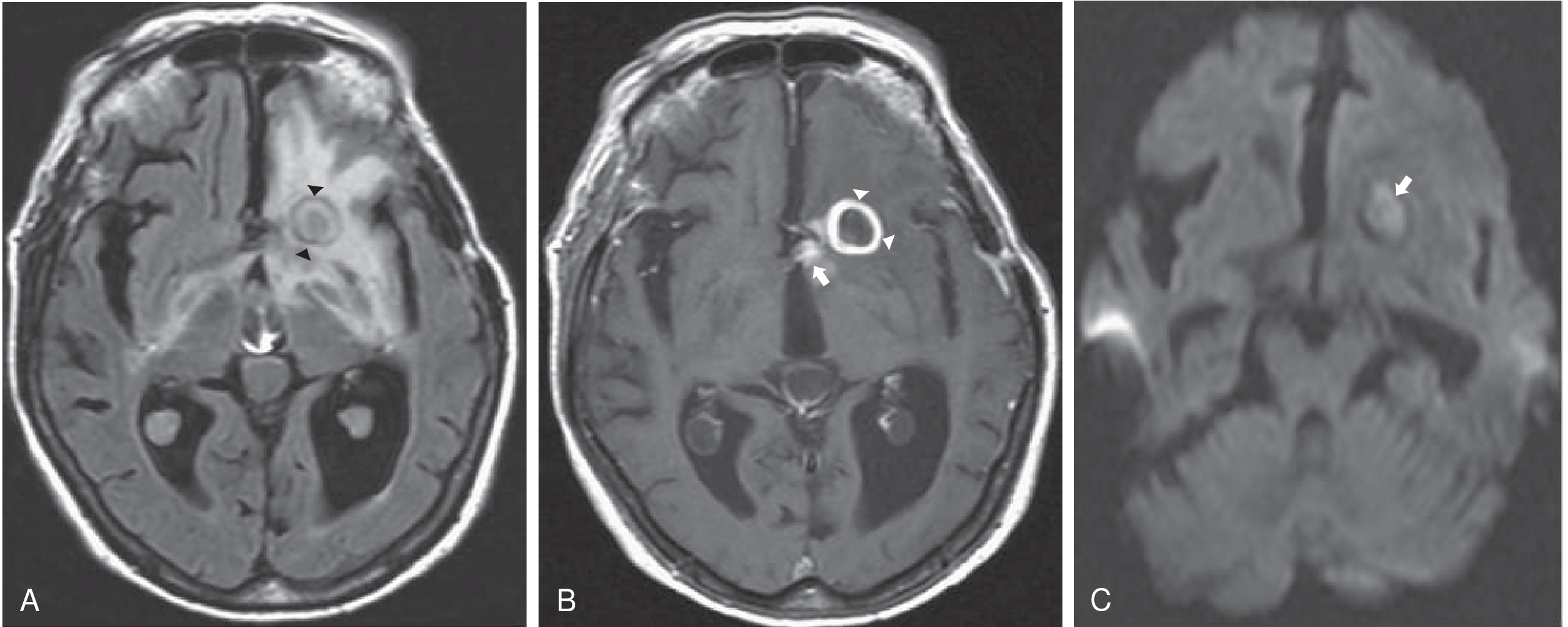
Cerebral Abscess: (A) FLAIR - round lesion with hypointense rim and surrounding edema; (B) T1+Gad - complete ring enhancement with surrounding cerebritis; (C) DWI - hyperintense cavity (restricted diffusion). - Bradley & Daroff's Neurology
Sources of brain abscess by location:
- Otogenic → temporal lobe or cerebellum; gram-negative rods
- Sinogenic/odontogenic → frontal lobe; anaerobic/microaerophilic streptococci
- Hematogenous → multiple, polymicrobial; anywhere in brain
- Post-neurosurgical/trauma → staphylococci
Treatment:
- Abscesses <2.5 cm with GCS >12 and known etiology: IV antibiotics alone
- Aspiration or excision for larger lesions, elevated ICP, or treatment failure
- Antibiotics per source (e.g., ceftriaxone + metronidazole for odontogenic/sinogenic)
2. Cerebral Toxoplasmosis (in AIDS/immunocompromised)
The most common CNS mass lesion in AIDS patients. Caused by reactivation of latent T. gondii (>95% have positive IgG).
- CD4 count <100 cells/mcL in 80%; risk highest at CD4 <50
- Multiple ring-enhancing lesions in 86%; single in 14%
- Located in grey matter: basal ganglia, thalamus, cortex
- On CT with contrast: single REL 35%, ≥2 lesions 62%
- A single lesion makes toxoplasmosis less likely and increases suspicion for Primary CNS Lymphoma (PCNSL)
Workup: Toxoplasma IgG (sensitivity ~95%); CSF PCR (54% sensitive, 99% specific); MRI preferred over CT
Management: Empirical pyrimethamine + sulfadiazine + leucovorin is standard first-line. If no response in 10-14 days, biopsy for PCNSL.
3. Primary CNS Lymphoma (PCNSL)
- Associated with HIV/AIDS and immunosuppression
- Often single lesion (in contrast to toxoplasmosis which is multiple)
- Periventricular location common
- May show homogeneous enhancement or ring enhancement
- Ring enhancement in PCNSL is less regular than abscess
- Responds to steroids (lesions may "vanish" on steroids - do not give steroids before biopsy)
4. Glioblastoma Multiforme (GBM)
- Thick, irregular ring surrounding central necrosis
- Usually single, large lesion
- No DWI restriction in the center (unlike abscess)
- Crosses corpus callosum ("butterfly glioma") in some cases
- Significant surrounding edema and mass effect
- Ring is complete even when it contacts cortical grey matter
5. Metastasis
- At the grey-white matter junction (emboli lodge here)
- Often multiple; known primary cancer (lung, breast, melanoma, renal, colon)
- Well-defined, complete ring; may have "halo" of disproportionate edema relative to lesion size
- Melanoma metastases may be T1 hyperintense (melanin/hemorrhage)
6. Tuberculomas
- Solid or ring-enhancing lesions, particularly at the grey-white junction
- Central T2 hypointensity (due to caseating necrosis) with ring enhancement
- Associated with basal meningitis, hydrocephalus, cranial nerve palsies
- HIV co-infection common in endemic regions
7. Neurocysticercosis
- Cystic ring-enhancing lesions with a central scolex (pathognomonic)
- Periventricular and subcortical locations
- Associated calcifications on CT in old/dead lesions
- Causes seizures in endemic populations
8. Tumefactive MS (Demyelination)
The radiological hallmark distinguishing it from glioblastoma/metastasis:
- Open ring (incomplete ring) - the open margin faces the cortical grey matter
- GBM and metastasis always show complete ring even when contacting cortex
- Younger patients, female predominance
- Other MS lesions visible on MRI; perivenular "Dawson finger" morphology
Imaging Approach to Differentiate RELs
| Feature | Abscess | GBM | Metastasis | Toxoplasmosis |
|---|---|---|---|---|
| Number | Usually 1 | Usually 1 | Often multiple | Usually multiple |
| Ring wall | Thin, smooth | Thick, irregular | Variable | Thin-moderate |
| DWI | Restricted (bright) | Low signal | Low signal | Variable |
| Location | Any | White matter | Grey-white junction | Basal ganglia, cortex |
| Edema | Moderate | Severe | Often disproportionate | Moderate-severe |
| Context | Fever, source of infection | Elderly, no fever | Known malignancy | HIV, CD4 <100 |
Key rule: DWI restriction (bright DWI + dark ADC) = abscess until proven otherwise.
Workup
- Contrast MRI brain - modality of choice; superior to CT
- DWI - essential for abscess vs tumor differentiation
- MR spectroscopy - elevated lipid/lactate in abscess; elevated choline in tumor
- HIV test + CD4 count - if positive, toxoplasmosis/PCNSL enter the differential
- Toxoplasma IgG/IgM serology
- Blood cultures, CBC, CRP/ESR
- Chest X-ray/CT - source of infection or primary lung malignancy
- LP only if safe (no raised ICP, no midline shift): CSF cytology, PCR, culture
- Stereotactic biopsy - when imaging cannot differentiate or patient fails empirical treatment
Sources:
- Bradley & Daroff's Neurology in Clinical Practice, Ch. 40 & 78
- Grainger & Allison's Diagnostic Radiology, Ch. 58 & 76
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed., Ch. 5 (Toxoplasmic Encephalitis)
- Tintinalli's Emergency Medicine, Ch. 174 (Brain Abscess)
This is a shared conversation. Sign in to Orris to start your own chat.